
ABSTRACT
A significant number of medical admissions and inpatients on general wards are unstable or have unmet medical or nursing needs. Ward-based physiological scoring (early warning scores) and similar innovations aim to identify those who may merit enhanced care, and initiatives such as ‘comprehensive critical care’ describe a whole system approach to this group. While the recommendations in this 15-year-old document have been largely accepted and implemented, the Future Hospital Report recognises that close cooperation between acute medicine and critical care is essential but lacking in many institutions. Much of what follows is opinion and conjecture as there is little hard data to refer to. Although an anaesthetically trained intensivist, I have been a member of the Society for Acute Medicine since its inception and have sat on Council since then as critical care representative. I was also the clinical director for acute medicine in Norwich for three years.
Introduction
Critical care as a speciality is relatively young, tracing its origins in Europe to the polio epidemics of the fifties. The traditional iron lungs which encased the patient inside a tank, with a rubber seal at the neck and applied intermittent negative pressure ventilation were inefficient and capacity was soon overwhelmed. Intermittent positive pressure ventilation (IPPV) applied via an endotracheal tube during surgery was by then relatively common practice, but there was little experience of using such systems for prolonged periods. In the Copenhagen epidemic of 1952, tracheostomies were performed and patients were hand ventilated in shifts by medical students. Both in Europe and North America simple mechanical ‘ventilators’ to undertake the task of delivering IPPV were rapidly developed and the medical students released back to their studies.
Clinical outcomes in those who regained adequate neuromuscular function were found to be excellent and the concept of managing numbers of patients requiring this complex intervention in designated areas or ‘intensive care units’ (ICUs) evolved. Initially managing respiratory failure attributable to both extrinsic (eg neuromuscular) and intrinsic (eg pneumonia) causes, ICUs began to manage patients with multiorgan system failures involving cardiovascular, renal, metabolic, nutritional and neurological deficiencies.
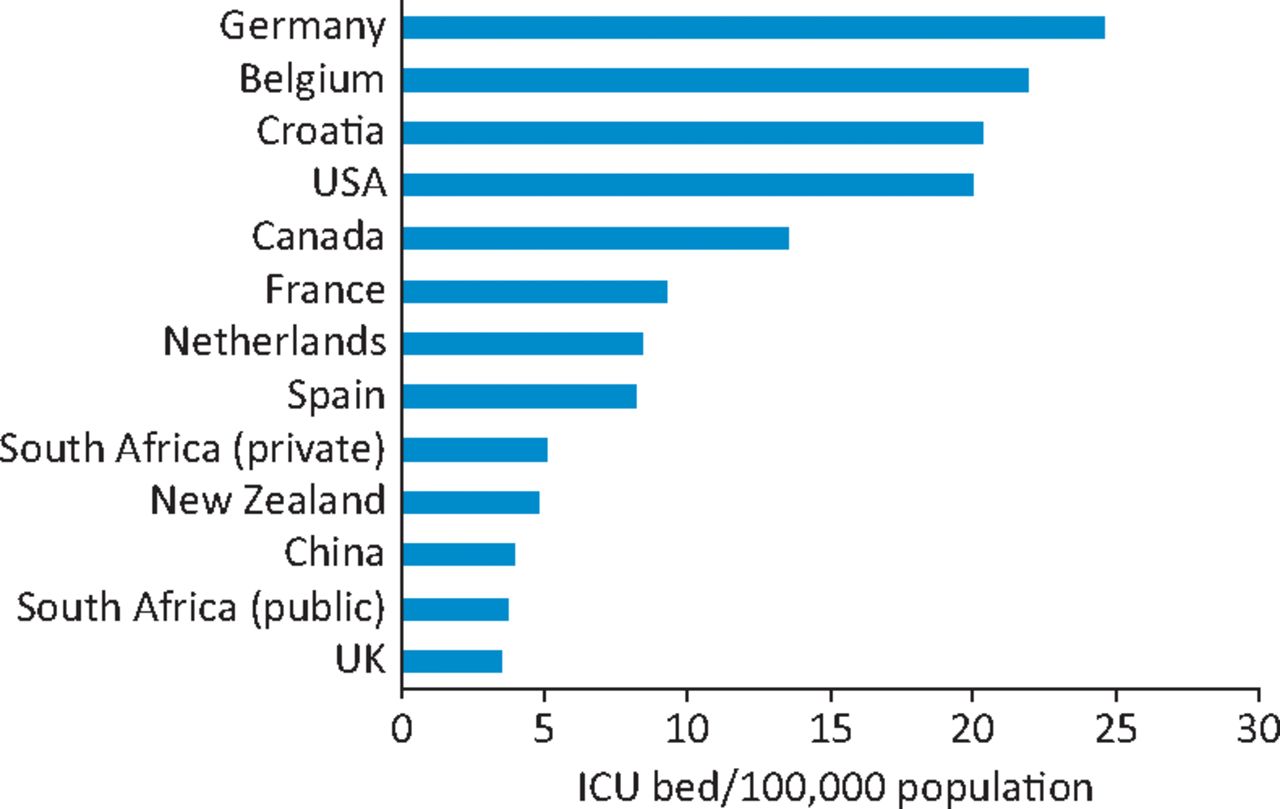
This historical legacy meant that until the last decade intensive care medicine (ICM) was practised almost exclusively by those with airway skills (anaesthetists), at least in the UK. Moreover, the dependence on technology and the desire to manage the whole patient led to ICM retreating metaphorically and literally behind locked doors. Admission was strictly regulated by those within, as was admittance. This is an expensive resource and undercapacity has always been an issue in the UK compared to other developed countries (Fig 1).
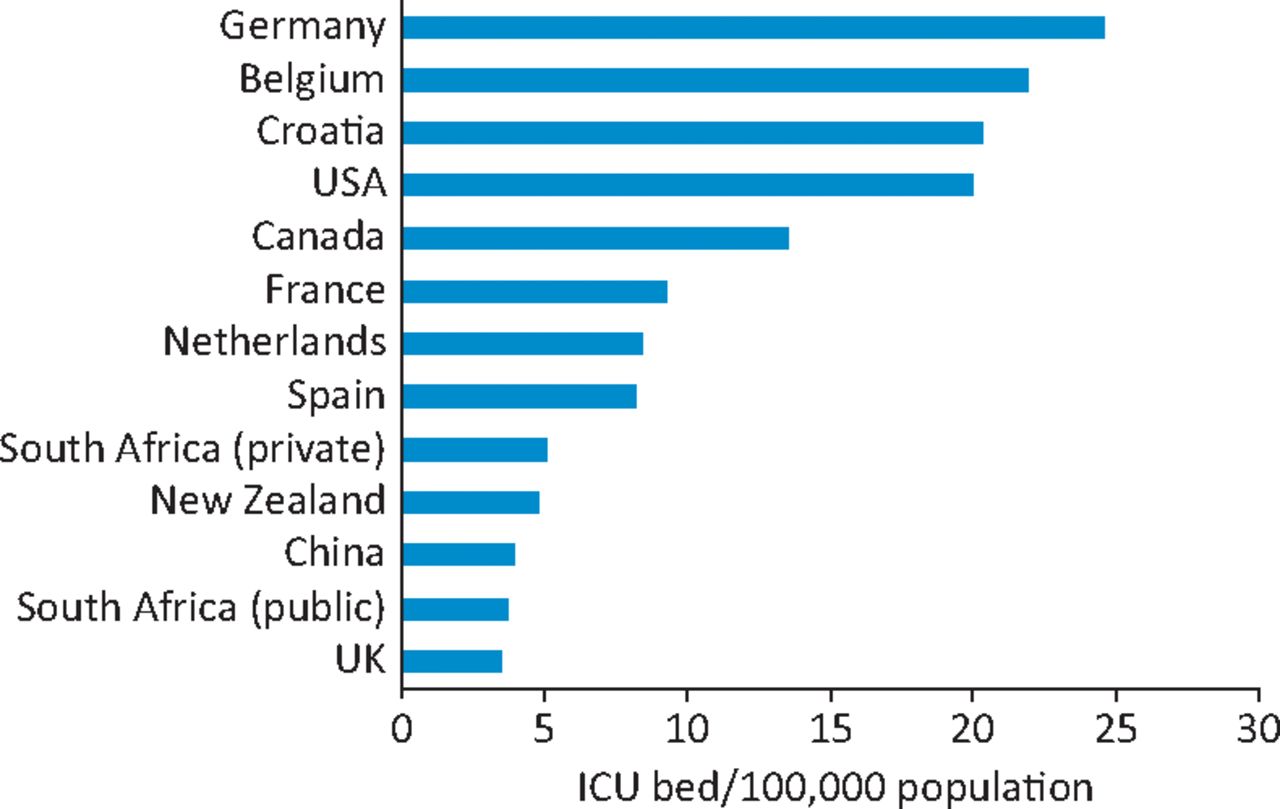
ICU beds/100,000 population from respective national data. Reproduced with permission.1
Much has changed over the last fifteen to twenty years. The Department of Health (DoH) report, Comprehensive critical care,2 published in 2000 was instrumental in describing ICM as a system not a place, and the introduction of outreach teams has accelerated a move towards lower levels of dependency and anticipation of deterioration as central planks of the clinical model.2,3 Indeed, the report described a service designed around patient needs across the whole hospital, proposing to replace the artificial divide between intensive care, high-dependency care and ward care with a patient-focused rather than location-focused service.2
These principles remain valid today although the aspirations are by no means fully realised. Critical care, as defined in the report by the DoH, is indeed delivered by many outside the formal units in respiratory, renal and cardiology wards, across the surgical floors and at the front door, although changing demographics and patient expectations are placing huge demands on its capabilities particularly in medicine.
So how can cooperation between medicine, particularly acute medicine, develop to best care for those in need?
Policy initiatives
The size and complexity of the challenges presented by our ageing and frail population with multiple chronic medical conditions is clear to the public, policy makers and the medical profession. Indeed the proponents of acute medicine recognised this more than 10 years ago and, through the formation and evolution of the Society for Acute Medicine who, with the support of a significant few within the Medical Royal Colleges, have developed and embedded a comprehensive training scheme and established dedicated acute medical units within most UK hospitals. However, in many places the relentless pressure of the work has meant the role of the medical registrar has become intolerable – torn between the ever-busy front door and the needs of an inpatient population cared for by cross-covering foundation year and core medical trainees.
A significant proportion of both these populations of patients are clinically unstable and may require some form of augmented care. Analysis of medical admissions, particularly looking at the Society for Acute Medicine's benchmarking audits, suggest approximately 10% of presenting patients have an national early warning score, or equivalent, of four or more.
A comprehensive inpatient audit performed in two hospitals in the east of England on two occasions, summer and winter, designed to assess ‘unmet need’, employed a multifaceted tool incorporating aspects of both physiological instability and nursing dependency. The results were consistent in both trusts on both occasions; about 10% of inpatients had unmet need and 2–3% fitted level-2 criteria (Table 1). The data thus confirmed a proportion of both acute presentations and inpatients are at increased risk, and many of these might benefit from some form of augmented care.
Levels of critical care as defined. Reproduced with permission.2
There is a clear need for early recognition and intervention at the point of admission in the 10% cohort discussed earlier. These patients have an inhospital mortality of about 4%.
The seven-day service debate is also relevant here. An analysis of acute hospital admissions by Fremantle et al4 reported a 16%, 30-day, increased mortality of those admitted to hospital Sundays compared to Wednesdays. The increased mortality was in emergency admissions and almost exclusively in a cohort of medical patients with diagnoses including carcinoma of the lung, myocardial infarction, congestive cardiac failure, acute renal failure, stroke and sepsis. There was no severity scoring of these patients and many may well have had a terminal illness. Patients actually in hospital at the weekend had a reduced risk.
The message emerging from studies such as these is clear. All acute medical units should have facilities to deliver augmented care (level 1). Larger units should have dedicated level-2 beds appropriately staffed and allowing invasive monitoring, simple inotropic support and non-invasive interventions such as continuous positive airway pressure or non-invasive ventilation. The basic principle here is one of early recognition and aggressive intervention. Many patients with new, reversible illness will stabilise and improve. Some, who either have or are developing organ failure, will require level-3 care. Close communication and cooperation between the acute physician and critical care physician is essential if this model is to work. A third group of patients are more difficult, and in many ways demand an even closer understanding between medical teams.
These are the patients who are sick, unstable or deteriorating but where critical care intervention is unlikely to be beneficial. This is a difficult area, as predicting outcome from critical care is difficult and there is almost no hard evidence to support decision making.
The future
Many authorities recognise the challenges to delivering effective healthcare. Political initiatives include the Five year forward view from NHS England,5 Shape of training from the General Medical Council6 and latterly Seven-day working,7 the ‘manifesto commitment’ of the current government. The Royal College of Physicians’ Future Hospital Commission recognised the relevance of interactions between emergency, acute and intensive care medicine when considering how interactions between different medical specialities might develop to the benefit of patients.8
Perioperative medicine might represent one model in which an integrated pathway from general practice, through admission and surgery to rehabilitation has been adopted for high-risk patients, and may provide a template on which to base similar initiatives for medical patients. This is a truly multidisciplinary programme and trusts are appointing perioperative physicians to support surgeons and anaesthetists in assessing, risk stratifying, optimising and caring for these patients. This need not be an isolated role and much of the inpatient work of the hard-pressed medical registrars is in dealing with the fallout in these very patients. The potential role of the acute physician in the management of perioperative patients is discussed elsewhere in this issue of the journal.
The ‘generalist’ agenda advocated by Shape of training is similarly important. Acute care common stem (ACCS) core training has been in place for some years and has ensured physicians can train in basic anaesthesia and intensive care and vice versa. The principles underpinning this are supported by the three Royal Colleges involved: Royal College of Anaesthetists, Royal College of Physicians, Royal College of Emergency Medicine. It is likely that it will become the sole route of entry into speciality training in anaesthesia. Formal critical care training includes significant time in medicine, and acute, renal and respiratory medicine may all dual train with critical care. This close collaboration is the foundation for service cooperation and increased awareness of the unstable and at risk patient. It makes sense for all of those following an acute medicine training pathway to undertake an ACCS-type programme. Indeed this could be advocated for other medical specialities with a significant cohort of patients presenting acutely unwell.
An increasing number of clinicians hold dual accreditation and some have consultant posts with sessions in both critical care and acute medicine. Many more, however, have been unable to obtain this sort of post. This is an inevitable consequence of the way critical care is delivered in the UK. The vast majority of units are relatively small and traditionally staffed by anaesthetically trained intensivists. A critical care on-call commitment is essential to the stability of these units but the real shortage is of those with an on-call commitment to the front door. The sharing of posts in both areas is one possible solution. Importantly though, this trained workforce is ideally suited to support the delivery of the principles within comprehensive critical care.
There is an increasing tendency to admit and treat. Active management, involving multiorgan support may be prolonged and ultimately futile. This imposes a significant burden on patient, families, careers and the economy. Even in those who survive, quality-of-life will be incrementally reduced and many will die within a few weeks of discharge. Critical care cannot reverse the progression of chronic disease and frailty is a reliable predictor of poor outcome. A period of augmented care at admission allows time to assess these patients, obtain detailed social histories and evaluate their response to simple interventions. Informed discussions about realistic treatment options with the patient and their families are possible. In some, perhaps many, a decision to withdraw care or continue, but with limits will be agreed. These discussions should include the critical care and acute physician.
Conclusions
In summary, there are many areas of integration and cooperation with critical care and medicine. These start with overlapping training, recognising the many shared competencies, and there are an increasing number with shared consultant roles. If we are to better meet the demands of the cohort of inpatients with unmet needs and those presenting acutely unwell, we need to accept that recognition and intervention is required throughout the day and week. The acute care hub, in a physical sense, may be unrealistic in many settings, but the principles are universally applicable. The ability of the medical team to deliver effective augmented care at the point of admission is more important than the physical space. The acute physician with critical care skills will have an essential role directing this care in the future hospital.
- © Royal College of Physicians 2016. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.