
ABSTRACT
There is an increasing realisation that new care models will be required to deliver healthcare to an increasingly elderly and complex patient population. District general hospitals (DGH), particularly those in rural locations, have a key part to play in providing care to their local population, but there is a growing realisation that the DGH model will need to evolve considerably to be financially and clinically sustainable in the future. NHS England's Five year forward view has established a number of options for new models of care, and health communities around the country have been selected as vanguard sites to pilot these new care models. Yeovil District Hospital has been working for two years in primary care, social care and community services in the Symphony Project to develop an integrated care model which will proactively manage the care of the most complex patients. The model has been selected as a vanguard site and the hospital is developing a new model which has the potential to be adopted by other smaller local district hospitals.
Policy context
When I became the chief executive of Yeovil District Hospital in 2012, the demise of small hospitals was seen as inevitable. The drive to centralise services in larger, specialist units that had a greater number of consultants and equipment, and the associated economies of scale and efficiency, were perceived to seal the fate of small hospitals. Many believed that local district general hospitals (DGHs) would need to downsize radically or close as they were rendered clinically and economically unviable.
In the past twelve months, there has been a significant about-turn in the direction of travel and recognition is growing that DGHs have an important role in providing services to their communities, particularly in more rural areas where an increasingly elderly population with complex comorbidities requires good local services.
The publication of the Five year forward view1 in autumn 2014 was significant for smaller hospitals with its focus on developing new care models that responded to local need and context. In particular, the primary and acute care system model (PACS) promoted in the Five year forward view provides a real opportunity to bring together clinicians from primary and secondary care to integrate services across organisations for the benefit of patients. Having been selected by NHS England as one of the vanguard sites to test out these new care models, the health and social care community in south Somerset has been given an opportunity to radically redesign how care is delivered across our system and to the benefit of the people it serves, and to ensure financial and clinical sustainability of both primary and secondary care in the locality.
Yeovil District Hospital NHS Foundation Trust
Yeovil District Hospital NHS Foundation Trust (YDH) has a strong track record of clinical and financial performance over a number of years. As an early foundation trust (2006, it was one of the first nationally to deliver the 18-week waiting time standard in 2007; and it has delivered a balanced financial position for many years. The hospital delivers a standard range of DGH services from 345 beds and a small (1,600 births per annum) consultant-led maternity unit. There were 45,538 emergency department (ED) attendances in 2014, which represents a cumulative increase of 6.8% over the previous 5 years. YDH actively collaborates with neighbouring trusts, including Dorchester and Taunton, in providing services such as percutaneous coronary intervention, vascular services, ear nose and throat and oncology; specialist services are delivered by centres in Bristol and Southampton.
The majority of services at YDH are commissioned by Somerset Clinical Commissioning Group (CCG) with a small percentage (15%) being commissioned by Dorset CCG. Both Somerset and Dorset are popular retirement destinations and 21.6% of the local population are over the age of 65, compared with the national figure of 16.3%. The demographic of the patients cared for by YDH is therefore comprised predominately of older people, and the proportion of older patients is projected to increase significantly over the next 20 years (ONS 2008 – based population projections for south Somerset).
The Symphony Project
Against this backdrop of increasing demand from an older population, and the financial pressures facing acute hospitals, the trust began a programme of work in 2012 to explore how to deliver a model of care that would accommodate the increasing demand locally while delivering financial sustainability. The Symphony Project brought together the acute hospital, primary care, the CCG, community services and social care with the aim of delivering an integrated care model combined with a new commissioning and contracting process that would address some of the existing perverse financial incentives incorporated into the existing system.
First, the Project sought to understand the pattern of patient utilisation of the existing resources and the costs being incurred by partner organisations. This involved the sharing of anonymised data from patients receiving primary, secondary and community care, as well as from those using mental health and social care services. This data set was drawn together by the South West Commissioning Support Unit and an analysis undertaken by the Centre for Health Economics at York University.2
Use of the Symphony data enabled partner organisations to obtain, for the first time, a complete picture of the way in which services are utilised and the associated costs incurred across the system for each patient. This was an important tool not just for the project team and the organisations involved but also for engaging clinicians in a data-driven discussion about the way in which services were currently configured, provided and used.
The data-analysis exercise demonstrated that although age was a determinant of service utilisation, the more significant driver was comorbidity, with the costs of care increasing significantly as the number of chronic conditions increased (Fig 1).
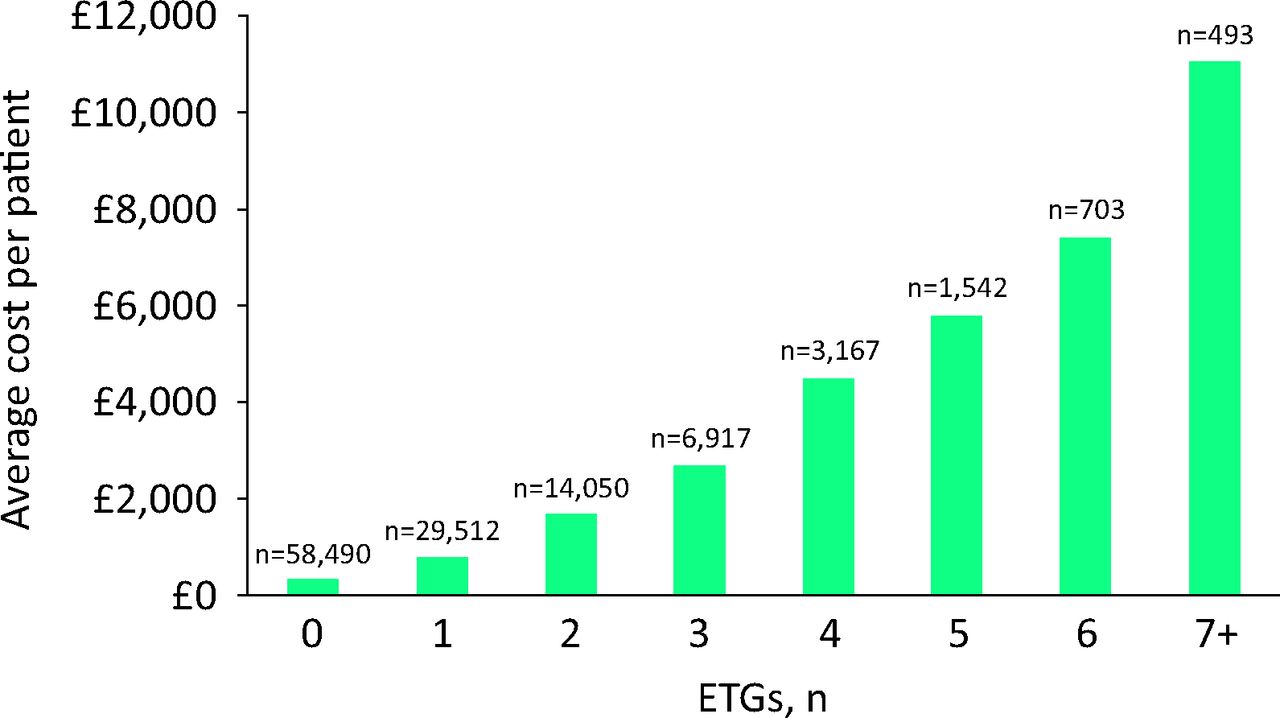
South Somerset average cost per patient versus number of clinical conditions per patient (expressed as number of ETGs). ETGs =episode treatment groups.
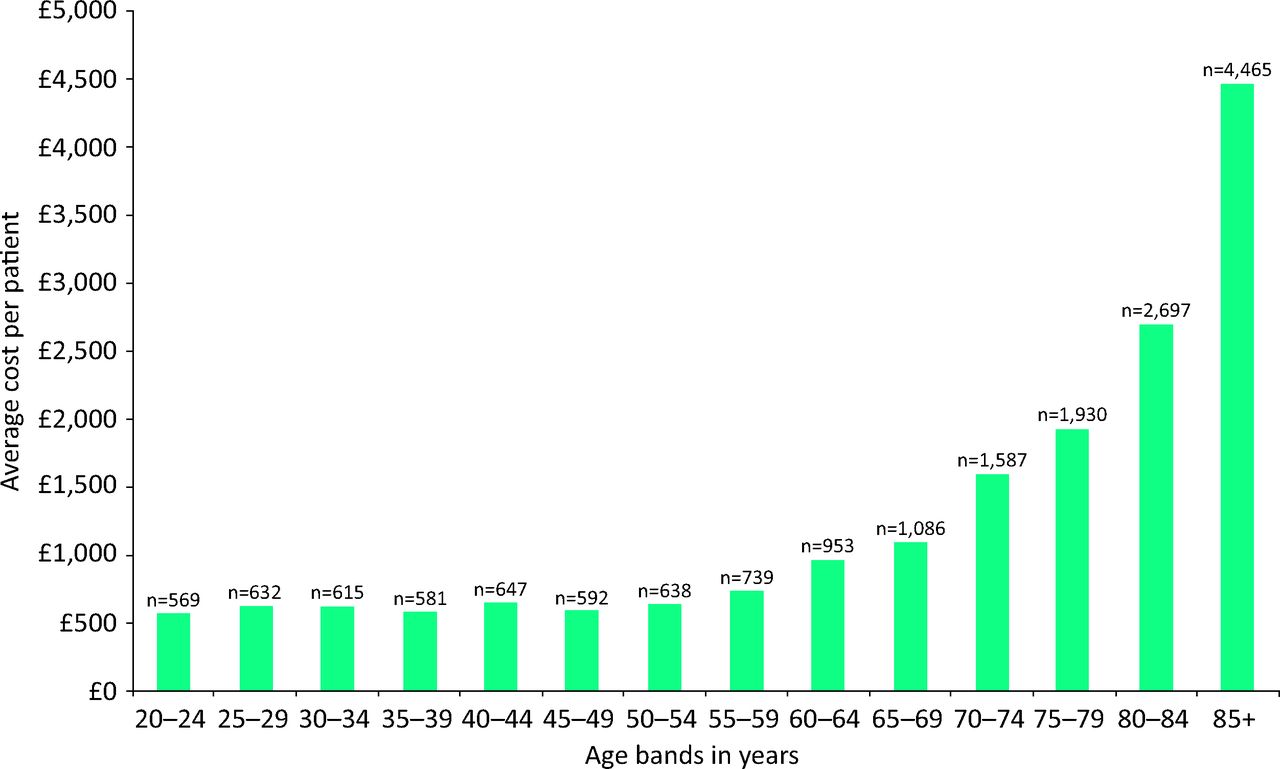
The data analysis also corroborated what many clinicians recognised: as comorbidities increase, the utilisation and cost per patient of providing acute hospital services increases. In primary care, both indices remain relatively stable. Moreover, the data reflect the experiences of the current health and care systems: that as patients’ needs become more complex, they experience many more hospital appointments as outpatients, more diagnostic tests and more frequent attendances and admissions through the ED. In summary, the DGH is effectively delivering a large part of the care for multiple long-term conditions in the most expensive part of the system. We should not be surprised at the operational and financial consequences that this produces (Fig 2).

Average cost of care by age band for the South Somerset population (from Symphony data set, South West Commissioning Support Unit).
Delivering new care models for the most complex patients
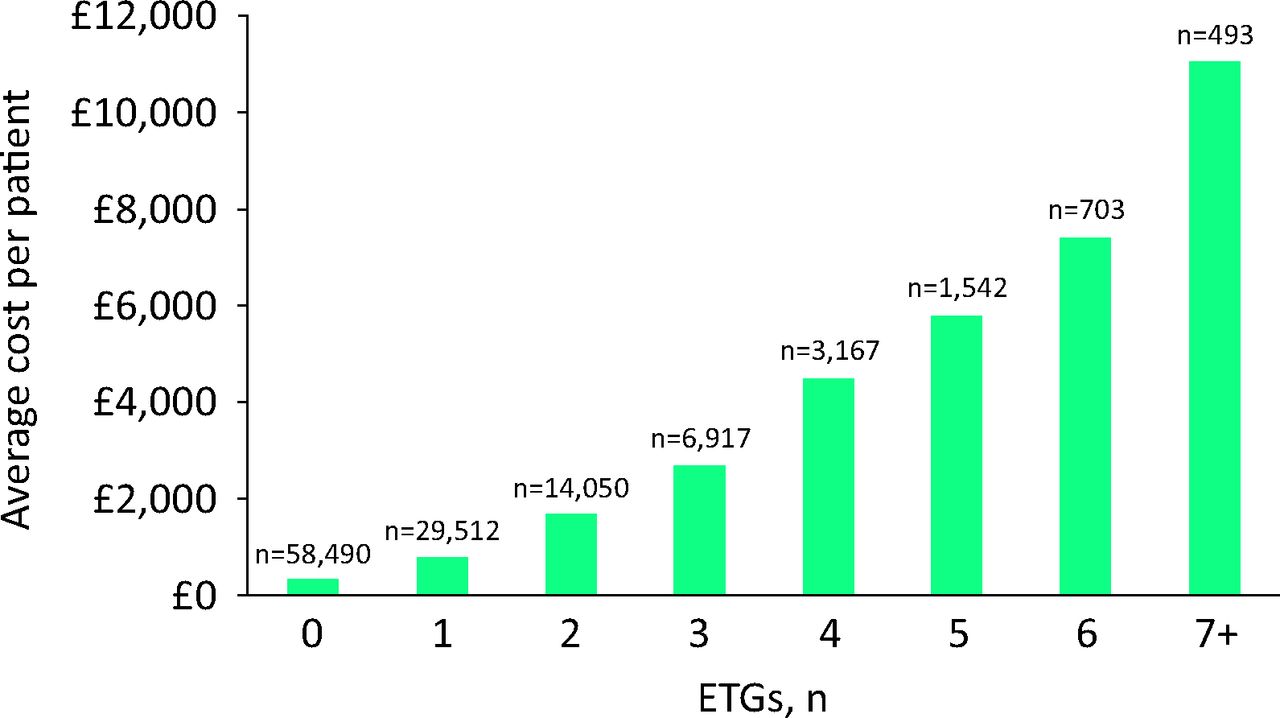
The analysis of the Symphony data showed the partner organisations that the traditional model of integrating care for specific disease pathways (diabetes, heart failure, chronic obstructive pulmonary disease) would not necessarily address the biggest challenge facing both commissioners and providers: the challenge of managing multimorbidity (Figs 3 and 4). A new care model is required for these patients, and this has been the focus for the past year. The model now being implemented sees the establishment of a ‘Symphony Hub’ that proactively coordinates and manages the care for the most complex patients identified from the integrated data set. Initially, a cohort of patients numbering some 1,500, drawn from across the GP practices in south Somerset, will be managed by a multi-disciplinary team of nurses, therapists, social workers and care coordinators. In addition, there will be medical staff working in the Hub who will provide medical oversight and care. It is this oversight that distinguishes the Symphony model from other integrated care models currently operating elsewhere.

Cost of care by setting for diabetes patients with an increasing number of other chronic conditions (expressed here as number of ETGs (from Symphony data set, South West Commissioning -Support Unit). ae = accident and emergency; cc = continuing care; cm = community services; ETGs =episode treatment groups. ip = inpatient; mh = mental health; op = outpatient; pc = primary care; sc = social care.
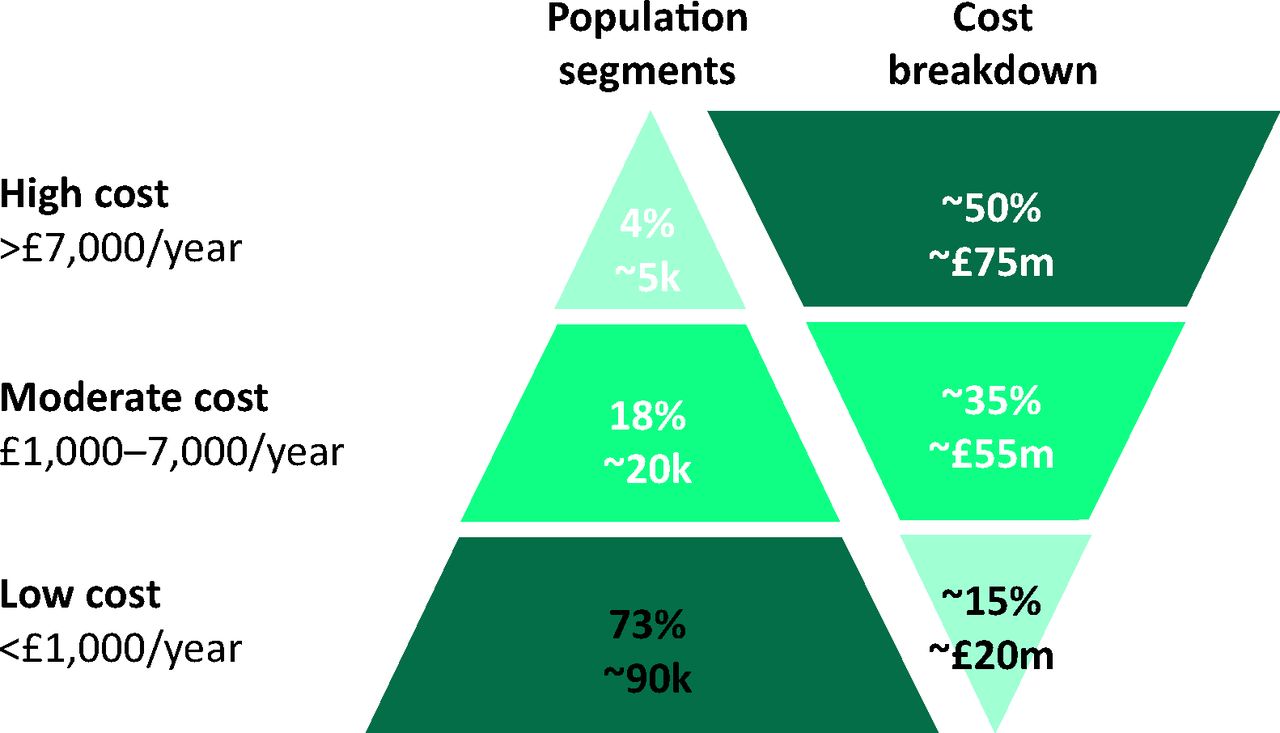
Breakdown of total health and social care costs for the south Somerset population (from Symphony data set, South West Commissioning Support Unit).
The Symphony Hub doctor or extensivist
Key to the new care model for the most complex patients is the Hub doctor, who will be employed by the hospital as the host provider for medical care and coordination. These interesting new medical roles have been open to hospital consultants and GPs to apply for; they have attracted, in particular, those who wish to develop their clinical skills in caring for complex patients. The Hub doctor will work closely with other members of the Care Hub team and will build strong links with hospital consultants, who will be able to support and advise on the care of these patients with multiple comorbidities.
Equally important will be the relationship between the Hub doctor and the patients’ own GP. Those managed through the Symphony Hub will remain on the practice list of their GP, who will continue to receive the capitated payment for their care. Understandably, there is a range of views within primary care about other medical professionals ‘taking over’ the care of their patients, but the aim of the Hub is to provide additional medical capacity to help in the management of complex patients who need a greater level of input and coordination than can be provided at present within the existing primary care model. The coordination of care between Hub doctor and GP will be crucial, and the fact that applicants for the Hub doctor posts are predominantly GPs will ensure that these doctors have a strong understanding of the potential issues and will actively share information with colleagues as to how patients’ care needs are being addressed.
Much of the thinking around these new medical roles has been based on research and examples from the UK and abroad. Both community and acute providers in Torbay have demonstrated the benefits to patients of integrating health and social care services in the community. Many integrated care systems in the UK have, however, struggled to engage and involve primary care clinicians fully in their integration efforts.
Models in the US, such as Care More (caremore.com) and ChenMed (chenmed.com), have had success in developing integrated care models. These models involve primary care clinicians in leading new care models to proactively manage the most complex patients on the state-funded Medicare and Medicaid programmes (Box 1). Such clinicians are often referred to as ‘extensivists’ and bridge the gap between acute hospital specialists and the local primary care doctor. The healthcare system in the US is clearly very different from that in England, but some principles from these models have guided our thinking locally and these critical factors have been fundamental to the design of the Symphony model now being put into practice.
Box 1. Success factors identified from US primary-care-led healthcare models for older people.

The role of the hospital specialist in integrated care
Development of the Symphony Care Hub is a real opportunity to utilise the expertise and skills of hospital physicians in a proactive and collaborative way. As the care of patients with complex conditions outside the hospital is improved, the role of the consultant physician will be to support their primary care colleagues by providing advice and specialist input into decision making.
YDH has already made significant progress along these lines with the establishment in January 2014 of a Frail Older Persons Assessment Unit (FOPAS). This development was designed to provide a facility where older patients, referred by their GP or attending the ED, can be assessed by a consultant geriatrician, nurses, pharmacist and therapists. The unit is away from the busy ED and is an ambulatory facility that is specifically designed to assess and discharge as many patients as possible back to their homes. The unit has proved to be very successful, with 75% of patients being discharged home the same day following a comprehensive geriatric assessment and all patients receiving a clear plan that is shared with the GP and community staff. The consultant also provides advice to GPs by telephone and will review and follow up patients who have been seen in the FOPAS as required.
This service has received very positive feedback from patients who are pleased to receive a rapid assessment and diagnosis and are usually able to return home the same day. GPs also value the ability to receive a comprehensive assessment of their patient and specialist advice on managing the patient in the community. The FOPAS service will provide an excellent specialist link to the new Symphony Care Hub, and as the first hub is to be co-located alongside the FOPAS, there will be ready access for the Symphony team to specialist geriatric skills.
Conclusions
The work of the Symphony project emerged from the recognition that existing models of care do not serve our patients well. Equally, staff across the system are frustrated with the unrelenting workload associated with managing patients who have reached a crisis point and require significant input either in primary or secondary care.
The traditional idea that the local hospital is the ‘provider of last resort’ is not sustainable, and if the system does not radically adapt, such institutions will not be financially or operationally viable. The approach of looking outside the physical boundaries of the hospital and re-thinking the entire healthcare system will produce an integrated and accountable care organisation, led jointly by clinicians from the hospital and from primary care, that will oversee the delivery of this and other care models locally.
With a detailed understanding of patient populations, and with clinical commitments to improve both services to patients and leadership across the system, improvements in both quality of care and in the efficiency of resource utilisation will be secured, along with the future of the DGH.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.