
ABSTRACT
Healthcare systems worldwide face the challenge of recognising and improving safety, timeliness, quality and productivity. The authors describe how the COM-B model, developed by Michie et al in 2011 to explain and change criminal behaviour, is useful in identifying what skills and capabilities healthcare providers require to improve their systems. These skills include the intellectual capability to understand, design and improve healthcare processes; the opportunity to do this in their daily work; the motivation to do this – in particular recognising the reasons not to change; and finally unlearning the behaviours based on historical system beliefs that are now invalid. Individual self-awareness and organisational leadership are required to give staff the time and resources to reflect, experiment and learn.
Introduction
Quality improvement is the designing and redesigning of work processes and systems to deliver healthcare with better outcomes and lower cost.1
Professor Don Berwick began his keynote speech at the 2016 International Forum of Quality and Safety in Healthcare with a simple question: ‘Would you trust a surgeon who didn't know anatomy? By extension, therefore, would you expect someone to re-arrange a healthcare system without some knowledge of how the healthcare system works’?2 We contend that poorly informed system tampering produces potentially negative consequences in those systems.3 The resulting disruption can endanger patient safety, staff engagement and the wellbeing of both patients and staff. Healthcare services will never realise their full potential until improvement becomes part of every worker's day job rather than a temporary phenomenon.4 For this paradigm shift to occur, we will need to learn and, more importantly, unlearn behaviours.5
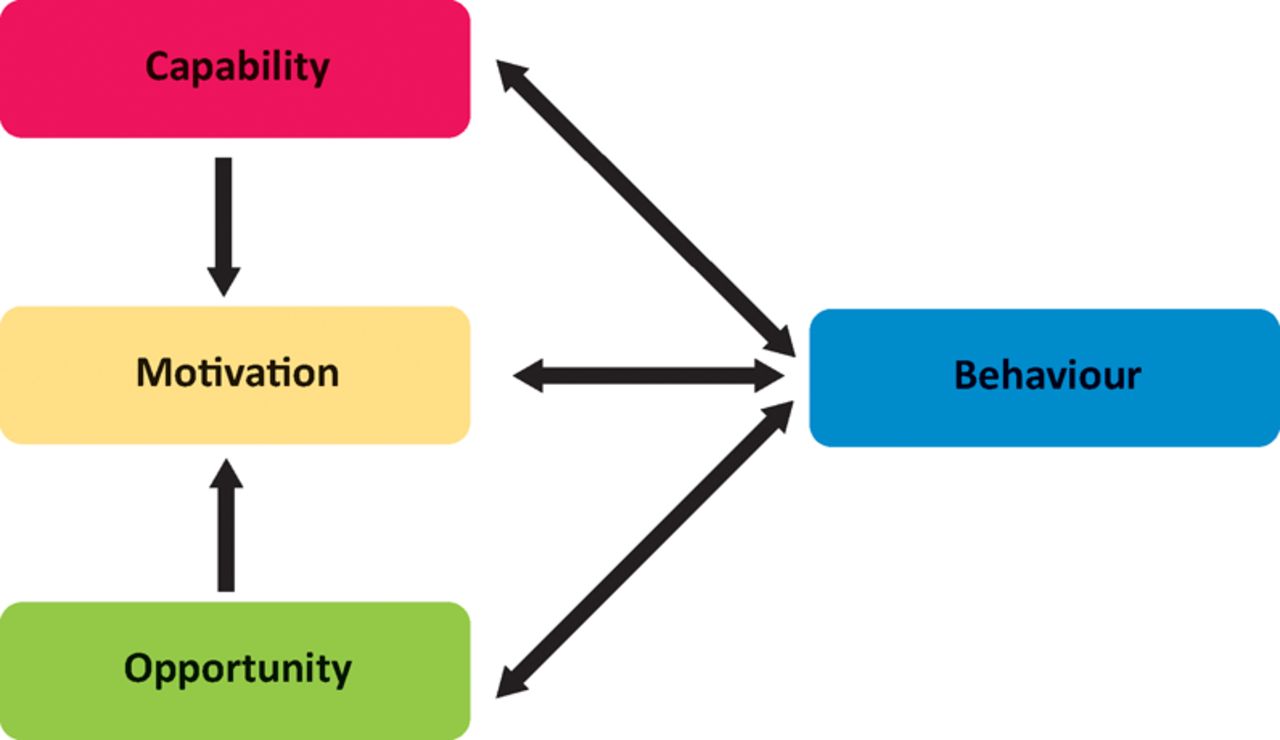
Although ‘every system is perfectly designed to get the results it gets’ (attributed to Dr Paul Batalden, the Dartmouth Institute, USA), we do not believe that this state is a result of deliberate intent. All improvement requires change yet not all changes are an improvement and the challenge faced in managing change is neatly framed by the COM-B (capability, opportunity, motivation and behaviour) model (Fig 1).6 We will use this model to describe the three issues that need to be addressed by healthcare professionals, including clinicians and managers, to achieve successful improvement behaviours.

The COM-B model. Reproduced with permission from Michie et al.6
In this ‘behaviour system’, capability, opportunity and motivation interact to generate behaviour that in turn influences these components. Capability is defined as the individual's psychological and physical capacity to engage in the activity concerned; it includes having the necessary knowledge and skills. Motivation is defined as all those cognitive processes that energise and direct behaviour, not just goals and conscious decision making. Motivation includes habitual processes, emotional responding, as well as analytical decision making. Opportunity is defined as all of the factors that lie outside the individual that make the behaviour possible, such as the availability of resources (especially time). The single-headed and double-headed arrows in Fig 1 represent potential influence between components in the system. This model can be encapsulated by the questions ‘can't?’ or ‘won't?’ that are the barriers to change in behaviour.
Capability (can't)
There are two aspects to capability: firstly, the underlying cognitive potential of the individual to learn and apply system design and improvement science to their daily work. Current research has repeatedly shown that the most successful and long-lived adaptable organisations are led by engineers or those with a scientific background.7 The explanation given is their rational (data-based) problem analysis and ability to design, study and learn from the results of their incremental, real life expensive business experiments.
The second aspect is the availability of the training in system design and improvement science. Physicians are trained to expert level in their area of specialist subject matter knowledge. However, the training in skills to design and improve the system that delivers care is limited – it was more than a decade after starting clinical training that the authors of this paper started to gain system design and improvement science skills. Many clinicians and managers resort to expensive and time consuming MBAs that do not provide them with all the skills they seek.8 As a consequence, many organisations – including those in healthcare – resort to in-house programmes that are often designed by those with rudimentary improvement science skills. This leaves the individuals with inadequate skills to address the gap between the safety, financial rhetoric and the reality faced by many service industries. These quality improvement agendas are underpinned by knowledge from widely available lean, six-sigma and theory of constraints courses, many of which have been adapted for healthcare. However, they often miss one key component: system design. Multiple ‘single point improvements’ will not be sufficient to address the huge gap in safety, quality and finances faced by many complex industries – most particularly healthcare. Fortunately, we are now in the information age in which the ability to pass the new and different memes that make a difference no longer depends on a hierarchical ‘church’ policing the established beliefs. Don Berwick describes the emotional impact and almost ‘religious’ experience when we recognise the significance of system design and improvement science as the missing pieces of the knowledge jigsaw we have been searching for.
Motivation (won't)
So what motivates healthcare practitioners? It is widely accepted that those in healthcare are motivated by a strong sense of duty and professionalism, as well as scientific curiosity and empathy for our fellow human. Positive motivation to improve our healthcare system should not be an issue. The motivational will to change is most effective when there is both ‘push’ and ‘pull’. Are our current improvement paradigms a barrier? Does our need to learn a new improvement skillset create a fear of the consequences of addressing our lack of capability?9 This manifests itself in potential loss of face when we have to admit that we don't know what we are doing. This can lead to challenging behaviours. Recognising and addressing this is a key skill we have to learn to recognise and address, initially in ourselves. This emotional component creates the ‘push’ – the discomfort with the status quo. If we can create a belief, through clear evidence that ‘better’ can and has been done, then this generates the reciprocal ‘pull’ dimension.
Opportunity
The third element in this behaviour system is opportunity. There are a number of component parts to this, starting with leadership. Leadership enablement is needed to release staff – individually or in teams – to initially participate in learning quality improvement skills and then to have the space to deliver and reflect. Secondly, there is a need to provide structured learning so that it includes both technical and coaching skills because in healthcare successful improvement is 80% human and only 20% technical.10 Lastly, there is organisational culture that requires changes to be delivered using a scientific model rather than the belief that improvement is merely a result of ‘just doing something’.
Opportunities exist at three levels:
Front line work at the interface with the patient. This is where the expert subject matter knowledge lies in how to deliver the value that the patient seeks.
Management work:
Understanding the constraints that need to be addressed and the gap between the system's aims and current results. Constraints reveal themselves as errors and rework or queues and delays. They are rarely due to a shortage of resources and are more commonly due to policies, eg scheduling, prioritising or batching.
Focusing their attention on improving outcomes and productivity through that constraint, even if it is not in their department or organisation. This means working collaboratively, not competitively.
Coordinating the experts at the coalface who have the inherent and detailed understanding of how the constraint works and enabling them to test and learn new ways of working.
Measuring the current and required performance and creating real time feedback upwards and downwards.
Recognising when there has been a statistically significant change to process performance, or not.
Executive work:
Understanding and articulating (in words and numbers) the purpose of their healthcare system.
Understanding the anatomy (organisation and physical structures), physiology (flow – including the invisible and challenging system dynamics) and pathology (constraints) in the current system that prevents it from delivering that purpose.
Focusing the management attention on the 20% of the constraints that account for 80% of the resources that are unable to deliver the purpose and are therefore wasted.
Coaching the next generation to design and then continuously improve the system to meet the current and future objectives in a constantly changing world.
Rationally monitor the impact of the system in real time against the purpose and remove all blame for a disappointing, and therefore revealing, result. To quote Don Berwick ‘treasure every defect’ – each disappointing result is an opportunity to further explore, understand and improve the system.
There are opportunities at all levels to design and improve the way the work is done. The majority of quality improvement programmes focus on the front line workers and ignore the greater impact at management and executive level. The executives and managers of those organisations in which system design and improvement science is endemic are staffed at senior level by individuals who understand the executive and management processes. They honed their process design and improvement skills at the coalface and were taught by and learned the management and executive skills from the previous generation. So the more senior an individual is in their organisational hierarchy, the greater their skillset and experience of leading and facilitating improvement. Organisational stability is essential for this learning.11 So how do we start this virtuous learning environment in healthcare?
Changing mindsets is an emotional experience. In both clinical and managerial work we learn ‘what works’ and we continue to deploy our preferred method.12 This freezing of working method leads us to feeling stressed if our mental model fails to work. This is characterised by an increase in effort (often seen as being exhorted to work harder). At some point we recognise that our mental model is no longer fit for purpose and we go through the challenge of unfreezing and the emotional roller coaster of learning a new way of working. Most senior leaders (clinical and managerial) were trained before improvement science became recognised in healthcare, which is why we struggle to recognise its validity both in everyday life and in academic publication.
There is, therefore, a need to embed an early training of this science in all pre and postgraduate training. The 2016 Academy of Medical Royal Colleges’ report recommends that there should be a progressive curriculum in quality improvement activity underpinning all training stages of a doctor, building capability and leadership, and a foundation for ongoing lifelong learning and implementation.13 We don't have to depend on a top-down delivery of this training anymore; it can be achieved via wider distribution models, ideally combined with in-house training:
One-to-one professional networks starting social movements, eg the RCP's Learning to Make a Difference programme (www.rcplondon.ac.uk/guidelines-policy/ltmd-quality-improvement)
Interdisciplinary learning across hierarchical boundaries, eg the Institute for Healthcare Improvement's Open School (www.ihi.org/education/ihiopenschool/Pages/default.aspx) and The Health Foundation's Q initiative (www.health.org.uk/programmes/about-q-initiative).
Conclusion
The COM-B model, ironically developed to explain and address criminal behaviour, provides a simple and useful model by which healthcare professionals can address their individual and organisational limitations to achieve the vision of continuous improvement. The missing component is courage to recognise and address the gap between our rhetoric and reality.
Conflicts of interests
The authors have no conflicts of interests.
- © Royal College of Physicians 2016. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.