
ABSTRACT
Unscheduled care is complex, particularly because many patients have multiple long term medical conditions. It is difficult to ensure the appropriate care is delivered by specialist services to patients in a timely manner. Lack of specialist input may impact on patient safety and adversely affect outcomes. We describe an automated email alerting system which was developed as result of a clinical incident. Using free software and minimal computing resources an automated email alerting system was developed. The system identified patient admissions, compared them against patient cohorts and created alerts. It used only around 1,000 lines of Java7 code combined with free software and secure NHS mail accounts. The system currently sends alerts to many different teams at our hospital. The patient population includes 6,047 patients on one of our 10 monitored lists or special registers. From May to June 2013 the system alerted to 863 monitored patient admissions in 2,158 separate messages. This system has been adopted across multiple specialties, has been well received and has had a direct impact on patient care. Not only is this system efficient and effective, but importantly can be implemented with low cost and complexity and is hence easily reproducible across the NHS.
Introduction
With the increasing processing power of computing devices, and the proliferation of the internet and mobile devices, there comes a change in our expectations of information delivery and communication in healthcare. Access to electronic information systems at the point of care has the potential to inform clinical decision-making, and improve efficiency, quality and safety.1,2
There have been several studies demonstrating effective use of information technology (IT) in healthcare, including reducing admissions to hospital, adverse clinical events and clinical errors, and also improving business efficiency and patient safety.3–8 However, even with these advances, healthcare professionals often do not have access to real-time patient information at the point of care.
This solution was implemented by a large organisation serving an approximate population of 750,000, with three acute hospital sites and many specialist services having inpatient services on only one site. This configuration for an acute provider is not unusual in England but does present challenges in terms of communication across the organisation, particularly in relation to non-elective admissions.
Here we present an example of a simple IT solution that is reproducible and deliverable across the NHS. We have developed a generic email admission alerting system that sends a message to a recipient group when a patient from a defined patient group is admitted onto the patient administration system (PAS). Within 2 minutes of the patient being admitted onto the PAS an email alert is sent to members of the specialist team, which may include consultants, specialist nurses and allied health professionals. This allows appropriate action following a patient admission, including patient-specific advice and, if necessary, clinical intervention ranging from a ward review by a member of the specialist team to patient transfer within the trust.
Methodology
Approval for use of data was sought from the informatics development group within the trust and the information governance group.
There are three main parts to the system:
Identifying patient admissions.
Comparing these admissions with cohorts of patients from specialist groups.
Informing the appropriate specialist team.
All of these have to be considered within the overall landscape of NHS IT, especially data security and patient confidentiality (Fig 1). Important aspects of this system and keys to its success are both its low cost and the simplicity of its development and implementation. With this simplicity also comes reliability.
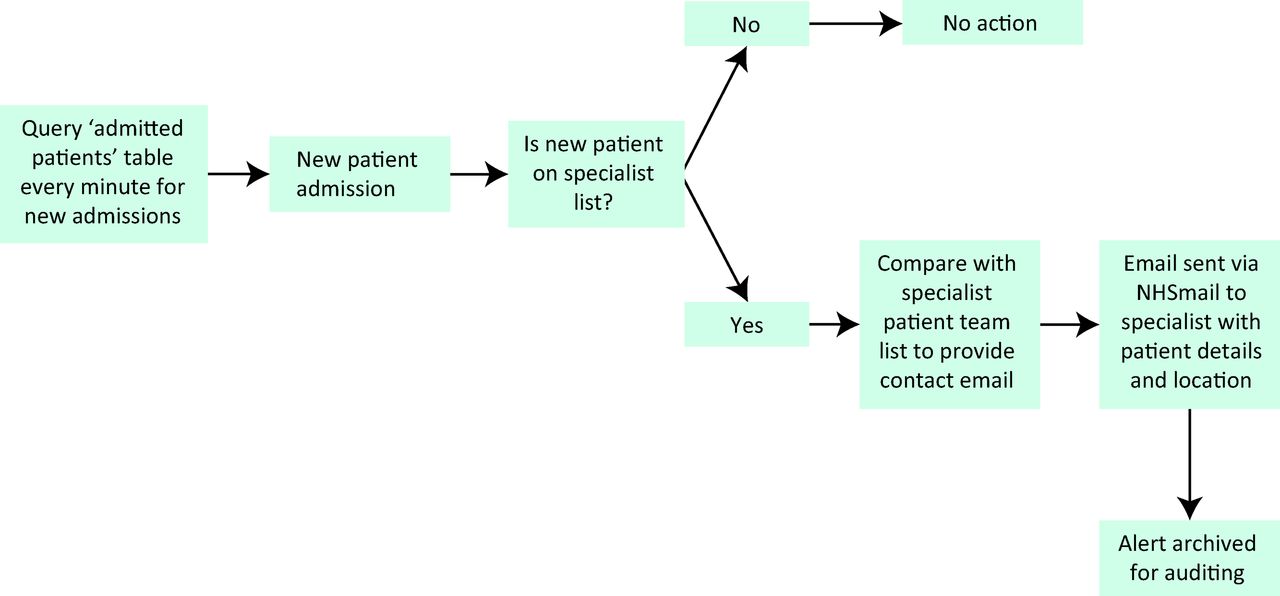
The data flow for the email alerting system. This incorporates the three key parts: identifying patient admissions, comparing these admissions with cohorts of patients from specialist groups and informing the appropriate specialist team.
The system uses only free software and requires minimal computing resources. (See Table 1 for details on where to source all the systems used.) It currently runs on a virtual machine with a single central processing unit (CPU) core, 1-GB RAM and 8-GB disk space. It is written using only around 1,000 lines of Java 7 (Oracle Corporation) code, combined with database vendor-specific Java database connectivity (JDBC) drivers running on the Community Enterprise Operating System (CentOS) CentOS 6.4, with an open source relational database management system, MySQL 5.6 (Oracle Corporation) as a local data store/cache and SimpleJavaMail (Google) for sending email messages. The total cost of implementation is approximately 40 hours of programming time plus £250.00 for the virtual machine. Maintenance costs vary according to the NHS organisation, but we estimate a maintenance commitment of approximately 1 hour monthly. Finally, user accounts will require maintenance although most NHS organisations have well-established, integrated, access management teams (IAMs). The system uses open source software and NHS infrastructure (eg NHSmail), allowing it to be easily transferred to other NHS organisations.
Systems and software used
Identifying patient admissions
All NHS hospital PASs have the ability to communicate with other computer systems by sending messages defined by a version of the Health Level 7 (HL7) protocol. In particular, a PAS could emit an admissions, discharges and transfers (ADT) stream that would inform an alerting system of new admissions (Fig 2).
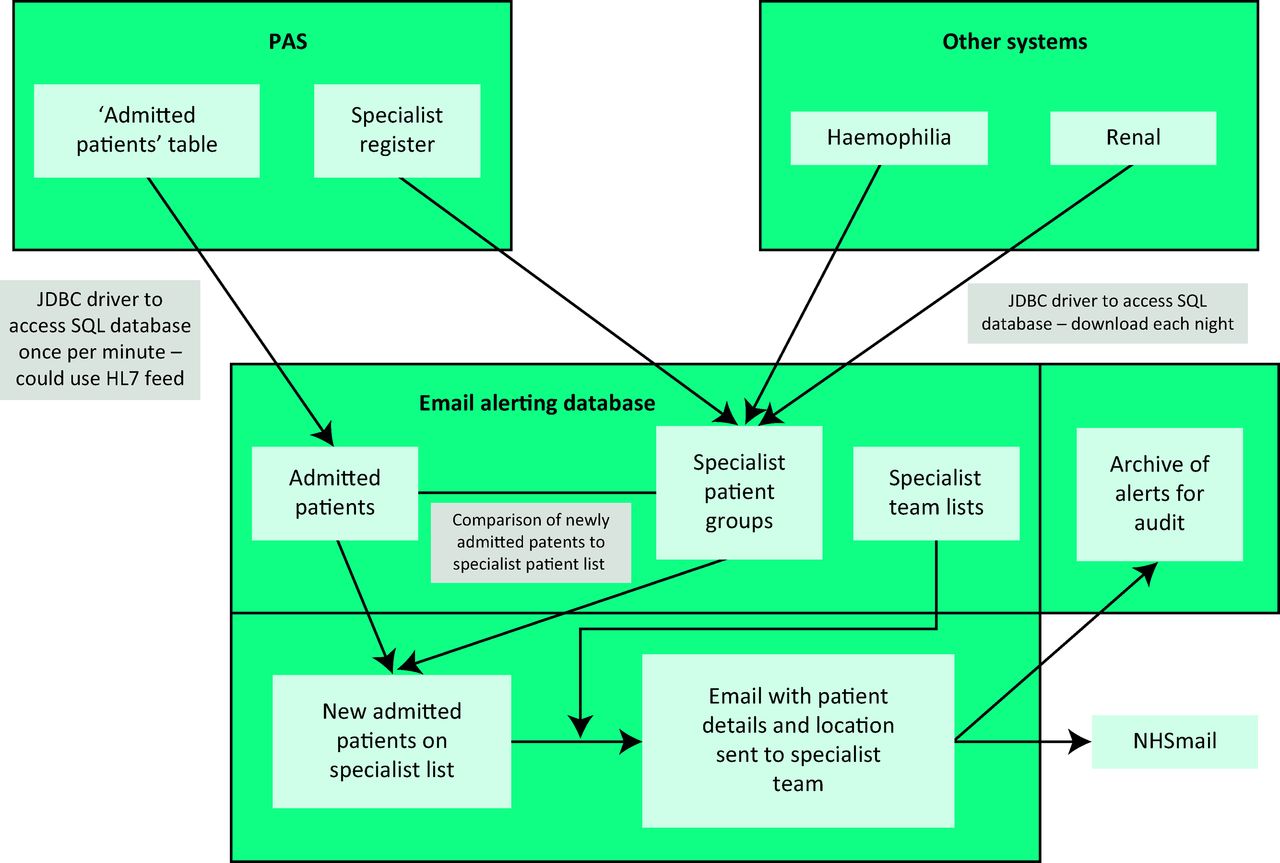
The email alerting system, demonstrating data sourcing and data flow between systems in order to generate an alert. HL7, Health Level 7; JDBC, Java database connectivity; PAS, patient administration system; SQL, structured query language.
To reduce the reliance on third-party software suppliers (and therefore development time and cost), the decision was made to poll the central database directly and identify new admissions from their recent appearance in the ‘admitted patients’ table, rather than consume an HL7 feed. The PAS at East Kent Hospitals University NHS Foundation Trust (EKHUFT) uses an InterSystems CachÈ (InterSystems Corporation) object store for which a JDBC (Oracle Corporation) driver is available to access the data through structured query language (SQL).
Identifying specialist patient groups
Some of the patient groups were available on special register lists within the PAS. These were imported into our system in the same way as the list of admitted patients (Fig 2). Other groups (eg patients with haemophilia, renal transplant recipients) are stored in separate clinical systems and these are downloaded each night via JDBC.
Informing the specialist team
NHSmail is a secure messaging platform that complies with NHS data security regulations (Connecting for Health9) and also enables staff to receive their emails, in near real-time, on mobile devices such as tablet computers and smartphones, through the use of Microsoft's Exchange ActiveSync system (Microsoft).
It was decided to use NHS.net as the output from our alerting system for the following reasons:
Inherent compliance with data security regulations.
Fast delivery of messages to a wide range of mobile devices.
Easy integration with our system via SMTP (simple mail transfer protocol).
Results
This system has also been implemented for the following admission patient groups: oncology, learning disability, neurology (multiple sclerosis [MS] and motor neuron disease [MND]), haemophilia, MRSA (methicillin-resistant Staphylococcus aureus) carriers and people known to be previously Clostridium difficile positive. Other areas where such alerting systems may be appropriate include patients at high risk of Creutzfeldt–Jakob disease (CJD), patients with endovascular aortic stents or aortic aneurysms, patients in clinical trials, etc.
The system currently sends alerts to 21 members of staff at EKHUFT. The patient population includes 6,047 patients on one of our 10 monitored lists or special registers. In the months of May and June 2013 the system alerted to 863 monitored patient admissions. These 863 alerts were sent as 2,158 separate messages (one alert can be sent to several defined recipients).
Both in its development and in its delivery, we have continually involved both the end-users and the patients. The methodological concepts were discussed with patient representatives, in particular with reference to data sharing. As the alerting system was initially developed for patients with kidney disease, implementation was discussed with these patient groups including the Kent Kidney Patients’ Association (KKPA) and a local renal charity.
Since implementation we have received continued positive feedback. Examples include:
This [the email alert system] is really useful. We were previously often unaware of a patient admission unless a relative contacted and informed us. This enables us to check on their condition and have them transferred if necessary.
The Inpatient alert system has proven really helpful for haemophilia patients as we follow up any flags to ensure the patients are receiving the correct treatment, if needed. Patients have been reassured that we are aware they have been admitted.
I find the service very valuable Ö I’m able to be a little more flexible and responsive.
We have an oncology alert for patients who are admitted into hospital who are known to have cancer and also those on chemotherapy and/or radiotherapy. We find the alert system fantastic as it enables us to provide a proactive service. We are able to start our day looking at the alerts, work out who is in, then go on to PAS to gain more information about the patient and review or telephone the ward. This allows us to review patients often before the consultant on-call ward round and so enables us to give information to the team to ensure the team can make informed decisions regarding the patient and their management.
Discussion and conclusions
Here we describe the development and implementation of a clinical system at East Kent Hospitals University NHS Foundation Trust for providing instant electronic alerting to specialist patient admissions, to improve patient quality and safety in the healthcare environment through early specialist intervention. Not only is this system efficient and effective, but importantly it can be implemented with low cost and complexity, and is hence easily reproducible across the National Health Service.
This paper describes the results of a pilot of the system; measurable benefits in terms of patient outcomes would, however, be challenging to prove in the context of multiple other patient safety interventions in recent years. However, the system has been avidly adopted by multiple clinical teams. Additional alerts are being developed as a result of requests from users across the trust.
This development is the first step in changing the approach to data flow in our organisation; previously clinicians were required to search for information in clinical and non-clinical IT systems. The future must be notification of events as they occur, and this has been adopted in many applications for mobile devices outside the medical sector.
A criticism of the solution presented is that emails may not be regularly checked by staff in our organisation. However, with the availability of NHSmail on smartphones and other mobile devices, and a wireless network across the trust, this risk is to an extent mitigated. We plan to develop the alerting system using push notifications to mobile devices in the future to further mitigate this risk.
There is a potential risk when sending alerts to multiple members of the same team; it raises the possibility of ‘alert fatigue’, but also the potential for individual members of the team not to take responsibility for taking action as a result of the alert. Alternative approaches to alerting mere general teams may be required where there is the ability to comment on alerts or to document actions taken as a result, for the rest of the team to review. Therefore this approach may be most appropriate for specialist clinical teams (eg oncology, renal transplantation and learning difficulties) where teams are small and responses can be discussed among the team.
It is possible that such systems may not be appropriate in large general teams for the reasons described above; further work is required to validate such a system in these settings.
It has to be acknowledged that all solutions such as the one described here require user acceptance. We present preliminary data supporting the use of such automated alerting systems. It has to be recognised that we may have encountered only ‘early adopters’ in this pilot work and acceptance across an entire NHS trust may require considerable change in management. To date the system has required virtually no training for recipients of the alerts and we are receiving regular requests to add additional alerts.
Finally, one key recommendation from the Francis Report was ‘accurate, useful and relevant information’.10 The system described here delivers an alert of a specific patient admission to the relevant healthcare professional at the right time, aiding early effective clinical intervention in complex patient groups. This is a key example of the use of information technology in healthcare to improve patient safety.
Learning points
> Alerting systems can be easily developed in NHS trusts using free software
> Alerting systems provide critical information rapidly to clinical teams
> Push notification of critical data is an efficient way of providing information to clinicians.
Authors’ contributions
All authors in this study were involved in conception and design, and critical revision of the manuscript for important intellectual content, and gave final approval of the manuscript for submission. CF, MB and MW designed the algorithm for patient alerting. TW developed the code for the alerting algorithm, SM and MF developed the testing regimen for the algorithm.
- © 2015 Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.