
ABSTRACT
General hospitals in Singapore are undergoing a process of transformation, from being siloed providers of acute care, into vital hubs of a regional health system that integrates community and hospital-based care to meet the health and social needs of the population. Collaborations between the acute hospitals and other community providers, such as primary care and nursing homes, have been strengthened through clinical leadership supported by government policies that enable the sharing of key hospital clinical resources throughout the community. These collaborations have enabled better use of hospital resources while strengthening the capabilities of regional healthcare providers. Successful collaborations are propagated through the use of an intermediary enabling national agency. This paper outlines the journey that has been undertaken thus far and provides a few examples of how acute hospitals have begun to refocus their attention towards a new paradigm of care. The initial experiences and key lessons will be useful in the planning of a new ‘greenfield’ hospital campus designed from the ‘ground up’ which will embody these key principles of the hospital of the future.
Journey from a soloist to an ensemble member
The wisdom of John Donne's words – ‘No man is an island, entire of itself’ – apply more truly today in healthcare than ever before. Patients present with increasingly complex needs, and are often on a chronic healthcare journey interrupted by unexpected ‘bumps’ of acute exacerbations, with needs that straddle health and social spheres. No sole healthcare entity, no matter how dedicated and learned, epitomised in the acute hospital of today, can singlehandedly meet all their needs over time.
The journey that has been undertaken by Singapore in recognising this evolution is, in many ways, an expression of the principles articulated in the report of the Future Hospital Commission of the Royal College of Physicians; recognising the future roles of the general acute hospital as sitting at the hub of a new ecosystem of care, improving collaboration across health and social care delivery, and acting as an agent for improvements in public health.1 As in the NHS, acute hospitals and medical specialists in Singapore have had the lion's share of the public healthcare budget, justified as necessary to allow the building and concentration of critical knowledge, infrastructure and technologies, to effectively and efficiently provide care for the population. After decades of investment, this strategy has enabled public acute hospitals in Singapore to provide high quality healthcare at a relatively low cost while achieving world class healthcare outcomes.2,3
However, this focus on funding acute hospitals has led to a disproportionate strengthening of tertiary and secondary as opposed to primary care, and often at the expense of non-acute hospitals and other community care providers. The unexpected result has been that acute hospitals in Singapore have been seen as the critical provider that patients and caregivers turn to in times of need, rather than as one component of a larger healthcare ecosystem.
As elsewhere, financing has been the critical lever used to shape behaviours of both providers and patients. Singaporeans enjoy free choice in this regard, with providers paid on a fee-for-service basis. This has resulted in a highly competitive private and public sector market that curbs healthcare cost inflation and which has kept care quality comparable between healthcare institutions. For more costly specialist and community care options, gatekeeping based on assessed needs by care providers is used to ensure that the services appropriately meet the needs of these patients. Excessive out of pocket costs are mitigated through a combination of government subsidies, mandatory insurance and personal health savings accounts. However, this combination of fee-for-service and patient choice has also provided incentives to expand the service offerings of each acute hospital while discouraging integration of care with other healthcare entities.
The general hospital within a hub of healthcare services
To address this concern, there has been a paradigm shift in government policy in recent years towards regional health systems (RHS), of which there are six in Singapore. They are envisaged as facilitated networks that will enable the integration of healthcare entities within a defined geographical region; allowing acute hospitals, primary and community care services to deliver seamless, hassle-free and patient-centred care. Leadership, resources to build and augment healthcare delivery capabilities, and the ability to coordinate information flows across the region are all essential prerequisites of any integrated care delivery system. In the Singapore context, it has been decided that the public sector acute hospitals are best equipped to meet these requirements, and hence serve as the hubs of the RHS. The hospital clinical and administrative leadership typically initiates and organises the key activities that need to be undertaken to bring all the key stakeholders together, forge a common and aligned purpose and work towards an agreed set of goals and objectives in the RHS.
Providing leadership
Hospitals are landmarks in communities, with organisational and clinical governance structures that generate confidence for funders, community partners and patients in the quality of care provided. Hospital utilisation records provide insight concerning populations of patients with the highest clinical needs and facilitate the targeting of interventions. Together, these give the acute hospitals the first place among equals in any regional health system. The acute hospital also acts a regional beacon for promoting public health in the community. An example is the Mini-Medical School Forum organised by one of the public acute hospitals in Singapore. This is a health education programme with a distinctive ‘hospital twist’ which aims to educate the public on ageing-related and caregiver issues. Each run of this programme involves a series of three weekend seminars held by a multidisciplinary team of hospital faculty involving specialist, primary care practitioners, nursing, and allied health professionals. The seminars aim to equip the public with knowledge and skills to cope with medical conditions common in ageing, such as hypertension, diabetes mellitus and osteoporosis. Each round of this programme has been consistently oversubscribed. These efforts complement population screening efforts jointly organised by the hospital and community to identify persons with chronic diseases. The acute hospital is able to further augment these efforts through targeted follow up, and by targeting future sites of potential population screening based on observed geographical variation in disease prevalence. Another innovative programme leverages on recruiting volunteers in neighbouring households to augment the care of frail patients to prevent unnecessary readmissions.4
Building up and augmenting community services
The specialist and multidisciplinary resources present in the acute hospital provides opportunities for them to strengthen the capabilities of community partners, and to augment the provision of services in areas that these partners are unable to fulfil. For example, a programme based in an acute hospital taps on its strength in geriatrics to bolster the capabilities of nursing homes in the region. Geriatricians and hospital-based clinical teams provide training and guidance to nursing home care professionals to improve the management of their more complex patients. This training is further enhanced through a teleconference system. The system allows multiple sites to benefit simultaneously, enabling hospital specialists to participate in multidisciplinary team meetings to discuss care plans, and permiting both scheduled and ad hoc consultations with specialists. This has improved staff and system productivity, and reduced the need for patients in nursing homes to be transferred back to the acute hospitals for follow-up clinic appointments.5
Collaborations to build capabilities do not only exist in the community sector but also in primary care. Hospital specialists have started to form collaborations with primary care practitioners to provide specialist advice on more complex patient management issues. These extend from emergency physicians providing advice on the management of injuries, to organ-based specialist advice relating to chronic disease management. These collaborations have enabled these patients to be cared for at locations where their needs are best met.6,7
The acute hospital is also well poised to plug gaps in the healthcare ecosystem through directly augmenting community service provision. Realising the needs of vulnerable patients in the immediate post-discharge phase, some of the acute hospitals have commissioned specialist home care teams. These teams are led by hospital-based doctors drawing on a multidisciplinary team, including nurses and therapists, to enable patients to be cared for at home safely in the immediate post-discharge period. Such patients typically have care needs, such as complex wound management, or require specialist review of cardiac or respiratory failure after transfer home.8,9
Improving information flow across health and social care
The increasing frailty of the rapidly ageing Singapore population means that there is a growing need for a seamless flow of accurate information from acute hospitals to patients, and their families and community care providers. Hospitals in Singapore have employed care coordinators, usually with a clinical background, to assist patients with complex health and social care needs who may be identified through past utilisation data, and who would be assigned to a coordinator to augment the clinical team in the identification of potential challenges upon discharge; linking these patients with appropriate health and social community resources facilitates smooth discharge home. These patients often have medical needs complicated by social care issues that require sharing of care plans and goals not just with patients and their families, but also community-based health and social care providers. These follow up the patients post discharge to review the progress of care plans and address new concerns by the patients. These initiatives adopted from international models have been validated and shown to reduce hospital utilisation in Singapore.10
Apart from addressing needs of patients when admission is needed, some hospitals in Singapore have taken a more proactive approach to facilitating information flow by staffing community nurse posts to create health ‘touch points’ within the community. These posts, staffed by nurses rotated from the acute hospital, enable patients to get basic health assessments and referrals to appropriately needed community resources. This system allows these nurses to practice to current standards of care, but also enables them to better appreciate the challenges faced by patients across the entire care continuum.
Role for a national care integrator
Many roles of the acute hospital as a hub of a healthcare ecosystem described have been developed through the passion and drive of clinician leaders in each institution. One of the key challenges faced was the institutionalisation and promulgation of successful and sustainable models across all six RHS. To address this concern, the promulgation of ideas was assigned to an independent entity, the Agency for Integrated Care (AIC), tasked with the role of being the national care integrator. In this function, the AIC acts as an advocate for care integration, helping to consolidate the best practices in integration from one RHS and sharing it with the others. The AIC also drives the development of professional capabilities within the primary and community care sector so as to enable the acute hospitals to work collaboratively on an ‘even keel’ with their partners. The current strategy map of AIC demonstrates the need to integrate multiple cross-cutting tracks to achieve its vision (Fig 1).
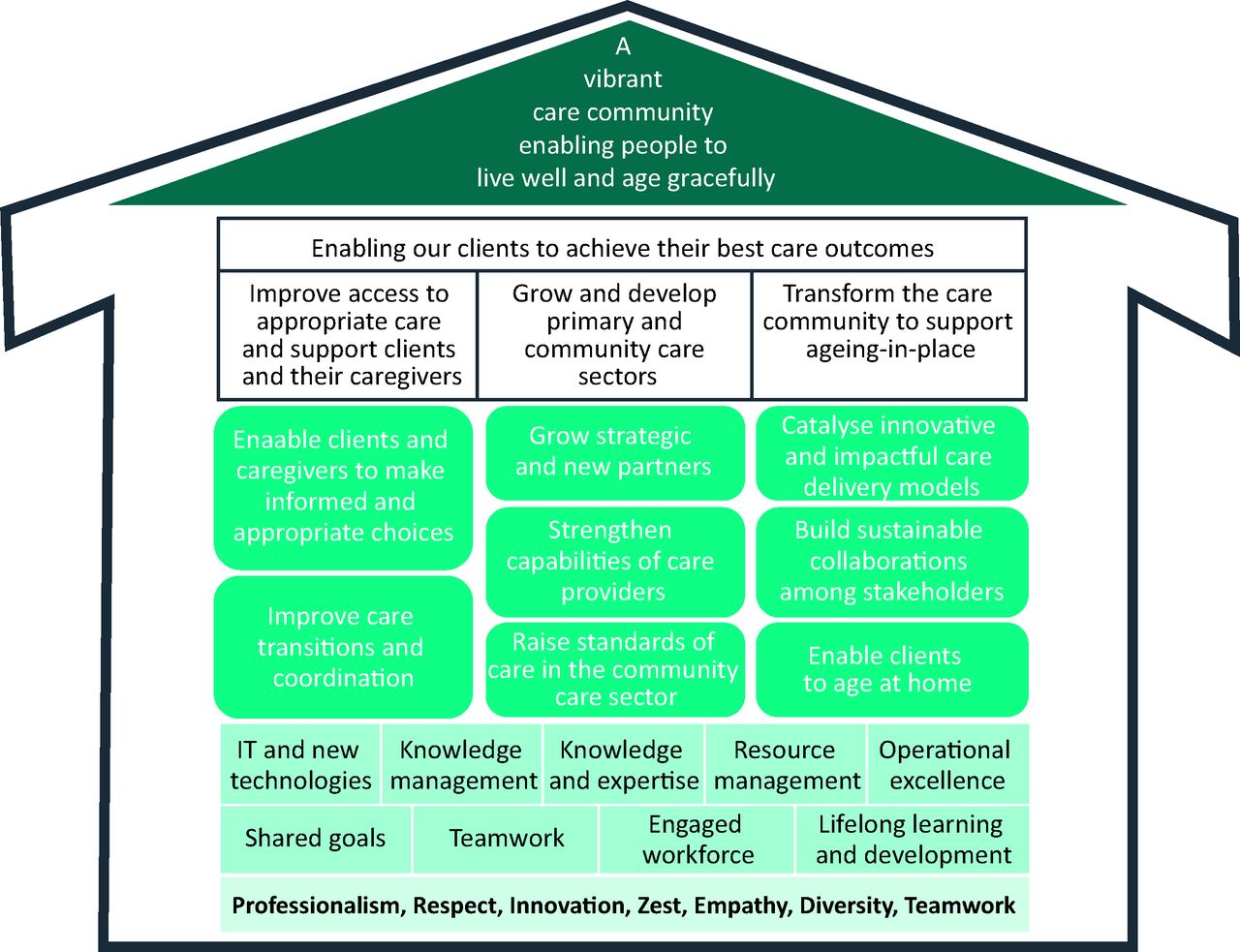
AIC's strategy map. Map indicates the need for multiple tracks of work needed to create an integrated healthcare system.
Challenges faced in care integration
The shift in the acute hospital paradigm, from playing a soloist role to being an ensemble performer, presents challenges at the hospital, regional and structural levels which need to be addressed. Hospitals require their identities and mission to evolve. Addressing this challenge starts with strong clinical and management leadership but also requires structural changes in the education and training of clinical staff. A key step undertaken to address this is the reorientation of the hospital's own staff so as to shift their focus away from an infrastructure centric view of care, to a patient centric and holistic view of care.
The second challenge is building a trusting network of partners within the healthcare ecosystem. Partnerships are critical in establishing this new role of the acute hospital as a care hub that requires different agencies communicate with each other and exchange information relating to care plans and goals. Regular, formalised community partner sharing sessions organised by the hospital, engage with the community not just at the leadership level, but also at the operational or staff level.
The third challenge is the creation of effective system enablers for care. These include financing reforms and more efficient and effective systems for information exchange. Trials of new funding systems, to create flexibility for hospitals and other care providers to efficiently meet needs, are underway. These experiments in new financing approaches involve some form of population-based capitated funding. To facilitate information flows, the government has created a national electronic health record that has been further augmented through regional systems to communicate care plans.
Future directions
The recommendations of the report of the Future Hospital Commission focus on the care model within the hospital, but also force a fundamental rethink of its role within a healthcare ecosystem delivering safe, high-quality sustainable care centred upon the needs of patients. The challenges identified need to be continually addressed on a hospital, regional and national level. While existing hospitals continually develop new solutions and adapt existing processes and infrastructure to meet these needs, the capacity to change is moderated by existing frameworks of care within a hospital.
In Singapore, a brand new hospital campus is being built from ‘ground up’ to operate as an ensemble performer. The campus has been designed to integrate with the future capabilities of other care partners in the community to deliver care. Planned to be open from 2022, this integrated health campus will be at the heart of an ecosystem of care, bringing together all the key providers in the community to deliver coordinated, holistic, person-centric care to the population. The authors look forward to sharing this exciting journey and experience of designing and implementing these new models of care in a future issue of the Future Hospital Journal (Fig 2).

Preliminary artist impression of campus. Reproduced with permission from SAA Architects Singapore.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- Journey from a soloist to an ensemble member
- The general hospital within a hub of healthcare services
- Providing leadership
- Building up and augmenting community services
- Improving information flow across health and social care
- Role for a national care integrator
- Challenges faced in care integration
- Future directions
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.