
ABSTRACT
Healthcare is at an important crossroads in that current models of care are increasingly seen by politicians and policymakers as unsustainable. Furthermore, there is a need to move away from the reactive, doctor-centred model of care to one that is more patient-centred and that consistently delivers accessible, high-quality and safe care to all. Greater use of health information technology (HIT) is seen by many key decision makers as crucial to this transformation process and, hence, substantial investments are made in this area. However, healthcare, particularly in UK hospitals, remains a laggard in HIT adoption. To uncover the underlying reasons, we discuss current implementation and adoption challenges and explore potential ways to address these. We outline strategic, organisational, technical and social factors that can ‘make or break’ technological implementations. Most importantly, we suggest that efforts should be characterised by an underlying awareness of the complexity of the hospital environment and the need to develop tools that support provision of integrated multidisciplinary care. We conclude with a discussion of promising future developments, including increased patient involvement; access and contribution to shared records; the penetration of smart devices; greater health information exchange and interoperability; and innovative real-time secondary uses of data. We argue that there is considerable merit in evaluating the introduction of these interventions to help ensure that they are optimised for effectiveness, support efficient working and minimise the possibility of inadvertently introducing new risks into already complex health systems. Our over-riding message is that HIT should be seen as, where appropriate, a potential enabler and an important source of data to support healthcare redesign and that critical, ongoing evaluation is key to maximising benefits. However, it should not be seen as a silver bullet.
Introduction
The number of preventable deaths in hospitals globally is alarming.1 In English hospitals alone, an estimated 12,000 patients die every year because of entirely avoidable errors, costing the National Health Service (NHS) up to £2.5 billion a year.2,3 Overall costs of care are also increasing, with a £30 billion shortfall predicted for the NHS England by 2020.4
Healthcare information technology (HIT) has been hailed as a way to reduce these figures by enhancing the quality and safety of care and, through so doing, improving outcomes.5–8 Significant national and local investments have been made on the basis of this assumption – it has, as a result, been predicted that the HIT industry will generate global revenues of US$185 billion by 2018.9
Previous work has identified that the key uses of the current generation of HIT offerings include: the storage, management, and transmission of data; decision support tools; and facilitating care from a distance (Box 1).10
Indeed, the underlying empirical evidence base is promising, albeit lacking transferability between settings and evidence surrounding economic returns.10 It is particularly difficult to demonstrate the impact of HIT implementation on clinical outcomes, because the effects of technologies are often hard to attribute.10
In the UK, general practitioners (GPs) have been successfully using HIT tools for decades,11 but the routine use of these in hospitals is lagging behind and many desired benefits remain elusive.12 This is particularly true for the larger, more complex HIT, such as electronic health records (EHRs) and electronic prescribing (ePrescribing) systems that are now increasingly implemented, because these transformative technologies are commonly expected to bring the biggest benefits.13,14 That said, the recently initiated English Technology Fund is stimulating implementation activity and hospital implementation efforts are picking up in England.15
However, why, well over a decade after the launch of major government-led HIT initiatives such as the English National Programme for IT, has HIT implementation and adoption in hospitals been so slow? In addition, despite substantial investment, why do these technologies often fail to live up to their potential?16,17
Factors contributing to slow HIT implementation progress in hospitals
Major benefits can be achieved through implementing HIT.10 This is particularly true for organisations that have extensively customised systems to suit their needs (ie ‘home-grown’ systems) and have overcome the difficult early implementation phase.13,14 However, the in-house conceptualising, building and maintaining of HIT systems is a complex, costly and time-consuming process and, therefore, most healthcare organisations are now choosing to buy commercial off-the-shelf (COTS) products. Nevertheless, these packaged products typically have a single underlying code base and, thus, offer little, if any, scope for local customisation, which can result in major challenges to the software integrating with, and supporting, clinical workflows. Other issues relate to limited experience with procurement, and the considerable start-up costs of systems.
Nonetheless, there are important lessons that the difficult journey of implementing hospitals towards electronic environments can demonstrate. These relate to strategic context, organisational approaches, technical characteristics and social consequences (Fig 1). They are discussed in more detail below, with particular reference to the UK. Potential strategies to address challenges are summarised in Box 2.
Box 2. Summary of potential strategies to address implementation challenges surrounding HIT in hospitals.


Factors contributing to slow implementation progress in -hospitals.
Strategic context
UK hospitals are large organisations that are part of an even larger system that is governed centrally – the NHS, which is further divided into NHS Wales, NHS England, NHS Scotland and NHS Northern Ireland. Although aims are similar, HIT implementation strategies and the associated involvement of governments vary. For example, England has now moved from an initially ‘top-down’ implementation model through a national programme characterised by central procurement of standardised technological systems, to a model that allows more local input in decision making among implementing hospitals.16,17 However, the consequences of the previously centralised procurement model are still widely experienced, particularly where organisations are continuing to implement solutions that they have not selected themselves. This can have disastrous consequences for not only the acceptability of systems among users (they are more likely to reject a system that they feel has been forced upon them), but also the strategies used by managers to initiate and sustain organisational transformations (they might not support the implementation and, therefore, behave in a way that conveys doubt to users).18
A particularly important factor that can to some extent facilitate adoption is the existence of financial incentives.19 For example, the USA has been successful in stimulating HIT use through the use of a centrally administered stimulus package.20
Organisational approach
For implementing organisations, strategy is just as important, but unfortunately not more straightforward. Radical organisational changes are often necessary as part of implementations,21 but these are complicated by the complexity of the hospital environment.22 Many teams work together often over great distances to deliver care – a carefully choreographed act. When new ‘off-the-shelf’ technology is introduced, the dynamics change and hospital staff have to learn new ways of working.23 This is not always easy for individuals and extremely difficult to manage. For example, there is a risk that organisational processes are simply automated, as opposed to redesigned, which then results in a lack of the desired benefits.17,24 In addition, there is commonly little appreciation that benefits might take a long time to materialise (because they are, to a large extent, dependent on efficient health information exchange (HIE)) and that desired safety and efficiency savings are hard to attribute.17,25,26 As a result, financial risks are a real threat, particularly within the first few years of adoption. Therefore, it is important not to overestimate early benefits and to appreciate that these are likely to have diffuse effects that are difficult to measure.17,25,26
Technical characteristics
It has also frequently been found that technical characteristics can influence the implementation of HIT.16,17 Key challenges include poor usability, functionality and performance (which can introduce new threats to patient safety).27–29 Issues here can range from long system response times to long-winded data entry, which can mean that information cannot be accessed when needed and/or recorded by users.16,17 In addition, system design can mean that certain errors are more likely. For example, selection errors can occur when users unintentionally click on the wrong medication because it is in close proximity to the intended drug on the list.16,17 Such technical issues often emerge not only because system development lacks end-user input, but also because of the difficulty in customising systems to suit the needs of different professional groupings operating within hospitals.16,17
Other repeatedly found technical characteristics that can hinder implementation progress include the lack of HIE and interoperability within and across organisations, as well as the marginalisation of patients and carers.26,30
Social consequences
As already alluded to above, system implementation can have various unintended and undesired consequences. Some of these are social in nature, with various potentially adverse effects on clinical workflows and collaborative working.16,17,23,31 For instance, it has been found that, in some cases, systems can reduce face-to-face contact within teams and between healthcare professionals and patients, and shift the focus of healthcare professional work to increased data entry activities.16,17 This in turn can lead to resistance to use HIT or the development of ‘workarounds’, where the technology is used in ways other than intended.32
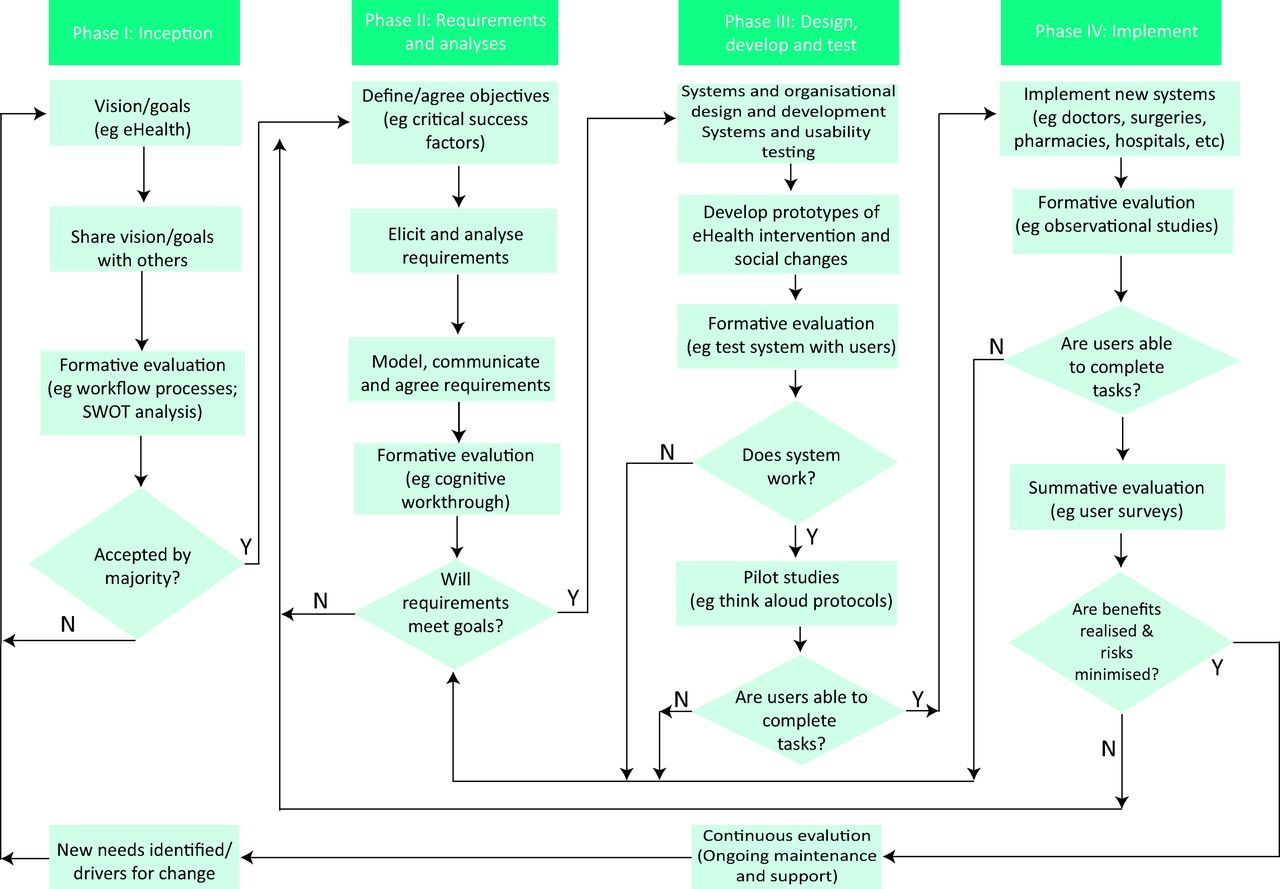
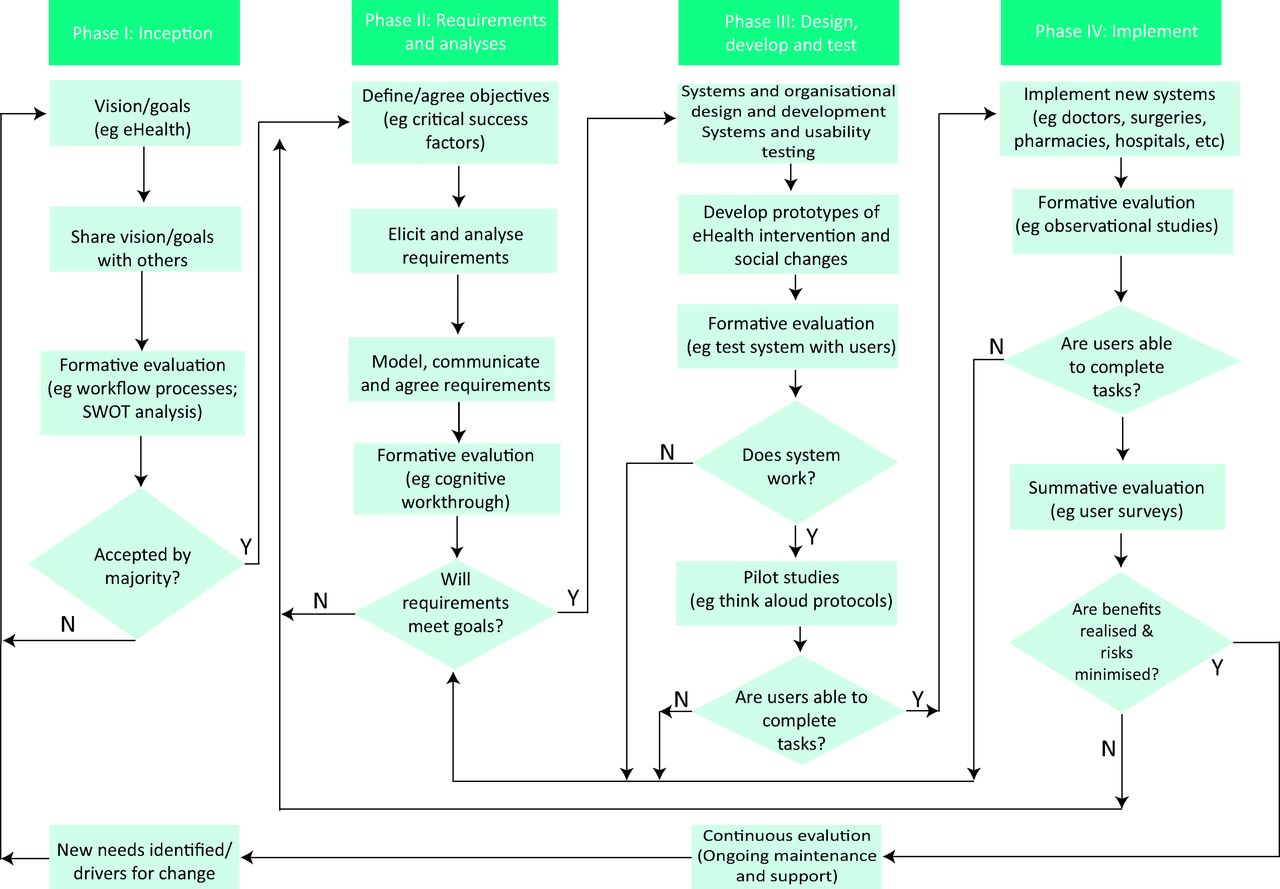
To ensure that system design reflects different needs, it is important that efforts are made to understand and take account of the broad range of stakeholders who are using HITs.33 Admittedly, the range of users in hospitals is large, but some successes have been recorded through strategies including: close working relations with developers, clinical champions and leadership, and continuous engagement and evaluation activities.25,26,34 Meaningful and ongoing evaluation is particularly important to promote more clinically relevant technologies and ensure continued engagement of users (Fig 2).35,36
Opportunities and challenges ahead
As it stands, HIT applications in UK hospitals are still inadequately conceptualised tools that do not meet the complex needs of patients, professionals and organisations. This is in part the result of the multifaceted environment and the multitude of factors that need to be considered during implementation and beyond (discussed above). Notwithstanding the significant amount of work required, a vision of the future aims of technological change is important. Below, we discuss some potential future scenarios and international innovators that have made significant headway towards achieving these.
Interfacing and HIE on a larger scale
Many of the benefits of HIT are dependent on sharing of information – be it across devices and equipment or across healthcare organisations.37,38 Therefore, one important development that is likely to see increasing attention is HIE, the electronic exchange of information relating to health. The Holy Grail of HIE is the so-called ‘HIMSS Level 7’, a state of seamless electronic information exchange that enables using data to improve processes of care, quality, and safety (see the discussion surrounding secondary uses below).39 This includes a fully functional electronic health record used to exchange information across the local health community, with access for health professionals and patients. Stages of adoption are tracked by HIMSS Analytics, a USA-based not-for-profit organisation that helps organisations to work through eight stages towards an electronic care environment. Currently, 190 US hospitals, three European hospitals, three Asian hospitals and one Canadian hospital have achieved HIMSS Level 7.
On a small scale, the more consistent use of standards will pave the way for HIE with ‘smart’ devices that are able to respond to electronic signals. This includes, for example, wearable technology, such as wristbands that contain wireless communication devices and can exchange information with hospital computers. Benefits here include not only instant access to patient-specific information for healthcare professionals, but also (depending on the ability of the device) potentially monitoring of vital signs.40
Similarly, there is likely to be greater use of robots in hospitals that are part of a larger HIE system, such as those that dispense medications to reduce dispensing errors, or those that clean hospitals to reduce healthcare-associated infections.41,42
Looking ahead, the drive towards integrated health and social care and the availability of cloud-based data management means that we are likely to see greater developments surrounding sharing of data with community providers and, indeed, directly with patients themselves. As a result of these developments, data management, security, storage, analysis and interpretation are likely to be core future missions for hospitals.43
The beginnings of seamless integration can already be seen in some local health communities. For example, the Indiana Health Information Exchange is the oldest health information exchange network in the USA. It uses electronic data interchange for healthcare transactions between hospitals, community care facilities and other healthcare organisations. Run by the Regenstrief Institute, it now holds data on more than 7 million patients.44 Similarly, the Andalucian health system has been using a Cerner integrated regional EHR and electronic prescribing system spanning public health, primary, secondary, emergency and social care since the 1990s.45,46
However, although already bringing significant local benefits because data are seamlessly shared between electronic devices, humans and locations; current tools that have emerged with a discrete focus, often on particular functions within hospitals, have limited capacity for HIE and interoperability, and are not designed to support transitions between home-, community- and hospital-based care. Existing HIE initiatives also tend to use an integrated system by one designated supplier. Potential issues might emerge when organisations using different systems are required to interface, and there is a risk of commercial monopolies.
Patient-centric architectures – patients as the new users
Although myriad HIT users are currently problematic, this is likely to become more complicated in the future, because patients are likely to have increased control over their records. Although patients’ ability to edit health information will facilitate involvement in care, the implications for working practices of healthcare professionals could be significant. At best, increased patient involvement will result in more targeted and efficient care with patients as active participants, whereas at worst, patients might be viewed as interfering, resulting in adverse effects on relations with healthcare professionals.
Nevertheless, some successful examples exist, although these do not allow patients to enter information electronically, but focus on facilitating communication between healthcare professionals and patients at a distance, and patient access to their records. For example, The National Shared Care Plan in New Zealand is a programme sponsored by the National Health IT Board and the Auckland Regional District Health Boards. It allows communication between patients with long-term conditions and between different healthcare providers through a coordinated electronic care plan.47
Similarly, OpenNotes allows patients to access and read their medical notes electronically. It is a national initiative in the USA aiming to promote patient access and active involvement in care activities and, in due course, the co-authoring of records.48
The Blue Button initiative allows patients online access to their own health information, including medications, allergies and lab results. It is widely used in the USA in the Veterans Health Administration and the Center for Medicare and Medicaid Services (the main US national social insurance program), among others. The scheme is expanding rapidly with numerous public and private sector organisations implementing the Blue Button and expanding Blue Button capabilities nationwide.49
Innovative secondary uses of data
Another promising development relates to the increasing secondary uses of data held within electronic systems. Currently, some of the benefits are derived from analysing data within organisations,16,17 but the future is likely to be characterised by aggregating data in a way that transcends organisational boundaries. Potential benefits exponentially increase with scale, although so do organisational challenges, because of the increasing number of health- and social care organisations involved. Moreover, key challenges are likely to include continuing debates surrounding patient confidentiality and consent, and the capacity to meaningfully analyse data that become available.
Again, some international examples of routine secondary uses on larger scales that transcend organisational boundaries exist. These already bring significant organisational benefits. For instance, Kaiser Permanente provides care for 8.6 million members in California and parts of Colorado. In 2002, the organisation began working with Epic Systems Corporation to create and implement an integrated EHR (KP HealthConnect). Although centrally governed, the system is configured in line with the needs of different localities. An in-house analytics team routinely draws on data to improve the quality and efficiency of care provided. This includes data warehousing, and both operational analytics (clinical and financial) and research analytics (to support research into for example health disparities and comparative effectiveness research).50
Geisinger Health System provides for over 2.6 million people in Pennsylvania. It began implementation of EpicCare, an integrated EHR, in 1996. Having collaborated with IBM to create an integrated data warehouse, the system now supports a range of research projects drawing on EHR data. As part of this, the organisation is able to simulate re-engineering of care processes, and allows for testing of new software tools in clinical environments and then commercialisation of these (xG Health Solutions).51
Conclusions
Medicine and in particular hospitals in the UK have lagged behind in relation to HIT implementation and adoption. A significant contributing factor has hitherto been short-term thinking relating to strategic environments, technologies and organisational strategies, often resulting in various unintended social consequences. Therefore, there is a need for a longer-term perspective that sees HIT not as an end in itself but as a continuous journey towards a future data-rich environment that supports the provision of safe, high-quality and efficient care, and the creation of learning health systems.
HIMSS Level 7 and the notion of continuously Learning Health Systems (LHS) that use electronic data for quality and safety improvements are currently the closest way to envisage this future.39,52 However, it is also important to recognise that new technical solutions will become available, working practices will continue to change and guidelines will be updated. Therefore, implementation of HIT is always a work in progress with constantly new emerging challenges. To deal with these challenges, hospitals will have to transform the way they function as HIT takes on new roles that have to be accommodated by healthcare workers.
The increasing use of HIT is inevitable and the range of HIT tools is likely to proliferate over the coming years as we move to ubiquitous computing environments. The approaches outlined above can maximise benefits and minimise risks throughout this journey. Developing HIT and creating data-rich environments is increasingly central to the provision of high-quality care, but is in itself insufficient because technological characteristics need to be contextualised within their social, organisational and political environments (Fig 1). Promising future opportunities include the co-creation of HIT to better support the delivery of integrated patient-centred care, design of data-rich environments, and more seamless models of care and exchange of information with other professionals and in particular patients and/or carers through the increasing array of consumer informatics tools.
Acknowledgements
We are very grateful to all participants who kindly gave their time and to the extended project team of the work we have drawn on. We are also very grateful to Dr Brian Robson's helpful comments on an earlier version of the paper.
This work has drawn on research funded by the NHS Connecting for Health Evaluation Programme (NHS CFHEP 001, NHS CFHEP 005, NHS CFHEP 009, NHS CFHEP 010), and the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-1209-10099). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
- © 2015 Royal College of Physicians
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Five key recommendations for the implementation of hospital electronic prescribing and medicines administration systems in Scotland
- Perceptions and experiences of the implementation, management, use and optimisation of electronic prescribing systems in hospital settings: protocol for a systematic review of qualitative studies
- Understanding and evaluating the effects of implementing an electronic paediatric prescribing system on care provision and hospital work in paediatric hospital ward settings: a qualitatively driven mixed-method study protocol