
ABSTRACT
A Health and Social Care Alliance established in 2012 and selected as a national ‘Integration Pioneer’ site is exploring how integration can address local system challenges faced in many health economies across the UK. The original programme focused on data gathered from the evaluation of the national Integration Care Organisation pilots – there were three in West Norfolk – about patient experience, aiming to develop stronger early community interventions in a more coordinated way to keep people independent longer. The early programme initiatives have created a firm partnership, innovative services and a good foundation on which to build, which has been a strength as the local health economy now faces a huge financial and clinical sustainability challenge in its current configuration. A transformation programme is therefore being developed to address the challenges and identify solutions through integration and innovation for the sustainability of a small rural locality.
Background
West Norfolk is a distinct local health economy (LHE) with a single clinical commissioning group (CCG) coterminous with Kings Lynn Borough Council. At its centre is the Queen Elizabeth Hospital NHS Foundation Trust King's Lynn (QEHKL), which serves the West Norfolk CCG area and some populations from neighbouring Cambridgeshire, Lincolnshire and Central Norfolk. The wider provider landscape includes a large mental health trust, a county-wide community trust and a vibrant voluntary sector. There is a strong history of local public sector partnership working, which also includes education and housing. West Norfolk has a widely scattered and increasingly ageing population of 165,000 people with pockets of social deprivation. There are limited resources to serve them, spread across multiple suppliers in the NHS, social care, local authorities and the voluntary sector. Residents have a variable understanding of a fragmented system and the health and care economy depends, to a greater extent than in many urban areas, on the goodwill of volunteers. However, the biggest problem is the lack of integration and information sharing.
West Norfolk benefited from its engagement as part of the National ‘Integrated Care Organisation’ (ICO) pilot in 2009–2011, during which local older people were canvassed. Respondents indicated that they only wanted to tell their story once, saw their GP practice as their single point of contact, expected care agencies to share information and be co-ordinated and weren't concerned which organisation provided what. These sentiments align closely with the National Voices statements.1
The ICO model was very successful in West Norfolk as it built on the well established foundation of partnership across public and voluntary services. As a result, there was commitment to innovate further and create joint initiatives to serve the population. Thus, the county council and CCG first established an integrated commissioning team for community health and care services from the inception of the CCG, providing the practical mechanism for commissioning integration. Community health and social care teams now operate from three integrated locality hubs, hold multi-disciplinary team meetings and have an integrated health and social management structure. Second, a ‘prevention first’ partnership has been established between the borough council, voluntary organisations, the CCG and county council, bringing together elements commissioned through the partners to create connected targeted prevention for older people. Third, the Borough Council has led the implementation of the first stage of this, creating a web-based database and helpline providing connection to a wide range of services to support older people maintaining their independence.2 Fourth, voluntary and community groups are supporting the establishment of a network of community-based support services to promote the connectivity of isolated people to these services. The introduction of a structured time banking scheme has already resulted in 750 new volunteers coming forward in the area. Finally, system-wide health Commissioning for Quality and Innovation (CQUIN) initiatives that targeted the avoidance of emergency admissions to hospital, where some providers contributed more than others to ensure the best overall outcomes, were implemented.
In order to ensure a coordinated approach to further innovation, the West Norfolk Alliance was established in 2012. This group of chief executives, led by the CCG, committed via a formal memorandum of understanding to tackle the obstacles to implementing more ambitious integration. Its focus derived from a very clear mandate to improve each individual resident's experience of care, learning from all that they had said about their difficulties. The ambition was to move from the scenario of describing the problem to a scenario of seamless integrated care, with the user in control. This informed the development of the strategic plan for integration, which explains the aim of integration and sets out four fundamental principles upon which the entire programme of work is based. These principles are illustrated in Fig 1.

The Alliance integration pyramid.
The 2013 National Integration Pioneer bid was therefore built on very clear ‘person-centred’ principles, which have guided every service innovation and care intervention. However, delivering this will require new ‘permissions’ that transcend organisational boundaries and challenge current financial incentives and regulations. The pioneer scheme affords the opportunity to influence policy at a national level and is essential in order to have a really positive impact on patient experience, advising relevant national bodies on how other similar LHEs can benefit. Transformation on this scale will require significant cultural change and, for this reason, leadership development and front-line staff development programmes have been developed. These challenge assumptions that hinder integration and empower frontline staff to behave differently when delivering care, and have the full support of all Alliance member organisations. The expectation is that staff will learn to consider themselves as working for the Alliance rather than one of its constituent parts.
The over-arching objectives for local integration are to align resources to the needs of population, not to institutional boundaries. Contact with any service will generate an integrated ‘Alliance’ response, deliver timely care, with a focus on maintaining health and wellbeing (and preventing ill health) while achieving long-term financial and operational ‘sustainability’ for health and care services in West Norfolk. A fundamental aim is to serve as a national forerunner to innovate, challenge and deliver sustainable health and care solutions for local populations.
Current context in West Norfolk
In West Norfolk, a number of factors are now converging, which serve to make up an urgent case for change. These include the increasing gap between demand and resources, as well the pressure facing smaller district general hospitals in terms of the general viability of this traditional model. This is well documented elsewhere and was acknowledged as a major challenge in Monitor's report published earlier this year.3 The challenges faced by the West Norfolk healthcare system are illustrated in Fig 2.
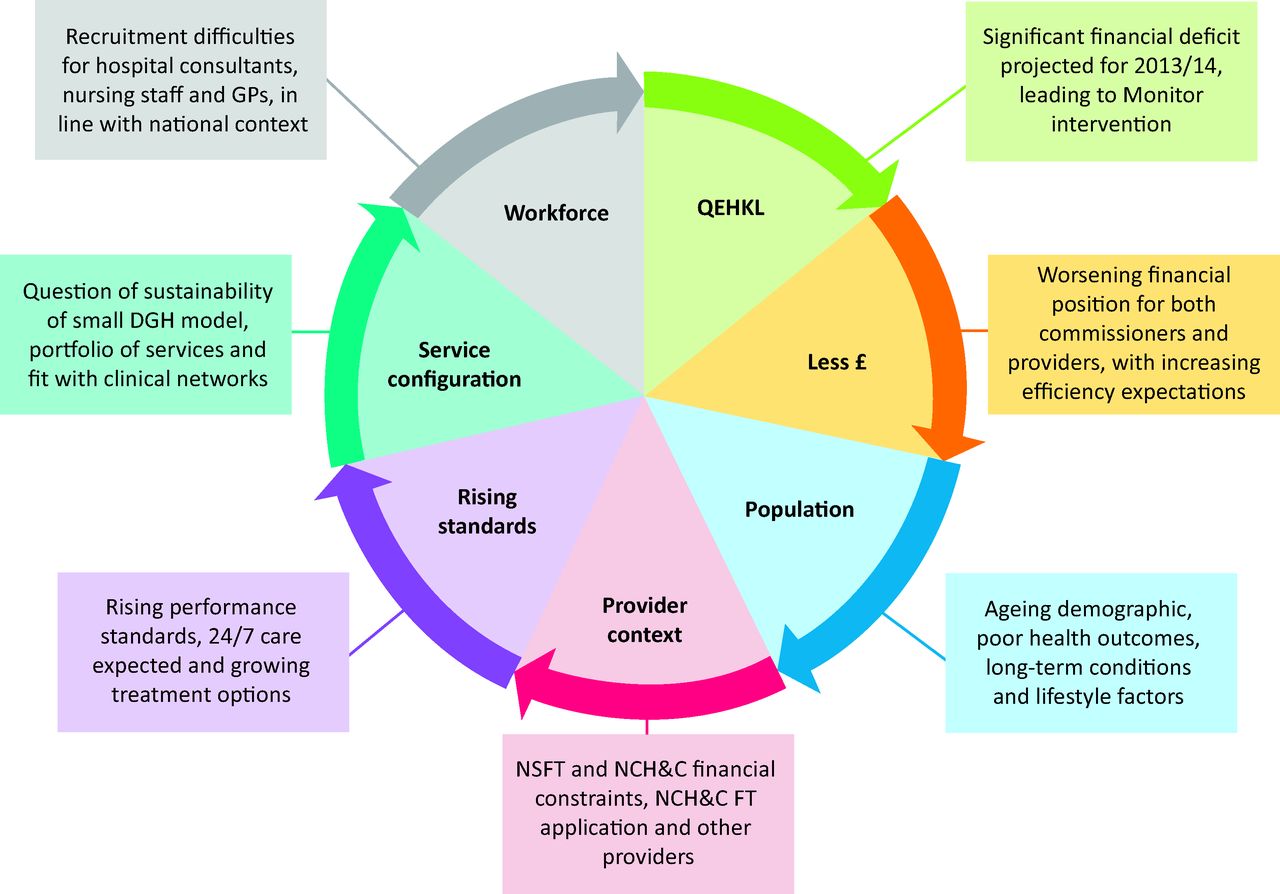
Challenges faced by the West Norfolk healthcare system. DGH = district general hospital; NCH&C = Norfolk Community Health and Care NHS Trust; NSFT = Norfolk and Suffolk NHS Foundation Trust; QEHKL = Queen Elizabeth Hospital NHS Foundation Trust King's Lynn.
The financial challenges
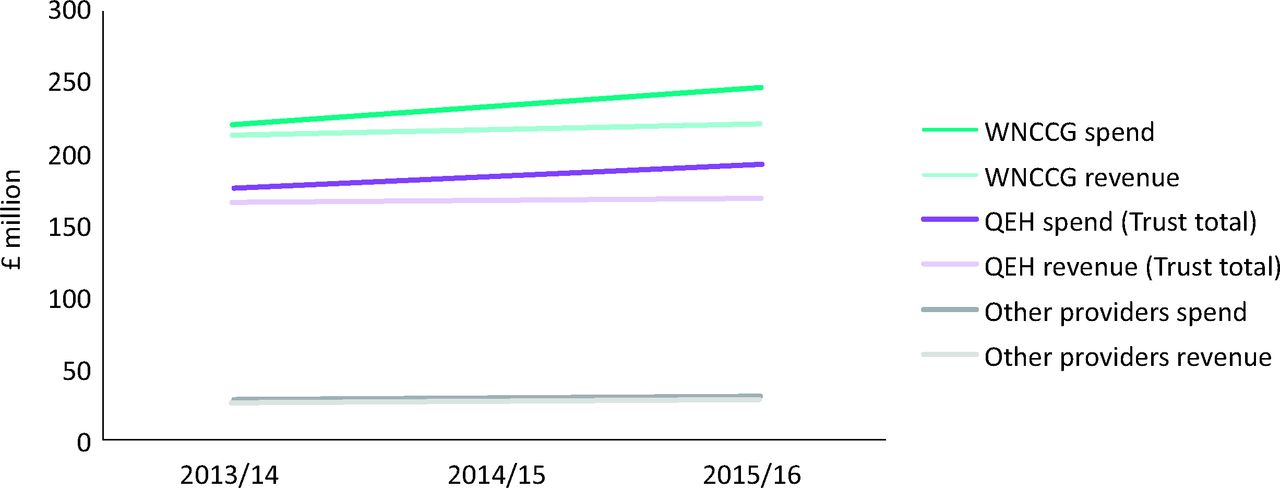
The national financial picture is one of a further £30 billion of savings by 2020, as identified in the NHS's ‘Call to action’4 and reinforced by its Five year forward view published in October.5 In line with the national financial picture, there is a growing gap locally between the available healthcare commissioning budget and anticipated financial costs (Fig 3). This is further compounded in West Norfolk by an ageing demographic, with higher than average incidence of long-term conditions and lifestyle behaviours with negative effects on health and wellbeing, so a proxy for the additional financial pressure caused by this profile was incorporated into the financial forecast, based on data supplied by the Kings Fund.6
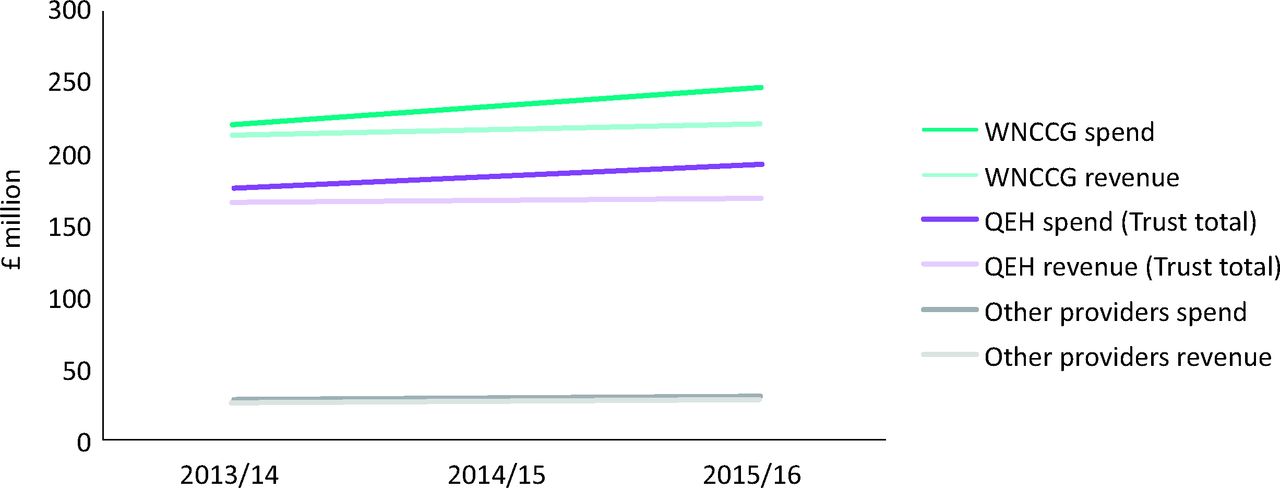
Financial challenges faced by the West Norfolk healthcare system. QEH = Queen Elizabeth Hospital; WNCCG = West Norfolk clinical commissioning group.
Continued pressure on commissioning budgets and the need for providers to achieve delivery of 4% cost savings with minimal impact on quality and service delivery creates a real and immediate problem. This is in the context of many providers being constrained by their infrastructure factors, such as ageing estate and technology challenges. Further, the requirement to increase NHS funding flow to social care will present further issues for consideration of future funding shares across health and social care. The CCG therefore decided in summer 2013 to commission an analysis of the financial and clinical sustainability of the LHE, including the three main providers and the CCG. The findings of this analysis were clear; continuing to commission services in the same way would become unsustainable.
Configuration challenges
Acute hospital services have been under review both nationally and regionally over recent years. District general hospital services have been called into question in terms of their clinical, operational and financial sustainability nationally.7 Legitimate questions have been posed regarding the clinical viability of DGHs to provide particular services based on catchment population and national royal college guidance, their ability to deliver services within estate constraints and whether they can operate effectively in a marketplace where choice and contestability is greater. Following detailed analysis of its financial sustainability, the QEHKL identified a significant shortfall in funding and finished 2013/2014 with a deficit of £13 million, with this position set to further worsen over forthcoming years. This led to the regulator Monitor placing the Trust into ‘special measures’ in November 2013. The need to develop a commissioning statement regarding local designation of essential services was clear and included particular consideration of the tension between clinical ‘best practice’ guidance and the rural geography, proximity of other acute providers, transport limitations and inequalities.
Workforce challenges
A fundamental contributor to the viability question facing small acute hospitals is the issue of recruiting and retaining high calibre staff. The Centre for Workforce Intelligence has estimated that if consultant numbers continue to expand according to the number of doctors in higher training, then the total number of consultants in hospital in 2020 would increase by 60%, increasing the pay bill by £2.2 billion.8 This challenge is compounded by the ageing population, the increasing clinical complexity of patients and the continuing impact of the reduction in trainee doctors’ hours enforced by the European Working Time Directive.
This picture, common nationally, is heightened in West Norfolk due to the difficulty in recruiting medical, nursing and wider therapy staff alike, with provider organisations being unable to fill vacancies and having to resort to initiatives such as recruitment from overseas.
Clinical challenges
Further to the difficulties in recruiting and securing a workforce that can cope with the increasing patient demand, additional challenge is posed by the need to ensure clinical expertise and sustainability of provision in line with the specialities and treatments offered by any one provider. For example, interdependencies between services will require certain clinical expertise to deliver effectively, which can be harnessed via direct recruitment, or via networks and collaborative provision. For the QEHKL, specific challenges will be posed in delivering sustainable high-quality hospital services due to the effects of geography, size and specialty skill mix on recruitment and retention of a high calibre clinical workforce in some specialist areas. Collaboration and consideration across providers will be necessary to consider how, through innovation and creativity, job roles can be created which prove more attractive to aid recruitment and retention. For all these reasons, the relationship between clinical and financial sustainability in smaller DGHs is strong.
Maintaining high quality care in the environment described above presents enormous difficulties but also opportunities. The acute trust has been implementing a quality improvement programme following CQC intervention in October 2013 and this added a further imperative to the case for change. Workforce recruitment played a major part in the quality concerns, and the simultaneous pressure facing acute trusts to achieve NHS Constitution standards, such as A&E waiting times and ‘referral to treatment’ times, with less staff available, created an unprecedented combination of factors that could adversely affect the quality of patient experience.
System Sustainability Programme
As a consequence of these converging challenges, the West Norfolk Alliance commenced an ambitious System Sustainability Programme in January 2014 to ensure continuity of care for West Norfolk residents. The main aim of the programme is the same as the integration ambition to ensure ‘sustainable, co-ordinated services with patients in control’. A series of working groups were established to take the programme forward, focusing on the patient experience, clinician views on quality and future sustainability. The working groups are shown in Box 1. Each started with an analysis of the local demography, inequalities, health needs assessment and workforce age and skill-mix profile. The groups then used a consistent method to examine key elements of provision throughout pathways of care. This involved mapping how services look today, how this compares with evidence about ‘best practice’, and how they could be redesigned in the future to improve access, quality and efficiency, using the concepts of ‘envelopes of care’ (the primary, secondary and tertiary settings and returning home) and ‘ceilings of care’ (triggers which determine when a patient moves from one ‘envelope’ to another).
Box 1. Working groups of the System Sustainability Programme, West Norfolk Alliance.

In this way, a consensus about services was built that highlighted particular areas for improvement and identified common clinical themes that were critical across the whole range of provision. Each working group produced an interim report with recommendations to be explored and implemented through the enabling workstreams (infrastructure, workforce, finance and contracting). Using this approach, each working group developed a set of recommendations and key themes, which could then be tested horizontally across a number of wider clinical specialties, to provide a whole-system picture and highlight actions for change, such as workforce development, new contractual mechanisms and the reconfiguration of services to improve financial and clinical sustainability.
Early findings
The results of the System Sustainability Programme are encouraging and lead to optimism that the methodology is a well-designed approach. There is an inevitable pressure in such situations to produce quick-fix solutions and meet the timetable of regulatory bodies for problems in particular parts of the system. However, what we have seen elsewhere in the country is that the process of transformation, particularly in relation to determining ‘commissioner requested services’ and finding long-term sustainability solutions for a distressed DGH, has to be conducted with rigour using an inclusive process involving patients, front-line clinicians, the public and MPs, to ensure transparency and clarity about both the scope of the problems and the potential solutions for debate and decision. The early findings are producing a series of hypotheses about the future configuration of services, which are being tested to see if they stand up to scrutiny.
In July 2014, Monitor appointed a Contingency Planning Team which commenced a programme in October to develop sustainable options for the future of the DGH.9 This programme is being overseen by Monitor and NHS England via the Local Area Team and the CCG, with the recognition that successful options must address the whole health economy and not simply the acute trust. The CPT programme therefore sits within the overall West Norfolk System Sustainability Programme, using the already constituted Clinical Reference Group and building on the findings. This has the advantage of creating a powerful data analysis and model-building resource through the CPT at exactly the right point in time, with local stakeholder engagement and clinical dialogue already well underway.
Conclusion
The challenges faced currently by commissioners and providers of health and social care are daunting. However, the focus and drive they generate can be harnessed to make great strides in improving the quality and efficiency of services. The problems facing the West Norfolk local health economy are not unique; many other areas in the UK with small DGHs face similar challenges with no obvious solutions. However, West Norfolk is ideally placed to develop a methodology to tackle these challenges, which may help to increase understanding and generate solutions for other health economies in a similar situation. What is clear is that a critical component in the development of solutions is local ownership, very early engagement of stakeholders about the nature of the problem, cross-organisational clinical dialogue about the local exigencies and a partnership approach to seeking sustainable long-term solutions for the ‘Neighbourhood Health Service’.5
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.