
OVERVIEW
Much has been discussed and written about the events at Mid Staffordshire Hospitals which led to the Francis Inquiry. The quality of leadership then and now has formed much of the debate. This short paper discusses some of the analysis of both Francis inquiries and seeks to understand the impact that these reports have had on the quality of leadership and the legacy from the mistakes documented at the time. Has the system which allowed the events at Mid Staffordshire to happen changed sufficiently to create a climate where the right leadership behaviours are allowed to flourish? Have we learnt the lessons from those inquires?
Introduction
Robert Francis QC published his first report into the Mid Staffordshire NHS Foundation Trust in 2010.1 The inquiry followed concerns about standards of care at the Trust, and an investigation and report was published by the Healthcare Commission in March 2009. The inquiry team heard a significant amount of evidence from patients, their relatives and staff and the final report included 18 recommendations for change (dwarfed by the 290 recommendations he made in his second report published some three years later). At the time of publication of his first report the Department of Health and the board of the Mid Staffordshire Trust accepted the recommendations of the inquiry in full. In his report, Francis referred to ‘an atmosphere of fear of adverse repercussions’ and a ‘forceful style of management’ contributing both to the lack of care and the lack of peer responsibility for raising concerns. In an interview with Channel 4 at the time he referred to the views of the senior leadership team of the Trust feeling like they were ‘in the premier league – they didn't listen to patients and staff. Leaders who behave like that won't stay like that for very long’.
A consistent theme during this whole period, and cited in both Francis reports and those published shortly afterwards, was the poor quality of leadership, both within the organisation and the NHS as a whole. NHS management and leadership has always been a contested area. There has been a longstanding recognition that a top-down, performance-driven culture will not produce the climate that creates the conditions for success. Francis emphasised this in both his reports. The Health and Social Care Act distracted from the issue. So what of leadership post-Francis?
An examination of some of the evidence from the time of the first inquiry up to immediately prior to the 2015 general election tells a difficult, inconsistent and unequal story of the state of leadership then, now and for the immediate future.
The publication of Francis’ first report was taken seriously by the then NHS chief executive, Sir David Nicholson, who immediately wrote to all NHS chairs and chief executives urging every NHS board to read the report and to ‘review your standards, governance and performance’.2 In the letter he also stated that the National Leadership Council (a council he chaired) proposed a new system of professional accreditation (in light of one of the recommendations in the inquiry report) and an undertaking to review the arrangements for the training, appointment, support and accountability of executive and non-executive directors of NHS trusts and foundation trusts. Accreditation of managers is still being discussed in the NHS but to date no action has been taken. Local responsibility for enacting any changes suggested by the report was key, and national action was also going to be taken to ensure this had been put in place. Accreditation of managers at the time suggested a concern about management competence and capability.
The lack of a public inquiry frustrated those who had been vocal in calling for an inquiry into the events at Mid Staffordshire. ‘Cure the NHS’, a patient pressure group established by Julie Bailey, the daughter of one of the patients who had died at Mid Staffordshire, spoke frequently and publicly about her frustrations with the initial Francis report. On 9 June 2010, very shortly after his appointment, the secretary of state for health, Andrew Lansley, announced a full public inquiry into the role of the commissioning, supervisory and regulatory bodies responsible for the monitoring of Mid Staffordshire Foundation NHS Trust. The focus away from the work of the hospital in isolation to other broader considerations was significant and during his parliamentary announcement Lansley specifically asked that the inquiry look into ‘how it was allowed to happen by the wider system’.3 The clear implications of the Inquiry were that the failures in care experienced at Mid Staffordshire were not restricted to the mismanagement of one organisation but that they were symptomatic of a broader set of issues and concerns in the way this system operated and their impact on leadership behaviours.
On election in government Lansley had already been shadow secretary of state for health for six years and rapidly produced his first white paper in July 2010. Equity and excellence: liberating the NHS was a comprehensive and detailed white paper that represented a hugely significant shift in focus for the NHS. Much of the focus lay in the shifting of power from the centre to local commissioners and specifically the general practitioner community. He stated:
The headquarters of the NHS will not be in the Department of Health or the new NHS Commissioning Board but instead, power will be given to the front-line clinicians and patients. The headquarters will be in the consulting room and clinic. The Government will liberate the NHS from excessive bureaucratic and political control, and make it easier for professionals to do the right things for and with patients; to innovate and improve outcomes. We will create an environment where staff and organisations enjoy greater freedom and clearer incentives to flourish, but also know the consequences of failing the patients they serve and the taxpayers who fund them.4
Although no reference was made to the Francis report in the white paper this shift of power and responsibility, and the apparent focus on patients were entirely in line with Francis’ recommendations. The subsequent impact on leadership behaviours, the context in which leaders operate and the culture that led to some of the issues at Mid Staffordshire has not been as implied in the recommendation.
To understand the reality of leadership at senior levels in the NHS at the time we need to look to the few pieces of work commissioned in this area. The National Leadership Council, chaired by the chief executive of the NHS, had been a further national attempt to steward leadership development activity across the NHS. Following on from predecessor organisations, including the Leadership Centre (2003), the NHS Institute for Innovation and Improvement (2006) and many more before, the Council had a broad remit that included clinical leadership, board leadership, new leaders and a newly established Top Leaders programme, created to address perceived succession planning and talent management deficiencies that led to an undersupply of applicants for chief executive and executive directors in larger provider trusts. The long history of development activity and frequent restructuring of the national architecture for this work suggest that not only had an awareness of the importance of management and leadership been around for some time, there was also an awareness from some of the most senior leaders in the system of the need to make changes.
The NHS Top Leaders programme included a personal diagnostic element. The diagnostic was developed in 2010 for the NHS by the Hay Group to assess the capabilities and potential of those people considered to be top leaders within the NHS. Participants in the programme were nominated by chief executives of the then Strategic Health Authorities and were those who were in ‘enduringly complex roles’ leading significant NHS organisations. The diagnostic consisted of five elements: i) a bespoke Top Leaders leadership 360 degree survey; ii) an inventory of leadership styles; iii) an organisation climate survey; iv) verbal and numerical reasoning tests; and v) the Dimensions test of Talent Q producing a ‘derailers report’ and summary of individual team preferences.
An interim report of the early composite findings from 156 initial participants was produced in 2010 and gave a stark account of the behaviours, preferences and abilities of the senior NHS community. The initial report included most members of the NHS executive team who had been instructed to engage with the diagnostic by their chief executive. It also included chief executives and directors from across the NHS, from all organisation types, all geographies and all professions.
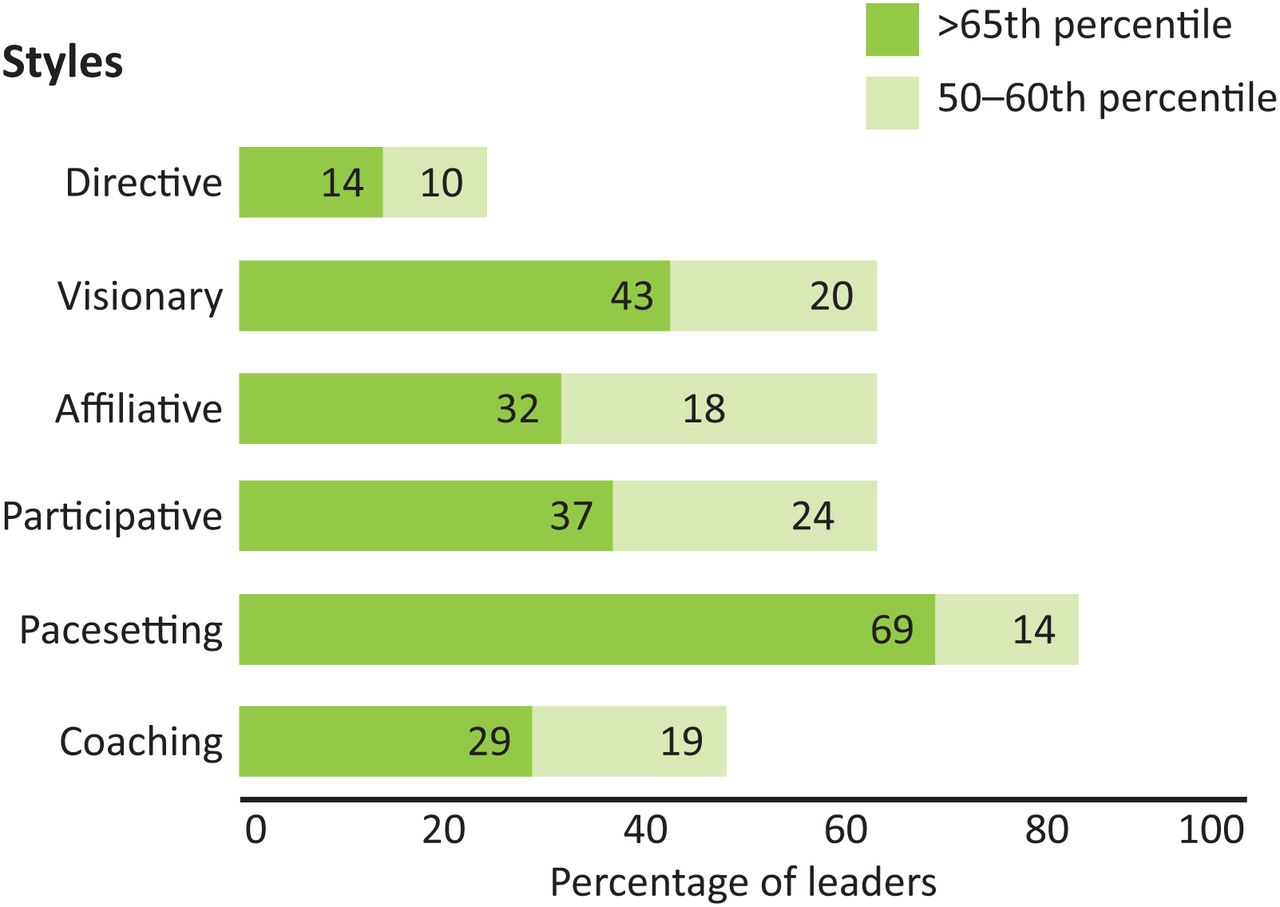
Of the styles and climate elements of the diagnostic there were three significant indications. The first was that of the early adopters of this diagnostic there was a remarkable convergence in both the narrowness and style of leadership they adopted: 69% of those in the survey reported as having a ‘pacesetting’ style of leadership with a further 14% declaring it to be their most common secondary style (Fig 1).

Composite NHS top leaders (n = 156).
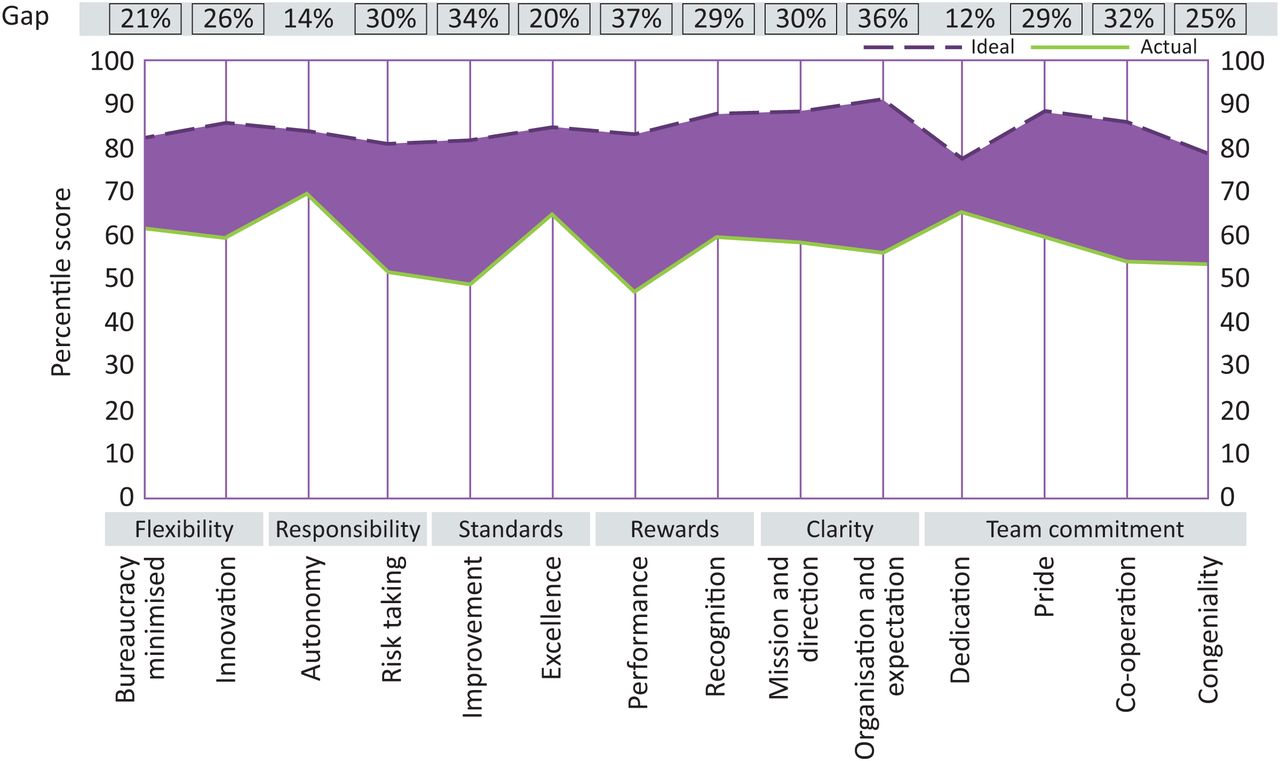
The survey also reported on the working climate experienced by NHS Top Leaders (Fig 2) and the climate that those working to them reported (Fig 3). These figures tell a similar story; NHS leaders and their staff were working in an environment that was described overall as ‘demotivating’ and for the most senior leaders at least was combined with a limited range of leadership styles dominated by more command and control behaviours.
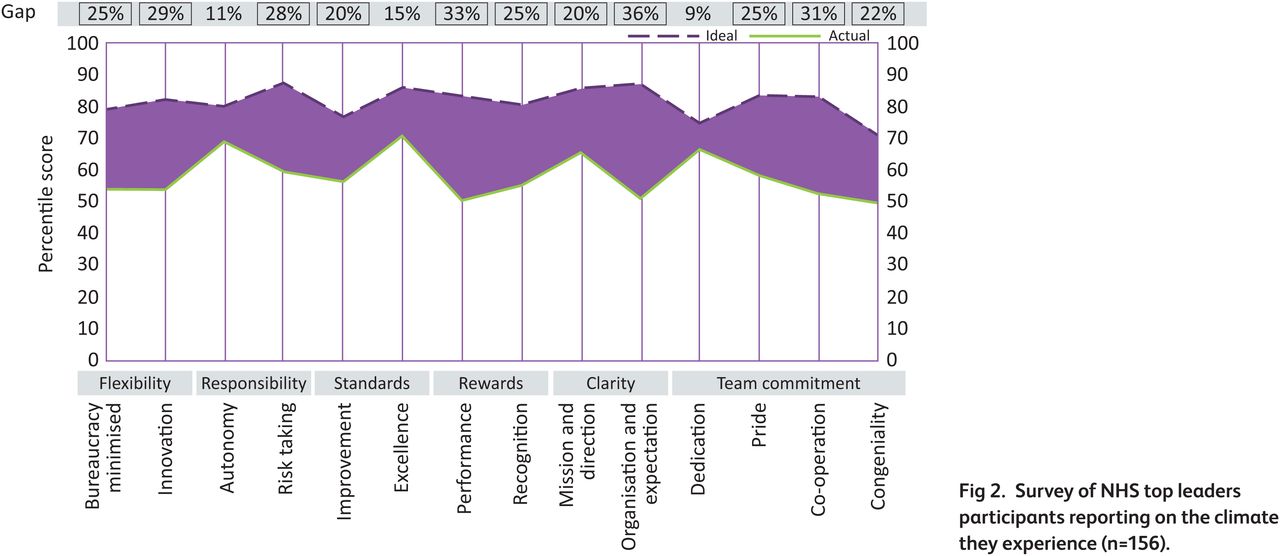
Survey of NHS top leaders participants reporting on the climate they experience (n = 156).
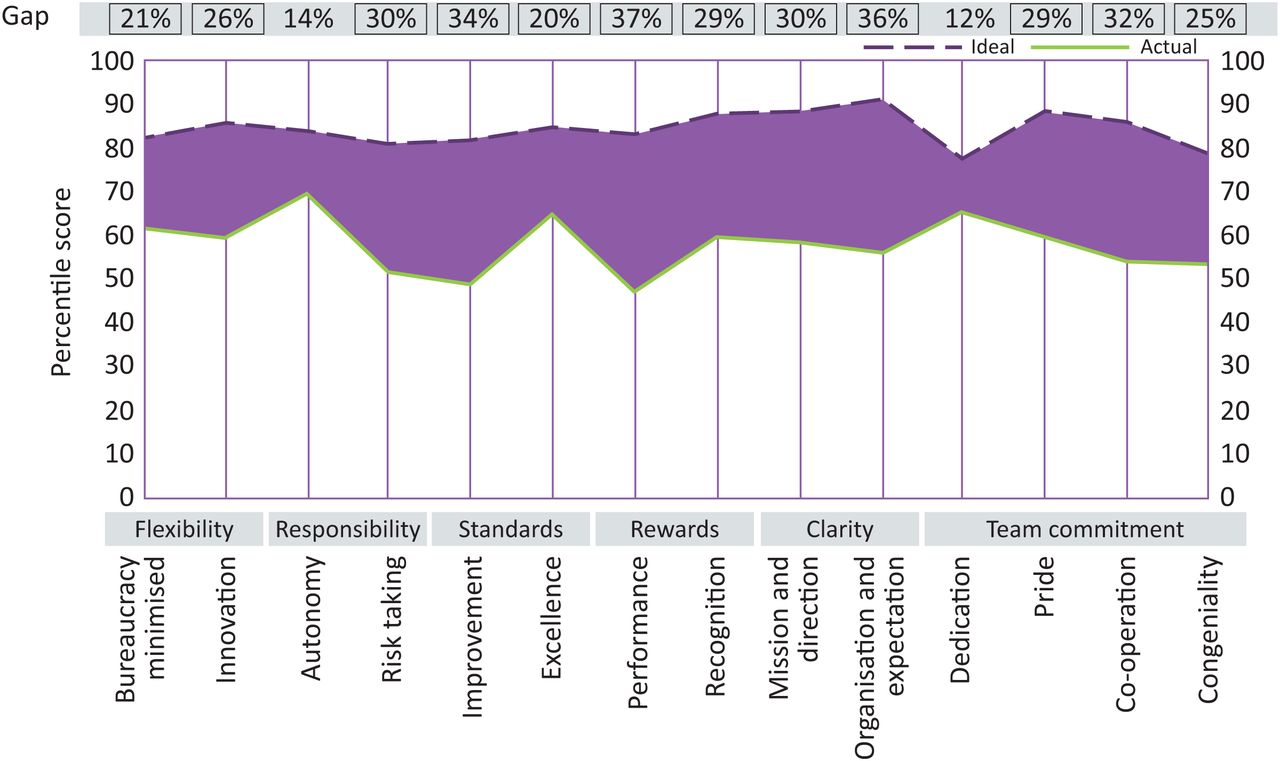
Survey of NHS Top Leaders direct reports and colleagues on the climate created by those participants (n = 858).
The behaviours required to provide the focus that Francis identified and recommended were not present in sufficient measure. There was still an overriding focus on targets and performance. There was a strong preference for top-down management. The actual climate being created fell short on most elements of the required dimensions. Key to both was the misalignment between the nature of performance measurement, performance reward and an espoused focus on quality of care.
This assessment of the state of leadership in the NHS at the time was shared by others. The 2011 King's Fund report from their commission on leadership called for the NHS to shift from the old ‘heroic’ model of leadership to make way for a more inclusive form of leadership.5
The authors describe the results of their inquiry into NHS leadership in the wake of Francis, alongside the pressures associated with impending austerity and restructuring demanded from the coalition government.
The report suggested the NHS was under managed — having many fewer managers than comparable industries and other health systems — but that it might be over administered because of the demands for reporting up the complex hierarchy.
However, it also referred to the enduringly populist assessment of the over management and over bureaucratisation of the NHS:
The public is no more sympathetic. Perhaps it takes its cue from the political attacks on bureaucracy. A recent poll conducted by Ipsos MORI (2009) showed that 85 per cent of the public supported proposals to reduce the number of managers in the NHS by one-third.
This position remains popular still. Speaking on the Andrew Marr show in May 2015 Simon Stevens, chief executive of NHS England, was asked by Andrew Marr whether one of the problems of the NHS was the over burdening of managers and administrators.6 The rhetoric remains constant.
In their 2011 report the King's Fund also rejects the arguments for ‘super-heads’, a notion borrowed from Gove's application of the term in education, saying that leadership experts have moved from a ‘great-leader’ to a ‘post-heroic’ model, which would be much more relevant to how the NHS now works.5
After an extended period of consultation on the white paper of 2010, including a listening exercise, the final Health and Social Care Act was passed in 2012.
Almost 12 months later and 3 years after it was commissioned, the final report of the Mid Staffordshire NHS Foundation Trust Public Inquiry was published on Wednesday 6 February 2013. This second report, now public, emphasised the role of leadership in prioritising patient safety and in listening to and learning from patients. It was comprehensive and included 290 recommendations, 204 of which were accepted fully. The initial government response to the report was published in March 2013. Patients first and foremost7 opened with a comprehensive statement of common purpose signed by the then heads of the 14 national organisations across health and social care. Stephen Thornton, then chief executive at the Health Foundation however noted that:
The Government's response to Robert Francis QC's report is still unfortunately rooted in paternalism and the overriding ethos is of the patient being ‘done unto’ rather than being in active control. There must be a deep top-of-the-office commitment to the fully engaged patient, to transform the NHS into a service that puts patients first and foremost.8
In addition to their own initial response the government commissioned six independent reviews to consider some of the key issues identified by the inquiry. These included: an independent review led by Camila Cavendish into healthcare assistants and support workers in the NHS and social care settings; a review into the quality of care and treatment provided by 14 hospital trusts in England led by Professor Sir Bruce Keogh, medical director at NHS England; a review of patient safety in the NHS led by Professor Don Berwick;9 a review of the NHS hospitals’ complaints system led by Ann Clwyd MP and Professor Tricia Hart;10 a review of the bureaucratic burdens placed on NHS providers by national bodies by the NHS Confederation;11 and a review into care for children and young people co-chaired by Professor Ian Lewis and Christine Lenehan.12 All these nationally commissioned reviews, involving some of the very most senior and experienced leaders across health (many beyond the boundaries of the NHS in England) were to provide advice, recommendations, and instructions to those in leadership roles about what they could do better, differently and more compassionately.
The recommendations from most of these reports appeared well aligned. They referenced a need for more support in training and developing leaders and managers, a greater involvement of clinicians in leadership and a rejection of the blame culture that was felt to be a threat to improving patient safety and quality of care. In essence, all the totems and symbols of a different culture (with devolved, distributed and collective leadership) hinted at by Francis. However the reviews and subsequent suite of complex recommendations and actions still reflected more of the same: one in which leaders should be instructed how to behave, how to act and how to be measured.
In a national strategy for nursing published in 2014, NHS England noted this and stated:
The Francis Report, the Keogh Report, and the Berwick Review into patient safety point to the multitude of factors that led to nurses, doctors and managers losing sight of quality and the need to learn lessons from these failings. The response: a re-dedication of the NHS to living its core values, with compassion being central within this and policymakers, commentators, conferences and blogs making genuine personal and organisational declarations that we can and will do better.13
A patient perspective was articulated by a National Voices paper on ensuring safe and high-quality patient care.14 They shared their plea that:
At the local level every health professional, every organisation and every professional and leadership body needs to reflect on how they can improve the safety and quality of the care for which they are responsible, in the light of the Francis recommendations. Trust boards need to be clear whether they are recruiting, training, deploying and supporting staff well enough to ensure the delivery of safe, effective and compassionate care.
In response to both political and economic changes and following data from the initial composite assessment of senior leader's diagnostics, the NHS Leadership Academy commissioned a review of its leadership model. One conclusion prompted the authors to note that:
In professional service organisations such as the NHS there is an understandable leaning towards shared forms of leadership. But confusion has arisen about ‘distributed’, ‘dispersed’ and ‘shared leadership’ as counterpoints to top-down, ‘heroic’ leadership. While shared leadership has been productive, the idea has unfortunately also led to a lack of clear thinking about the role to be played by those persons occupying leadership positions.15
The confusion regarding leadership at every level, the responsibilities of frontline staff to lead and the need to engage patients in leadership of design, delivery and ownership of their care, intended to address the failures of previous regimes, leads to a need to reflect upon what the new role of senior leaders is.
The government response to the Mid Staffordshire NHS Foundation Trust Public Inquiry, Hard truths: the journey to putting patients first16 reflected the general unease about the reality of the necessary changes to leadership culture being delivered by the leaders themselves. This view appeared to be shared by most analysts and commentators in 2013. Demonstrating a lack of confidence in leaders managing the shift, so well described by the various inquiries, reports, commissions and commentaries, the initial recommendations in the government's response were largely comprised of national, ‘top-down’ regulation and inspection actions.17 The recommendations suggested a reinforcement of the kind of structures and processes that had been cited in the Francis report as being responsible for the over reliance on assessment as a means of delivering great care. The Nuffield Trust report shared this view saying respondents reported that national bodies had persisted in some of the behaviours towards hospitals that had contributed to the problems identified by the two inquiries. This is a theme echoed coincidentally in the recent Point of Care Foundation report.18 The difficulty here is that the national body response tends towards hard or mechanical interventions rather than addressing the issues raised as ones associated with complex adaptive human systems, ie those related to behaviours, culture and leadership. 19
In 2013, the Hay Group followed up their initial analysis of Top Leaders diagnostic data from 2011 with a report on 758 senior leaders, including chief executive or board level members of primary care trusts, large acute trusts and pathfinder GP commissioners. The results were broadly similar to those from the initial survey two years earlier, suggesting very little had changed in leadership over the intervening period. Rather than focus on culture, leadership development and leadership excellence, the system had once again focused on restructuring, reorganisation and reform.
In 2014, the King's Fund conducted a further survey into the culture of leadership in the NHS. The survey of 2000 managers and clinicians asked their opinions on culture, compassionate care and leadership in the NHS and revealed that although things had improved since the 2013 survey ‘a majority still believe the quality of leadership is poor or very poor’ and more worryingly that ‘The survey consistently revealed a difference between the views of executive board members and the rest of their organisations. This suggests that boards are not in tune with how staff are feeling about their organisation’.20
The Health Foundations report published around the same time (a year after the second Francis report) shared the King's Fund assessment that frontline staff in particular appeared less engaged and supported, and had less control over changes in the culture that were needed. They stated:
Our analysis suggests that only 44 of the 290 recommendations from the second inquiry – that's around 15% – are solely within the remit of NHS organisations to do something about, and only an additional 7 can be addressed by staff at the front line.21
The King's Fund report of later that year concluded similarly, that important changes were needed for frontline staff as well as for the most senior: ‘Every interaction by every leader at every level shapes the emerging culture of an organisation’.22
So now what for leadership?
In 2015, Laura Bridges from Ipsos Mori noted that the indications are that the public perceive very little change to have occurred at all:
And the public believe that Mid Staffs was not an isolated incident. Most (92%) think there is a tolerance of poor standards in at least some hospitals. Over half (52%) of people blamed NHS managers for the patient care problems at Stafford Hospital – a far higher proportion than those who blamed nurses (7%) or doctors (3%).23
We know well what failure looks like. We have put in place ever more onerous and burdening assessment, regulation and monitoring of the quality, safety, efficiency and effectiveness of care. In part because self-regulation and peer assessment had not been seen to work, it did not prevent the mistakes at Mid Staffordshire. Leaders in the NHS are acutely aware of their responsibilities, and at a senior level, the consequences for failure to discharge their duties or to make mistakes that may have unforeseen or tragic consequences. Berwick's plea for a service without harm included a ‘no blame culture’, one which is not reflected in the numerous surveys about the culture of leadership in the NHS described above.
What is needed is a shift in approach to developing and educating our leadership community. Rather than assume that these ever more complex skills can be all acquired in role, the NHS needs to invest to ensure it has a staff group with such crucial responsibilities properly equipped to lead care. As the NHS moves into a fiscal year that is likely to be even more pressured than the last, facing a very clear requirement for marked increases in productivity, efficiency and effectiveness, and increased regulation and assessment, the conditions that Francis described about the ‘system’ in his second report appear as top down as ever.
To move away from this approach requires leaders at every level who are able to expertly navigate their roles and responsibilities with confidence and competence. Only this will shift the perceptions of the public, provide a service that is less likely to induce harm and create a continuously improving, compassionate healthcare environment.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
{kind=link}