
ABSTRACT
The Five Year Forward View describes ‘closing the care and quality gap’ as one of three strategic challenges facing the English NHS by 2020. The need for a coherent national strategy for achieving high-quality, affordable care has rarely been more pressing, but how effectively do existing national decisions and interventions support clinicians delivering care on the front line? And, in a complex and dynamic environment with multiple players, how should the health service move forward to develop a balanced strategy for quality that accommodates longer term goals as well as more immediate political priorities? Research by a team at the Health Foundation has assessed how the array of organisations, initiatives and approaches to quality stack up as an emergent strategy. Four concepts were used to provide a yardstick for quality-related policies and activities to help identify potential imbalances, gaps and duplication. The findings of this work, together with suggested steps to rectify the issues identified, are described here.
Introduction
Most OECD (Organisation for Economic Co-operation and Development) countries aspire to offer their populations high-quality and affordable healthcare. The starting point is to ensure access of the whole population to comprehensive healthcare, with financing mechanisms to support that. But the next is to work towards achieving high-quality care – quality in a number of domains including safety, effectiveness, timeliness, patient-centeredness, efficiency and equitable access.1 Achieving this needs a coherent and constantly developing strategy because of the many factors influencing quality of care, the long lead time needed to develop some of them and their complex interaction.
At varying points in the history of the NHS there have been attempts at producing some kind of overall strategy; in England, most recently in High quality care for all – the final report of the Next Stage Review led by Lord Darzi, published in 2008.2 Scotland, Wales and Northern Ireland have all since published explicit national strategies to improve quality in their respective national health services.3–5
In England, the strategy set out in High quality care for all has never been formally replaced, but since 2008 there have been significant changes to all levels of the NHS. Widespread reform to organisational structures and roles followed the Health and Social Care Act 2012 (the 2012 Act).6–8 Annual funding growth for the NHS in England has never been lower – projected to be 0.9% average real terms per annum between 2010 and 2020, against the long-term average of 3.7% – with an even more challenging settlement for social care.9 Well publicised scandalous lapses in care and subsequent inquiries have prompted a significant focus in national policy on improving patient safety since 2013.10–18
The resultant picture is of dynamic and complex development with multiple players. Given this, a key question is how best to move forward? How to develop a balanced strategy that develops short, medium and longer term goals, and can accommodate immediate political priorities? This paper tries to give some answers, based on research (focusing on England) published earlier this year by a team at the Health Foundation.19
Concepts
A starting point is to assess the array of organisations, initiatives and approaches to improve quality in the NHS. How do these stack up as an emergent strategy? To help, we identified four concepts, frameworks and taxonomies that could categorise a large number of different initiatives and approaches, and identify potential imbalances, gaps and duplication.
The Juran trilogy
The first concept is the Juran trilogy (Fig 1), which posits the individual and collective importance of three core functions in achieving high quality in any industry: planning, control and improvement.20

The Juran trilogy.
Juran framed these concepts as internal planning control and improvement processes within individual organisations. In the context of the NHS, the Juran trilogy is helpful to frame the processes needed at national level, external to individual provider organisations: the need for robust national planning to set direction, the provision of meaningful support (‘improvement’) to the professionals and organisations delivering care and the appropriate use of control mechanisms to ensure risks are minimised and progress is made. Furthermore, Juran stressed the inter-relatedness of these functions and the importance of achieving an appropriate balance between them to develop an effective approach to improving quality. How these functions are currently discharged within the NHS, and the extent to which there is an appropriate balance between them, was a fundamental part of our analysis.
The NHS Quality Framework
The second concept is a modified version of the NHS Quality Framework: a seven-step model for achieving high-quality care for all, outlined in High quality care for all, which appears to remain the current strategic national framework for quality (Box 1).21
Modified NHS Quality Framework.
Health system tiers
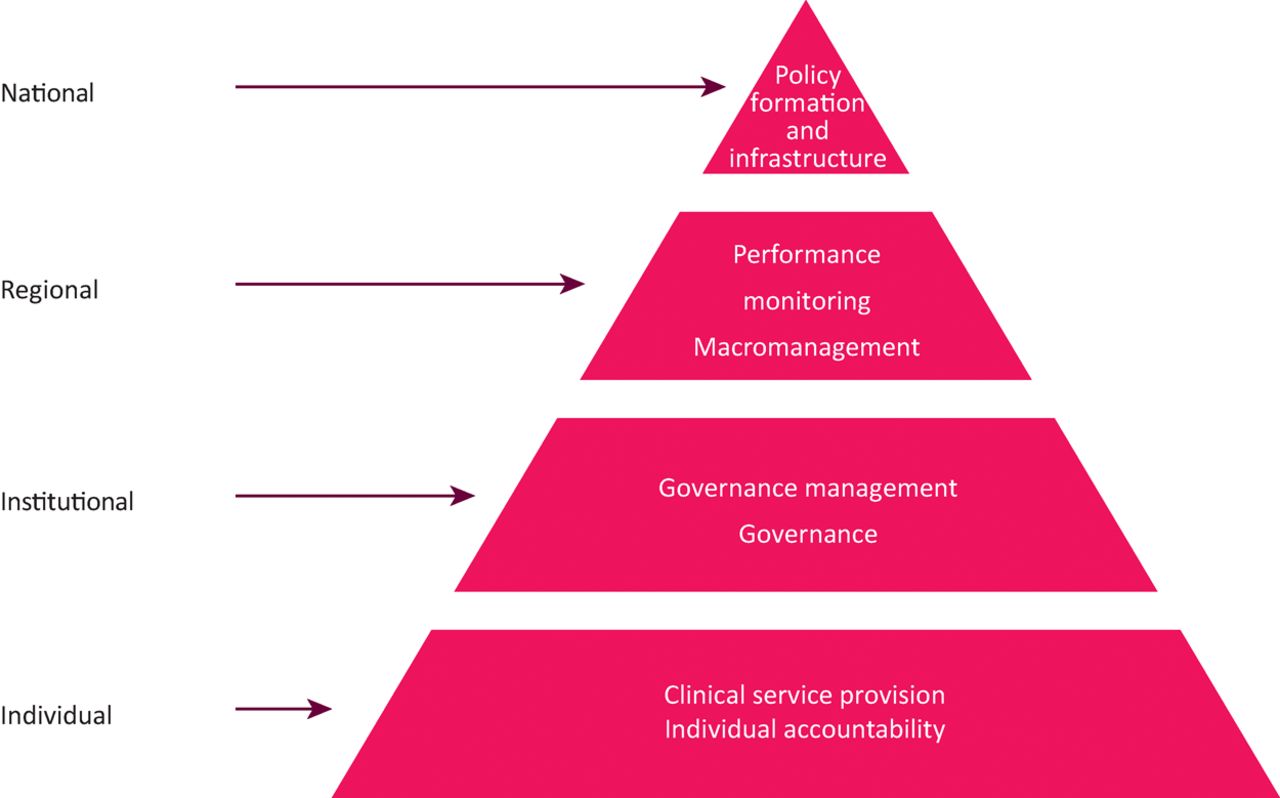
The third concept is that of creating multi-tiered capacity in a nation and is depicted by a pyramid with four levels, allowing for the design of discrete and synergistic activities and interventions at various geopolitical and administrative levels. The four levels (Fig 2) where activity needs to occur is applicable in almost any country and has been described as:22
national – essential functions are policy formulation, resourcing, infrastructure and accountability to the public
regional/local – essential functions include translating national policy into the local context, macro-management and monitoring
institutional – essential functions include good governance, competent operational management and continuous quality improvement
individual – this is the level of encounter between patients and health professionals where the key attributes of quality must be actualised through individual behaviours.
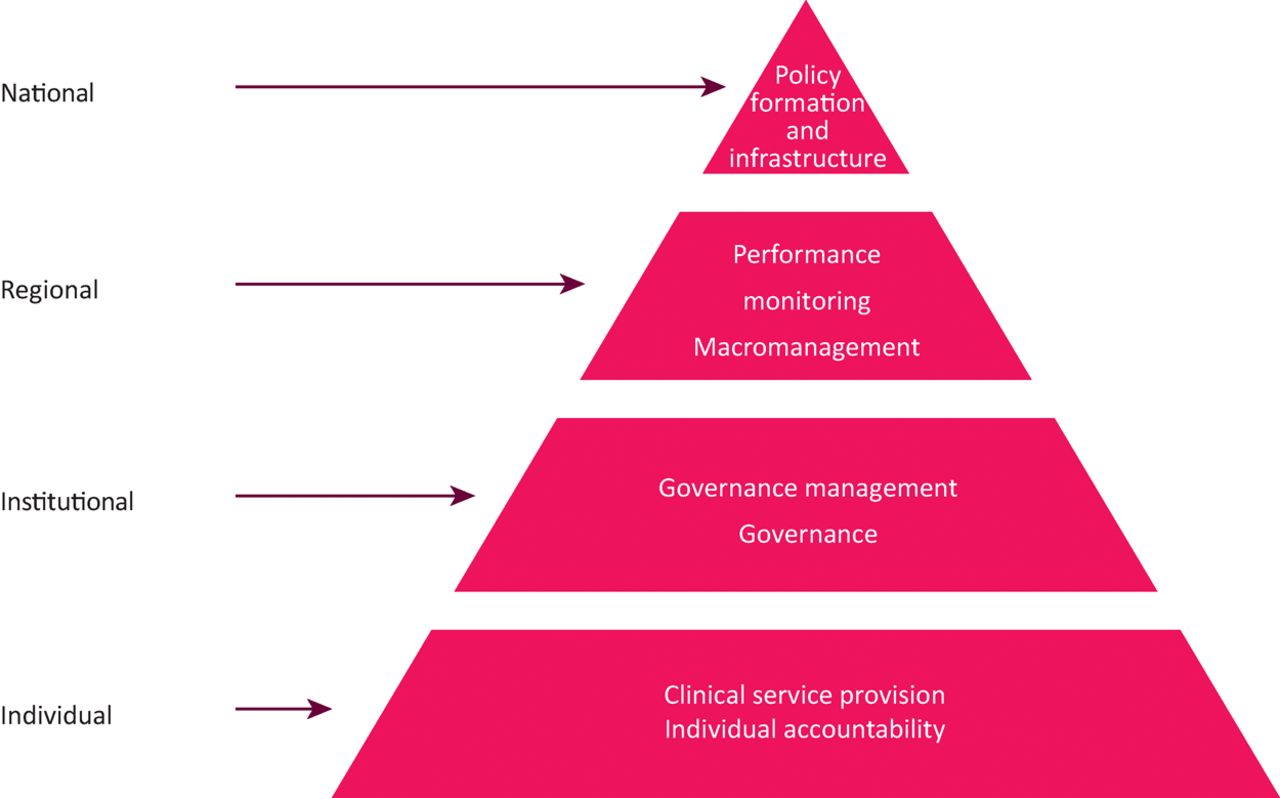
Multi-level model for building capacity for a national quality strategy.
Domains of healthcare quality
The fourth and final yardstick is to match up quality-related policies and activities against the domain(s) of quality for which they were intended to improve. Our report used the Institute of Medicine's definition of six domains of quality: safe, effective, patient-centred, timely, efficient and equitable.1
We used these frameworks to structure the analyses described.
Analysis
Three analyses are reported here; the first was of the government's broad approach to quality through its response to recent independent reports. The second of the self-described roles and responsibilities of the Department of Health, the main arm's-length bodies (ALBs)23 and selected other national organisations – as they now exist to support quality. The third was a qualitative set of discussions with over 100 senior leaders – from the Department of Health, ALBs, healthcare providers and commissioners, clinical leaders, patient groups and independent organisations. This aimed to construct an experiential-based perspective of the current approach to quality in the NHS in England. A further analysis, of the evidence of impact of some key initiatives, can be found in our original report.19
The government's broad approach to quality
Since 2010, the government has undertaken an evolving programme of NHS reforms. Some arose from the 2012 Act, others following recommendations of independent inquiries of well publicised scandals in care, such as Sir Robert Francis’ second inquiry into Mid Staffordshire Hospital NHS Foundation Trust. In response to the inquiries, the government commissioned a number of further independent reviews into a range of issues, which produced further recommendations.
In total, nine independent reports were identified, with the government's formal response published in four policy documents as listed in Table 1.
The number of initiatives resulting from the government responses to independent reports
Each initiative was analysed using several of the concepts outlined earlier, and the following themes identified.
The sheer volume of the government response to the crises of care in NHS trusts was obvious. In total, 179 new initiatives were announced by the government from June 2011 to December 2015 in just the four government responses chosen for this analysis. In the period following publication of the Francis Inquiry in February 2013, there were 143 initiatives – more than one per week over 2.5 years.
There were asymmetries in the focus of these initiatives: far more focused on regulation than support for improvement, and there was a stronger focus on improving safety relative to other domains of quality.
There was unclear accountability for implementation and assessment of impact: initiatives have been implemented at various timescales, in some instances without obvious accountability, follow-up or evaluation. Many initiatives are still in the planning stage, highlighting the time lag between policy announcement and the system response. Information on progress (or a clear decision to abolish the initiative) was often very difficult to find.
There was an over-focus on initiatives that are not well supported by evidence of effectiveness, such as changing organisational culture to improve quality. It could be that the evidence base in many areas is very weak, and ‘common sense’ prevailed, but a well-argued basis for initiatives was often absent.
Roles and responsibilities of the Department of Health, the main arms-length bodies
The main roles of national organisations were identified from their published mission statement and mapped onto a framework based on the seven steps for quality identified in High quality for all (Box 1).2 The Department of Health, Care Quality Commission (CQC), Health Education England (HEE), the National Institute for Health and Care Excellence (NICE), NHS England and NHS Improvement were all included in this analysis. Acknowledging that the organisations are more complex in practice, the mapping broadly showed the following.
All of the national bodies covered by this analysis play some sort of role in relation to the quality of NHS care. None of these bodies has explicit responsibility to lead work on quality at national level, nor does any single body appear to have a de facto leadership role in this respect.
The various roles and responsibilities undertaken by the national bodies often cut across the three core functions in the Juran trilogy of planning, improvement and control. Given the inter-related nature of the three core functions and the distributed national leadership of the health service, there is a premium on having effective mechanisms to share information, undertake joint planning and align actions.
Multiple bodies are involved in setting national priorities and standards for the different types of local institution in the NHS. The accountability of local institutions for quality is cluttered. An NHS foundation trust, for example, can expect to be held accountable for quality of care by clinical commissioning groups and NHS England as the local and national commissioners, the CQC as the national quality regulator and NHS Improvement24 as the independent regulator of foundation trusts.
There appear to be few national bodies heavily involved in building the skills of staff to provide high-quality care and improve the quality of services. This role has arguably been left to be fulfilled by local leaders, with consequent variation in capability across England.
There has also been a historic lack of support for improvement in primary care. CQC regulates primary care but NHS Improvement only aims to provide improvement support for secondary care. This is a gap that may be filled by the new programme of improvement support announced in the recent General Practice Forward View, but this will inevitably take time to become fully embedded.
Interviews of over 100 senior leaders
In total, we spoke to around a hundred people working at various levels within England, mainly through individual interviews and group meetings; of these 43 were senior leaders – three-quarters from the Department of Health or the main ALBs.
The most striking result of this survey analysis was the unity of the message. The vast majority – at a wide variety of levels and across a variety of organisations – agreed on the themes outlined below. While this could be due to an element of ‘group-think’, it also indicates a shared perceived need to develop a more coherent strategy.
There was a perceived imbalance between planning, control, and improvement. On planning, people highlighted the absence of a strategic approach to planning to support the NHS Five Year Forward View,25 which was thought to provide a shared vision but not a clear framework for implementation. This was attributed to the lack of a national centre within the reformed system and perceived poor alignment between the national bodies, which has also led to a proliferation of top-down requests for assurance and a surfeit of national priorities.
Most people suggested that, at national level, control had now become the primary driver of choice to improve quality of care. There were mixed views as to whether control has been become over-developed, but there was broad agreement that planning and improvement functions were under-developed. The establishment of NHS Improvement was broadly welcomed to support improvement within the NHS, but there were concerns that the new organisation has a very challenging set of immediate objectives.
The commitment to improving quality as the organising principle of the NHS was thought to be weak. Most people had concerns that the national tier of the system is now fragmented and the coherency of policy and policymaking has diminished. The 2010–15 parliament – including the reform and organisational restructuring that flowed from Equity and excellence: liberating the NHS in 2010,26 as well as the need to respond to several high-profile failures of care – was recognised as a turbulent period for the NHS. With national bodies taking on new roles, developing different ways of working and managing a major transition programme were widely thought to have led to greater divergence in the approaches taken by national bodies as well as increased duplication of effort.
Most people suggested that, in the wake of the Francis Inquiry, there has been a necessary focus on improving safety, but several wanted to see a broader focus on all aspects of quality.
People were mostly clear that health professionals have the ability to use skill and judgment to make clinical excellence thrive everywhere, but this is sometimes crowded out by a lack of national support for workforce engagement, training of clinical leadership and a focus on immediate pressures rather than designing and implementing improvements.
Discussion
The headlines of our analysis of the national approach to improving quality as outlined above show some clear messages: an impressive amount of activity to improve quality, but a lack of a clear coherent strategy evidenced by the range of uncoordinated initiatives; unclear guiding leadership of the agenda; an imbalance of recent initiatives towards ‘control’ over ‘planning’ and support for ‘improvement’ and towards safety over other quality domains; unclear follow-up and implementation; and, as described more fully elsewhere,19 actions not well informed by analysis of impact. Clinicians may well be bewildered by this complex array of organisations, requirements and initiatives with accompanying jargon.
At national level, the organisational changes set in motion by the 2012 Act has resulted in a group of statutory bodies – NHS England, NHS Improvement, CQC, HEE, Public Health England and NICE, the so-called ‘system stewards’ – operating at arm's-length from the Department of Health.
On the one hand, this more distributed leadership risks lack of coordination. But on the other, it offers an opportunity for a body of expertise to develop at arm's-length from political priorities of the day to develop and protect a coherent short, medium and longer term agenda for progress on quality. These arrangements must offer legitimate space for the government of the day to influence the NHS according to its own priorities, but not allow the NHS to be led by short-term political concerns, reactive to events at the expense of a medium to longer term strategy for progress.
An example of movement in this direction is the NHS Five Year Forward View,25 where system stewards have united behind shared vision. Clearly our analysis suggests there is some way to go, yet it is important to note that many of the ALBs are relatively new and organisational development within and across them takes time. There are important issues also here about the development of the role of the Secretary of State27 and the Department of Health, but space here precludes a foray into this interesting arena.
The other standout message from our analysis is, considering recent national initiatives, the imbalance of approach towards ‘control’ over support for ‘improvement’ and ‘planning’. Hard pressed clinicians will recognise the pressure to ‘work harder’, rather than being afforded the headspace and support to design and implement what might be more efficient practices. This imbalance has been recognised in recent years28,29 and there are small signs of progress.30–34 As Steven Spear, a senior lecturer at the MIT Sloan School of Management, wrote recently, high-quality care and great performance involve leaders making problem solving, improvement and innovation part of the regular routine of daily practice.35
So what might next steps be? Our analysis points to the need to:
articulate a single set of quality goals and common definition of quality
The ‘system stewards’ should publish a consolidated and balanced set of quality priorities with explicit, measureable goals for improvement. The national bodies should agree a definition of quality to provide a shared conceptual framework and a common language for quality.
provide unified national leadership for quality
The ‘system stewards’ currently meet in a Five Year Forward View Board, which provides a unified focus for action across the national bodies at the highest level. For pragmatic reasons, we suggest it should become the main national committee for making decisions about quality, supported in this role by advice from the National Quality Board,36 acting as the conscience and the intelligence of the system on quality. The role of the Department of Health here would need to be clarified and agreed, and how short-term legitimate government priorities can be addressed appropriately within a wider and medium-term strategy.
build on experience and evidence
Research on the impact of policy on quality provides few definitive answers, but sensitive use of the available evidence can guide policymakers towards a number of ‘best bets’ more likely to have a meaningful impact and more prudently employ limited resources.
update a set of core quality metrics
Based on advice from the National Quality Board, the Five Year Forward View Board should co-produce a unified set of core quality measures for the NHS to be used as the basis of performance measurement by all national bodies.
articulate a shared understanding of how improvements in quality and costs are linked and pursue both in tandem
The ALBs also need to develop a more sophisticated and granular view of the relationship between quality and resources. Being explicit where investment and disinvestment may occur, with what intended effects and risk mitigation, would provide a transparent basis for addressing quality within a seriously resource-constrained NHS.
provide unified regional leadership for quality
The Five Year Forward View Board should also consider taking further steps to bring together their various regional and local presences to share information, develop joint working arrangements and streamline requests for information from commissioners and providers. This already happens to some extent, for example through quality surveillance groups, but there is clear potential for achieving much greater alignment.
Conflicts of interest
The authors have no conflicts of interests to declare.
- © Royal College of Physicians 2016. All rights reserved.








{kind=link}
{kind=link}