
ABSTRACT
The inequity of medical negligence-based adversarial litigation in the USA, UK and Australia is a recognised target for reform. Plaintiff autonomy is weakened by a dispute resolution system that has evolved around lawyers, opposed experts and indemnity insurers; the need to prove breach and causation excludes compensation for other categories of medical injury; and patient access to the system is restricted by high entry costs. Two strategies towards reform are raised here. A short-term approach involves routine initial use of a single court-appointed medical expert for assessment of errors and liabilities, thus improving access while relegating fault-finding to a reserve role. In the longer term, adversarial litigation could be replaced in part by a no-fault compensation scheme – such as in Scandinavia, France and New Zealand – funded by taxation and by re-directed medical indemnity fees. Reforms such as these would be challenging to implement, but are achievable, so it is not premature for relevant bodies to consider a timetable for action.
Introduction
Adversarial litigation has been practised for centuries,1 with its existence justified in part by the desire of plaintiffs to have their grievances considered, contested and, where appropriate, compensated.2,3 In the medical malpractice field, these motivations have limited the uptake of alternative (eg mediation-based) conflict resolution,4 which could in theory reduce costly defensive medicine5 and thus benefit societal needs, including healthcare affordability and safety.6,7 Indeed, calls for replacement of the adversarial system by a no-fault compensation scheme – already argued to be ‘long overdue’ a decade ago8 – go back at least 50 years.9 The recent 2022 House of Commons Report on NHS Litigation Reform by the Health and Social Care Committee provides a powerful reminder that this issue has not gone away.10
The present system depends on expert witnesses who are renowned for their experience in the matter of dispute, enabling assessment of negligence cases with high complexity and damage claims. As part of a push for tort reform over the last 30 years, the laws of evidence and procedure with respect to the giving of expert medical evidence have been deeply considered and debated in many common law jurisdictions.11 However, viewed in a real-world context of rising public expectations, how fit for purpose does this high-cost paradigm remain? And if reforms to the system are to be made, what specific short- and long-term options are there?
Opposed experts: a counsel of perfection
For legal appraisal of disputes involving specialised scientific or medical matters, expert advice is often vital. However, the involvement of opposed experts may make the (non-expert) judge's task more challenging.12 Furthermore, although adversarial procedures remain the gold standard for elucidating legal truths, numerous aspects of this approach have been criticised.13 For example, some have remarked of US-style medical litigation:
... the majority of patients experiencing adverse events will have no recourse through the system ... {whereas for others} the result is time and money spent on fruitless litigation that serves neither to compensate the injured patient nor improve the health care system.14
One cause of this disconnect between costs and benefits is that the adversarial system has evolved from different legal and medical needs. Tort law seeks, in retrospect, to enable restorative justice and/or recompense for individual plaintiffs.15 In contrast, medical peer-review seeks to identify harmful practices for future deterrence across the profession – even though there is little evidence that negligence per se is, or can be, deterred by legal means.10
From a plaintiff's perspective, the adversarial system provides no compensation for medical errors or damages which are deemed non-negligent, or which lack proof of proximate causation.16 These considerations may help explain why no-fault systems are experienced by plaintiffs to be fairer than fault-based systems, both in medical injury and other contexts.17,18
A strength of the present system is that its routine involvement of multiple experts and lawyers leads to careful deliberation and judgements which grant due weight to both sides of a dispute. Yet it is debatable whether all disputes necessitate quite such a resource-intensive, in-depth and high-cost approach. This raises the question whether dispute resolution could be improved for many patients by introducing system changes that permit greater flexibility.
The court-appointed expert: one small potential step for patient access
Although many expert witness codes forbid advocacy, critics have argued that this ideal is unlikely to be achieved when experts are paid by one party.19–21 In Australian negligence law these and other challenges were appraised in 2002 by the Ipp Panel.22 Recommendation 8, paras 3.70–79 of this review stated that, based on the Panel's ‘collective sense of fairness', system reform should be considered by implementing a three-year trial of court-appointed experts, given that:
In most jurisdictions there is deep dissatisfaction with expert evidence. There is a widespread perception that, in many instances, expert witnesses consciously or unconsciously slant their testimony to favour the party who retains them. Although this problem has for many years been recognised and discussed throughout the common law world it remains unresolved. Many experts become identified as plaintiffs' experts or defendants' experts.... {but still} there are some medical practitioners and lawyers who oppose any change to this system.22
Section 3.81 of this review proposed practical details for implementation of such a trial of court-appointed experts, with related costings. Fig 1 depicts how this system might work.
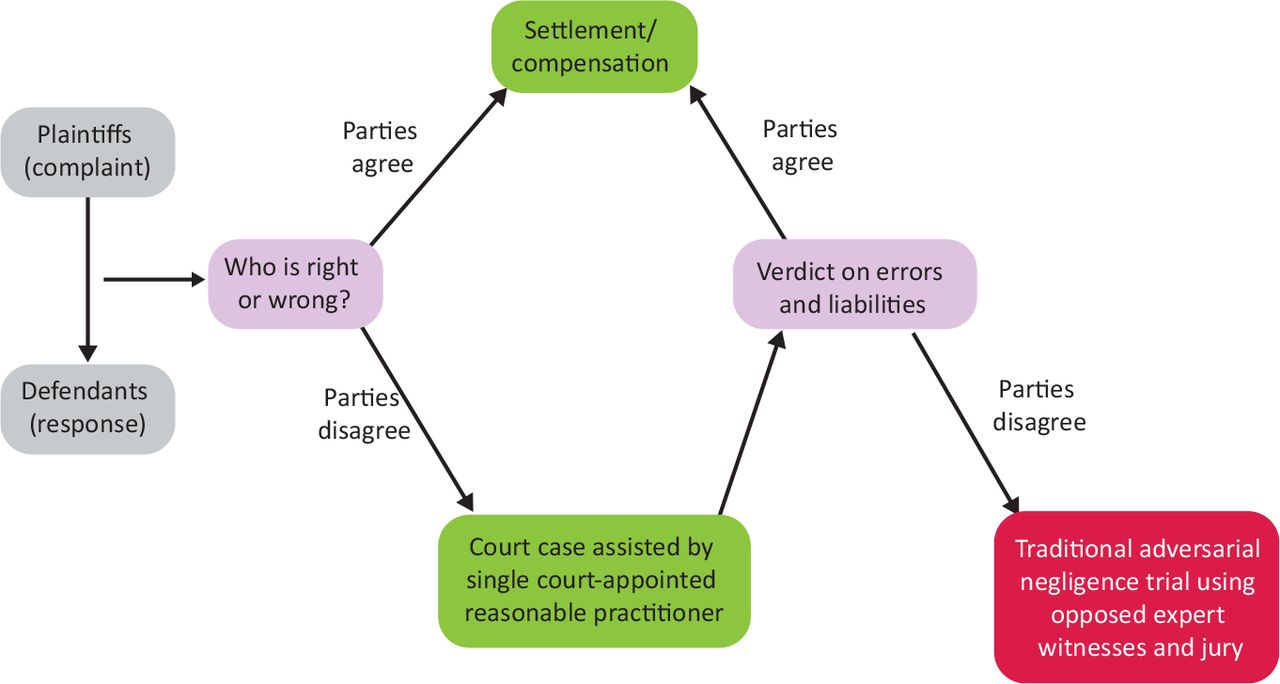
Workflow depicting how a centralised triage step could provide greater first-phase legal accessibility for patients of limited means, while reducing the number of costly trials requiring adversarial expert testimonies. The ‘reasonable practitioner’ specified in this schema represents an ‘expert’ who is deemed likely to provide a balanced view of errors and liabilities for the trial context.
A critical weakness of this approach relates to the perceived vulnerability of physician self-regulation systems to protective bias,23 with this being one of the more cogent justifications for the adversarial system. For this reason, use of a single court-appointed expert should best be considered an entry step in dispute resolution – albeit with the aim of satisfactorily concluding as many cases as possible – with other established options remaining open.
But it is arguable that the main factor perpetuating the modern adversarial medicolegal system is not an otherwise unmet need for multiple experts to ensure fair adjudications. Rather, the evolution in lockstep of medical defense organisations – which, through their receipt of medical insurance premiums, have come to monopolise the finances both for physicians' legal costs and patients' compensation – can be seen as the most challenging element of the status quo that would require restructuring in the event of future reform.
Medical indemnity insurers: the hidden persuaders
With the notable exception of plaintiffs,24 the adversarial malpractice system appears largely supported by all stakeholders: lawyers, doctors, governments and indemnity insurers. For lawyers, it eliminates uncertainties over the large costs of legal proceedings, which are defrayed via the premiums paid by all doctors to their insurers.25 For doctors, it relieves concerns that a practitioner could incur direct unreimbursed financial penalties for negligent acts, while it also deters many of their potential plaintiffs due to the substantial costs of private legal representation. For governments, it absolves them from the economic trauma of having to justify and set up new public alternatives such as tax-based no-fault compensation.
But for medical indemnity companies – uniquely among these stakeholders – adversarial litigation underpins the core business. For a patient seeking compensation in this system, the medical indemnity insurance industry is the sole financial source, and hence ‘the only game in town’. Moreover, like other insurance companies, these are businesses in their own right; they are not charities or public services, and so have no mission to support patient equity. In contrast to no-fault compensation schemes, the cumulative fiscal resources of the indemnity industry create a system imbalance that can deter plaintiffs, thus advantaging defendants and insurers alike (Fig 2). In addition, all physicians are encouraged by the indemnity culture to pursue defensive medicine – for example, carrying out excessive diagnostic testing (ie overservicing) to minimise risks of malpractice litigation – the main consequence of which is to disadvantage patients further by increasing the costs while reducing the benefits of their healthcare.26

Comparison of fault-based adversarial medical litigation (left) with no-fault compensation (lower right), illustrating (i) the imbalance of resources faced by plaintiffs in the former system, due in large part to the indemnity support for physician-defendants, and (ii) the less labour-intensive and more streamlined approach of the no-fault system.
These considerations highlight that the medical indemnity industry does not play a mere support role in the system; on the contrary, it is a veritable linchpin, and no reforms can plausibly take place without its cooperation. Implementation of a no-fault system would need to involve at least part-replacement of indemnity businesses – for example, with redeployment of staff into the government domain, and/or re-routing of malpractice premiums into a central fund, with or without additional support from employer levies. These complex transitions could require as long as one, two or even three decades of forward planning (eg in Australia, the UK or the USA, respectively), in turn raising the concern that ongoing bipartisan government support may not always be in place. Yet despite a slowing of reform by these systemic obstacles, there may be irresistible forces driven by technology which come to accelerate the pace of medicolegal change, irrespective of stakeholder preferences.
Clinical decision support software: a game-changer?
In the adversarial system, the role of the expert in negligence cases often comes down to their opinion as to whether or not a standard of reasonable care – often as defined by empirical studies or other evidence-based guidelines – was breached. In the future, however, many physicians' decisions may well be predicated upon advice provided in the background by clinical decision support softwares (CDSS) which are in turn based on artificial intelligence (AI). One motivating principle for this revolution will be that of improving patient safety and reducing physician error; yet despite these good intentions, adverse outcomes must still occur from time to time, leading to disputes over causation, foreseeability, avoidability and so on.
Differing possibilities are thus raised as to the impact of CDSS/AI on medical litigation. In the best of all possible worlds, CDSS will improve medical safety and outcomes to an extent that substantially reduces medical injuries or damage, thereby reducing litigation;27 if this vision is not fully realised, however, the legal impact of CDSS is harder to predict. If CDSS use comes to be equated with guideline adherence, akin to a Bolam-like guarantor of ‘reasonable care’, concerns over litigation may gradually persuade many clinicians to enmesh all decisions within a CDSS framework.28 Yet claims may continue to be raised by plaintiffs that any adversely-fated CDSS recommendation implemented by a physician remains, in hindsight, entirely ‘owned’ by (ie the onus of) that clinician, even if informed consent to the use of CDSS was signed. Conversely, defendants may claim, with some justification, that such evidence-based AI-guided decisions should have a mitigating effect (ie as a putative system error) on physician negligence judgements. Hence, assuming that CDSS software developers themselves are unlikely to be proven negligent, the expansion of AI could well drive the evolution of civil liability law towards a new system that focuses, more straightforwardly and achievably, on the financial management of losses – ie, no-fault.29,30
Fault lines of no-fault systems
Based on the experience of the countries mentioned above, introduction of a no-fault scheme is at least feasible as a commitment to a social good, and would seem unlikely to be replaced once implemented. Nonetheless, a frequent objection to no-fault systems relates to the fear that total costs may rise due to rising cases (‘opening the floodgates'10) – including, though not limited to, frivolous or vexatious complaints – from claimants who would hitherto have been discouraged by financial constraints. Despite this concern, some reports have suggested that costs may decline following introduction of no-fault compensation,31,32 especially if deterrence and compensation are separated;33 moreover, while it is very plausible that cases will increase, such a rise could also confirm an (intentional) improvement in system equity. Reassuringly, too, some published experiences have indicated that most additional no-fault cases are of high validity34 and minor severity,35 and that many of these have been associated with requests for accountability (eg prevention of future similar incidents, better explanations or apologies) rather than solely for compensation.36
There have long been calls for a medical liability system that not only compensates patients, but also holds physicians to account, while ensuring and improving medical safety,37 but this all-in-one goal appears to have been losing credibility over recent decades. The priority of a no-fault scheme must be to improve patient access to a fair hearing of their claims, and to compensation as indicated. Public agencies decoupled from the legal system could still be linked into these processes to ensure appropriate disciplinary assessment of physicians (eg healthcare complaints bureaux, and/or medical registration bodies) and to translate the insights gained into better patient safety across the healthcare sector (eg by ministries of health). If the imperfect reality proves to be that a blended tort/no-fault system is needed to pursue this wide set of goals,23 then such a compromise may well merit adoption.
Conclusion
The aphorism alluded to in the title of this article, attributed to Plutarch, is usually cited as, ‘Finding fault is easy, to do better is difficult’. In fact, Plutarch wrote:
...it is the easiest thing in the world to find fault with one's neighbour... and useless unless it be applied to correcting or avoiding similar faults.38
To many stakeholders it may seem ‘the easiest thing in the world’ to continue acceptance of the present fault-finding medical litigation system – notwithstanding that it is acknowledged to be inequitable, non-transparent, all-or-nothing, resource- and labour-intensive, subject to advocacy bias, encouraging of wasteful defensive medicine, and ineffective in deterring negligence. More positively, these same criticisms represent a recipe for ‘correcting or avoiding similar faults' via purposive design of a fairer and more constructive system. For example, the use of a single court-appointed expert to provide initial advice about errors and liabilities could, in one step, significantly reduce patient inequity, costs, and advocacy bias; while for doctors, too, such speedier dispute resolutions may well reduce stress and stigma.
There will remain complex cases that are best resolved by adversarial proceedings. However, the luxury of this option may not deserve its continuing mandate, and the opportunity costs of doing nothing could be rising. A no-fault system reform will be challenging to implement, making transitional strategies essential.22 Nonetheless, major benefits to legal accessibility and medical safety should flow from such reforms, making it desirable for representative institutions to work together and commit to planning towards this socially stabilising goal.
Acknowledgements
The author thanks Stephen Epstein SC for advice about the manuscript, and the family of Mr Frank Wolf for kind support.
- © Royal College of Physicians 2023. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.