
ABSTRACT
Both hospital-based care and physician training have undergone significant changes within the past decade. Current physician training in the UK is failing to meet the needs of patients, with significant numbers of acute and general medicine posts unfilled. Building on the themes of the 2013 Shape of Training review, we propose a model that places an alternative model of generalist – the ‘future hospitalist’ – at the centre of patient care and medical training. The reinstatement of the general physician at the heart of hospital care will increase flexibility in both training and workforce planning, and embed active leadership, patient safety and quality improvement in care delivery.
Introduction
The landscape of UK hospital-based care and service organisation is undergoing unprecedented and accelerated change. With acute hospital care widely perceived to be in crisis in terms of finance, service provision and workforce morale,1 concerns regarding junior doctor recruitment, training and retention have entered the public sphere. Although beyond the scope of this article, it is impossible not to acknowledge the current financial and political context, following Britain's decision to leave the European Union, year-on-year NHS budget deficits and the first strikes by doctors in England in 40 years. Details aside, a concatenation of external circumstances and internal NHS pressures have led to one of the most widespread and pressing debates regarding the shape of medical training within the last two decades. The current climate has highlighted the perceived tension between training needs and service provision, which are frequently cited as placing an unmanageable burden on both training programmes and individual trainees to achieve necessary educational goals and clinical experience.2
Additionally, and rightly, patient demands regarding quality of care are higher than ever before. Following devastating failings of care at the Mid Staffordshire NHS Foundation Trust over the last decade, the Francis Inquiry highlighted the need for changes in not only practice, but also the current culture within the NHS. It also called for greater openness and transparency between healthcare providers and patients.3 In the wake of the inquiry and the subsequent Keogh mortality review,4 there is understandable public anxiety over the quality of care provided by trainees rather than by ‘fully qualified’ consultants, a theme that has permeated media discussion of the recent industrial action by junior doctors. However, medical mistakes are increasingly identified as errors of omission or communication, rather than errors of training or knowledge,5 with improved communication shown to decrease errors by nearly one-third.6 The increased awareness and measurement of safety outcomes has resulted in algorithms and checklists becoming an integral part of modern medical practice;7 however, there is some resistance among more traditionally educated doctors.
So how should physicians be trained? In 2016 Britain, against a background of continuously revolving and devolving local and national services, doctors’ needs are inextricably linked to those of their patients. This is perhaps most evident in general and acute medicine, with trainees reporting increased pressure of workload associated with decreased public trust and increased patient volume, complexity and expectation.8 The lack of ‘give’ in a system developed to cater both to patient and training needs results in a tenuous, and at times precarious, balance between these needs and those of the service as a whole. Consequently, we risk cycling between levels of healthcare provision and sustainability as resources flow and ebb in response to care and training crises (Fig 1). As stated in the Royal College of Physicians’ (RCP) Future Hospital Commission (FHC) report,9 we need a radically different approach to medical training to better absorb and anticipate change proactively, and to foster much-needed innovation. The 2013 Shape of Training review goes some way towards identifying key themes affecting training although the timetable for implementation is unclear.2 Building on these, and the four cornerstone ‘duties of a doctor’ defined by the UK General Medical Council (GMC),10 we suggest a model for training physicians of the future, or the ‘future physician'.
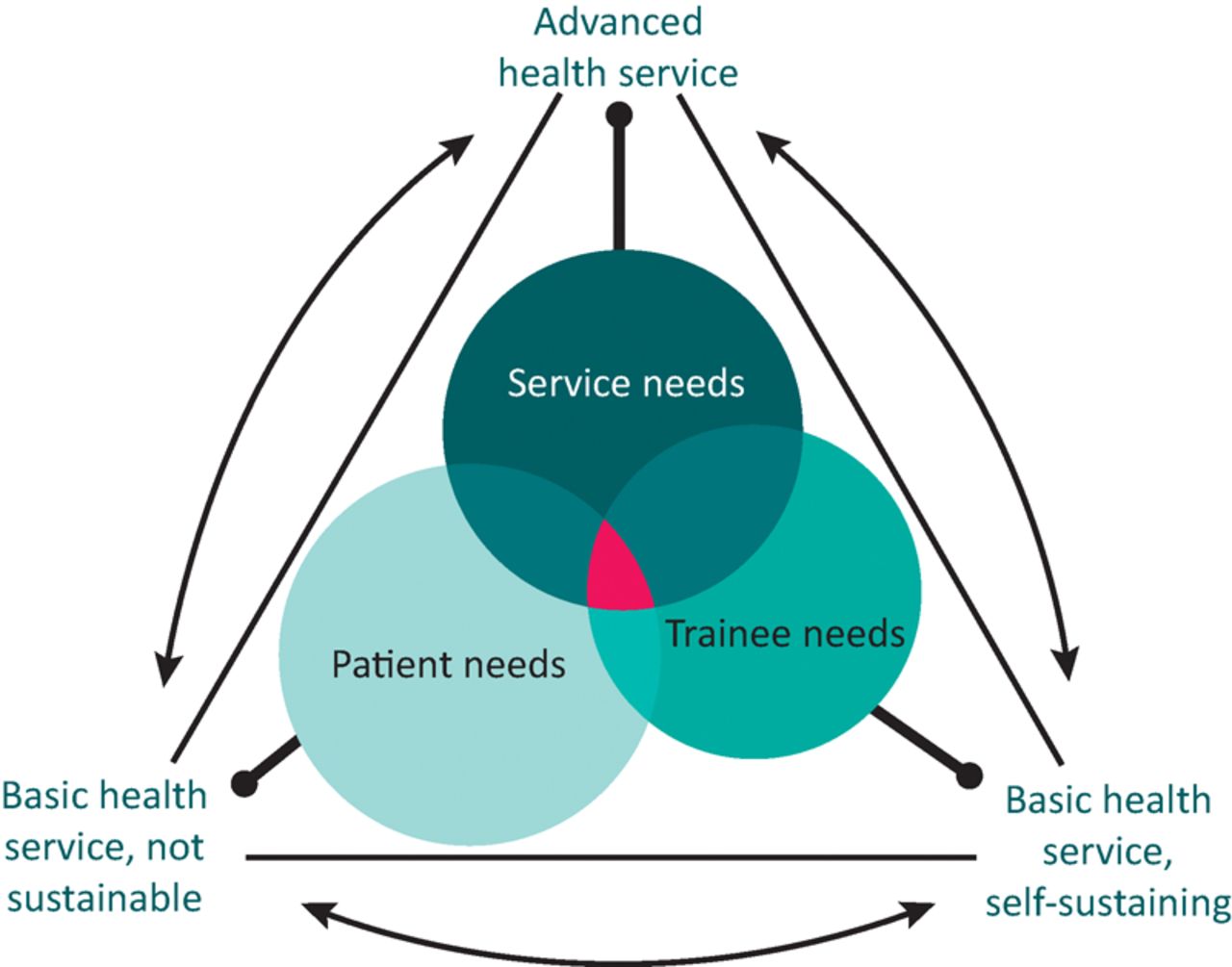
The intersection between patient, trainee and service needs, and the impact of these on the type of health service delivered. Although patient needs are paramount, a service that caters only to these is not sustainable in the long term. Similarly, a service that invests in training but not overall development will be limited. An advanced and optimally functioning health service will cater to higher–level organisational needs with a view to developing and further improving the service. This necessitates fulfilling the needs of patients, doctors and the wider community.
Current training
Following 2 years of foundation training, UK physician training is entered by two routes, via either the 2-year core medical training or the 3-year acute common care stem (Fig 2, Pathway A). Selection into medical specialties occurs after completion of these training programmes, and on attainment of full membership of the RCP. Most medical specialties dual accredit, and training in specialty and general internal medical (GIM) is usually intertwined over a minimum of 5 years. A dual Certificate of Completion of Training (CCT) is awarded after GIM and specialty competencies have been achieved, with a usual minimum total time in specialist training of 7 years. Excluding acute internal medicine (AIM), the proportion of medical specialty trainees dual-accrediting with GIM was 60% in 2014–2015,11 and there remains a significant shortage of GIM trainees throughout the UK.1 The independent Shape of Training review identified changing patient needs as a key factor in deciding how training should be delivered, in addition to the need for a pendulum swing towards generalist training with increased breadth and flexibility (Figs 2 and 3). Highlighting the tensions with service provision in the current climate, the report recommended a shorter period of training, which some have questioned as a cost-saving measure.12 However, the review made a recommendation that the proposed shorter 6-year duration of specialty training be augmented by an additional optional year, to be taken at any point, with the aim of developing management and leadership skills outside the clinical setting (Fig 2). The FHC report,9 published almost simultaneously, made similar recommendations with regard to the need for more generalists, and increased participation in acute and GIM service provision across all specialties. These findings were reflected in the 2014 review by the Joint Royal Colleges of Physicians' Training Board, which strongly encouraged (although did not mandate) dual training with GIM for all medical specialty training.13

A – Current postgraduate physician training pathway16 and B – Shape of Training postgraduate physician training pathway (adapted from the Shape of Training review2). ACF = academic clinical fellow; ACCS = acute common care stem; CMT = core medical training; CPD = continuous professional development; GIM = general internal medicine; MRCP(UK) = full membership of the Royal Colleges of Physicians; OOPE = out of programme for experience; OOPT = out of programme for training.

The five themes identified in the Shape of Training review contrasted with the training goals of the future physician.
Importantly, the Shape of Training review recommended the removal of a selection nodal point at ST3 in favour of achievement of a single Certificate of Specialty Training (Fig 2, Pathway B), rather than separate certification of completion of core medical training or acute care common stem specialty training followed by completion of additional further specialist training (CCT) (Fig 2, Pathway A). In addition to shortening and simplifying the specialty training programme, a more streamlined pathway would allow increased flexibility and individualised ‘theming’ of training, with the ability to flex in and out of academic and clinical training naturally as research and clinical interests develop. Despite the recommended immediate timescale of these changes in the Shape of Training review, there has been little progress in moving towards the type of training envisioned by either this review or the FHC report,14 with some trainees calling for a halt to implementation.15 Finally, because both the review and report were high-level strategy documents, neither made any specific recommendations about how competencies and progression of training in general should be assessed. Currently, both training time and experience are used as metrics, with recommended targets of patient numbers seen on the acute ‘take’ and numbers of clinics before CCT16 in addition to evidence of attendance at delivered teaching sessions, formally assessed clinical case management and procedural competencies. Assessment takes the form of an annual review of competence progression, which includes appraisal of a stand-alone electronic log of training activity, the NHS ePortfolio.17 This is a basic and somewhat unwieldy web-based application with extremely limited facility for cross-platform integration with other online training resources or software, and is generally unpopular with trainees and trainers alike.18–20 However, the ability to record details of training activities could facilitate a move towards increasingly competency-based CCT assessment, potentially shortening training duration.
Future training
To best meet the needs of patients, doctors and the future NHS, we propose a model with the aim of developing the future physician. Building on the Shape of Training review and the FHC report, we identified four broad goals of medical training with integral development of technological skills and digital innovation (Fig 3), and mapped these to the GMC ‘duties of a doctor’ (Fig 4).

Future physician proposals and goals mapped to the four General Medical Council (GMC) ‘duties of a doctor’ domains.
Goal 1: meeting the needs of future patients and services
The quality of patient care should come before all other considerations in the leadership and conduct of the NHS, and patient safety is the keystone dimension of quality.
Don Berwick21
Patients admitted to NHS hospitals are generally sicker than ever before, with multiple comorbidities and increasingly complex care needs, in part a reflection of our ageing society.22 Against this background, the FHC identified the need for ‘stable medical teams that deliver both high-quality patient care and an effective environment in which to educate and train the next generation of doctors’.9 Even within clearly identified care pathways, the Carter review found unwarranted and unacceptable variability in productivity, efficiency and quality of care across non-specialist acute hospitals in England.23 Given that acute medicine operates in a resource- and time-poor environment with high patient turnover rate and acuity, these findings are perhaps not unexpected. As an inappropriate corrective measure, the balance of service provision to training is skewed in AIM relative to other medical specialties, with trainees spending over 70% of their time spent in service provision, one of the highest proportions of service delivery among medical specialties. This is likely to contribute to the overall poor satisfaction rates among AIM and GIM trainees.11
It is likely that this unfavourable training:service delivery ratio has contributed to acute medicine being unable to recruit to approximately half of the advertised posts at the ST3 and consultant levels for the last few years.11 As such, the hopes that the specialty of acute medicine would be able to significantly reverse the trainee shortfall have not been realised and, to provide consistent, high-quality care under current pressures, general and acute medicine must improve recruitment and retention rates in the short term. Looking to the future, however, generalism must be made central to training to cater for the ever-increasing complex care needs of patients throughout their journey as inpatients and beyond. Finally, to optimise patient care and safety, the Carter review favours ongoing and increased centralisation of services.24 This reorganisation is likely to affect where and how physicians are trained. These two factors warrant an alternative model of acute generalist training, while still maintaining an ‘appropriate balance’9 between generalists and specialists to tailor care to changing patient needs.
Goal 2: the hospitalist as central to training and patient care
Today, hospital medicine is a respected field whose greatest legacies may be improvement of care and efficiency, injection of systems thinking into physician practice, and the vivid demonstration of our health care system's capacity for massive change under the right conditions.
Robert Wachter25
The UK has long adopted a model of delineation of care between primary and secondary care providers, with medical patients increasingly admitted to short-stay acute medical units, usually staffed by a combination of AIM and other rotating medical specialties.26 The care of patients with multiple comorbidities requiring longer admissions is usually transferred to a handful of ‘generalist’ specialties, with a significant contribution from geriatric medicine. In some hospitals, ‘emergency’ or ‘acute’ geriatricians also admit directly to the acute medical unit alongside their AIM colleagues, given that the benefit of early, holistic and continued care for older patients is well recognised. In the USA, the model of primary care physicians with admitting rights directing and supervising a patient's inpatient journey has been replaced by specialists in hospital medicine (‘hospitalists’) taking over care at the point of admission. This continues until discharge, with specialists and subspecialists providing only a consultative role.27 The growth of the hospitalist movement has exploded, with over 50,000 physicians recruited to the new specialty since the mid-1990s.25,28
The role of the US hospitalist is comparable to that of the UK AIM, GIM or acute geriatric consultant although, in the UK, acute physicians have been isolated in ‘time and space’29 by the acute medical unit. Age as a barriers is also a factor and, together, these limitations have been compounded by a lack of recognition, status and resourcing. The relative failure of the UK to expand general medicine is partly the result of these physical restrictions, but also because of resistance on the part of general physicians. Despite similar initial misgivings in the USA, the hospitalist model has been shown to improve efficiency and outcome,30–32 and also provide a better trainee experience.33 However, there is a significant disparity between the doctor:patient ratio and resource availability in the US hospitalist model, and that of the AIM, GIM or acute geriatricians caring for patients in UK hospitals.34 Lastly, both the hospitalist movement in the USA and acute medicine in the UK have arguably been the vanguard of the patient safety and quality movements, and are well placed to support these in training programmes.
We feel that a similar expansion of future hospitalists in the UK, drawing on the strengths of acute, general and geriatric medicine, would improve quality of care, patient safety and physician training, and help in ‘[re]valuing internal medicine’.35 Removing the restrictions of current practising patterns will increase flexibility and continuity, and help to elevate generalism while embedding it at the heart of future medical training. While we recognise the substantial differences with regard to training duration, funding and overall organisation of internal medicine between the USA and the UK, we have opted to use the term ‘hospitalist’ to describe our proposed model as a way of descriptively unifying the current medical specialties practising general medicine in UK hospitals, while simultaneously highlighting the broad changes that we are advocating.
Goal 3: flexibility in training and reduced discontinuity
If there were ever a group defined by lacking plasticity, it would first apply to doctors.
Eric Topol36
The Shape of Training review highlighted the need for increased flexibility in UK specialty training to meet the needs of the changing medical workforce.2 Currently, there is little room for flexibility on the part of either trainees or workforce planners, with specialisation occurring early and little room for pursuing other clinical interests later in training. In addition, training is organised on a rotation basis, with junior trainees in particular changing role, hospital or location frequently. This leads to a lack of cohesiveness in training overall, with trainees displaced from training leaders and potential mentors, and also considerable disruption to living circumstances. The perceived loss of control over career and working environment can lead to a lack of engagement and a constantly changing medical team at odds with the stability envisioned by the FHC report.9 Decreasing training discontinuity by setting upper and lower limits in terms of the number of rotations and rotation length, respectively, would help to diminish this, as would applying the hospitalist model of unified oversight of patients to overall rotation quality and education. In addition to creating functional teams echoing the traditional ‘firm-based’ structure, more stability would allow the development of sustained programmes of quality improvement and trainee-led education. Rather than reducing flexibility, increased continuity would allow trainees to better tailor their clinical interests and working patterns vertically across the duration of their training. Flexibility in the workforce would mirror flexibility in training. Competency-based assessment would become a true measure of trainees’ abilities and needs, and longitudinal trainer–trainee relationships would allow gestalt to be identified and developed.
Goal 4: promoting leadership, management and innovation
It is time for physicians to think beyond making their institution, practice, or professional society better. The population needs, and deserves, such leadership. And physicians can provide it.
Robert Brook37
Medical leadership has been increasingly recognised as a desirable skill for doctors at all levels, and trainees have a unique vantage point from which to lead change.38 Increased and visible leadership has been shown unequivocally to improve patient outcomes,39 in addition to contributing to a change in behaviour and culture,40 highlighted by the Francis report as a key determinant of quality of care.3 The hospitalist model recognised the need for clinical leadership at all levels early on, with the result that leadership roles and the development of practical skills fostering innovation are pursued as viable career alternatives to academic medicine. This emphasis has allowed hospitalists to expand a systems-based approach to patient care, focusing on patient safety and quality, and efficiency outcomes. In the UK, the importance of embedding quality improvement into the daily lives of UK physician trainees is increasingly accepted although better integration of management and leadership skills with clinical training is required. In contrast to the Shape of Training review, we argue that this should not be optional, and should be supported by project hubs and resources, such as the RCP-led Learning to make a difference.41 Schemes such as the nascent Future Hospitals’ Chief Registrar Programme provide a framework for leadership training and experience that we would like to see expanded across the UK. Development of these skills should be aided by education in epidemiology, data assimilation and analysis, and better understanding of the use and application of electronic health records and information technology to help drive innovation in patient care.36 In addition, better trainee clinical leaders will be better able to take responsibility for their training and learning needs, which will help to foster the rebirth of medical professionalism, widely acknowledged to be in decline.42,43 Lastly, active and effective leadership is corrective to medical tribalism, with increased engagement allowing the expansion from narrow specialty interests to include the system as a whole.
Challenges
Systems-level change in the NHS has often taken the form of continuous revolution without evaluation, which has, paradoxically, hampered true sustainable change and innovation. Aspects of recommendations in the Shape of Training review have been controversial,15,44 particularly in light of the failure of the Modernising Medical Careers Programme. However, there is an increasing body of evidence from the USA that the central role of the general physician in hospital-based care is successful in terms of reducing length of stay and improving outcomes, and could provide a useful template for change.26 Another challenge is the time taken to implement changes to training, estimated to take at least a decade, according to some commentators.45 We also not only accept that there might be considerable resistance to change on the part of physicians, but also recognise that organisational restructuring within the NHS could force changes that ultimately are less palatable. Finally, a method of assessing quality and evaluating implementation must be developed that has the capability to be responsive within a reasonable timeframe, to allow iteration and refinement of the training pathway.
Conclusions
General medicine is at a crossroads, and it must adapt to survive, let alone thrive. Although integral to our current system, the logistical restrictions on acute medicine mean that it will struggle to deal with increasingly complex patients with multiple comorbidities. Retaining medical specialties in a consultative role with inpatient medical care managed by a new model of future hospitalists could improve efficiency while maintaining the quality of care. The future physician model fits well within the aims of the FHC and the broad-based training envisioned by the Shape of Training review and, with appropriate safeguards, this has the potential to provide better career development for trainees, with an associated positive effect on workforce planning.
Conflicts of interest
FJ is a Future Hospital Officer.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}