
ABSTRACT
Demand for assessment at the acute medicine receiving unit (AMRU) regularly exceeded the capacity of the AMRU to assess and treat in a timely way. Audit work suggested that 28% of patients arriving could have had their care delivered in an alternative setting by a service that was already available. The system of referral was redesigned to re-introduce a mandatory GP to consultant clinical conversation to enable navigation of patients to the most appropriate clinical setting. This has relieved pressure on the AMRU and means that patients are directed to the right clinical setting, first time, more of the time. The numbers of patients presenting to the AMRU following such a conversation who could have had care delivered in an alternative setting has dropped below 5%. The ambulatory care rate for the AMRU has been maintained at 43%.
Introduction
We report long-term outcomes of collaboration between primary and secondary care to improve urgent care for adult medical patients presenting to the acute medicine receiving unit (AMRU) at Nottingham University Hospitals NHS Trust. Nottingham University Hospital is a 1,700 bedded, split site acute teaching hospital. The single emergency department and unselected medical take are sited on the Queens Medical Centre (QMC) campus. A number of dedicated pathways offer direct access to specialties on QMC and City campuses. Other adult medical patients with urgent secondary care needs are referred into the AMRU on QMC campus from the community. In the AMRU, patients are assessed and treated as ambulatory whenever safely possible. When medical admission is required, patients are transferred from the AMRU to the medical assessment wards.
Over many years, demand for unselected medical admission has risen. GP referral to hospital changed from a conversation between a primary and secondary care doctor – typically a GP and medical senior house officer – to a system of ‘fax and send’ with patients registered for admission through a largely administrative pathway. As attendances increased, the urgent care pathway through acute medicine became overstretched and there was an urgent need to find ways to relieve pressure on the service.
In 2009, GPs requesting patient admission to the QMC were asked to complete a 1-minute survey asking whether and how hospital referral might be avoided. The data (unpublished) from 9,112 calls suggested that in 2,597 cases (29%) attendance at the medical admissions unit could have been avoided. Of these 2,597 cases, 1,148 patients (44%) required access to diagnostic tests, 1,072 (41%) needed access to clinical expertise by phone and progressively smaller numbers cited the need for community beds, community nursing care, social care and mental health services. These alternatives would have been needed on the same day as the call in 89% of cases. This finding supported the development of a number of ambulatory pathways, such as deep venous thrombosis and outpatient antibiotic therapy services.
Although alternative pathways were utilised, attendances to the AMRU continued to rise. By 2013, unselected medical attendances to the AMRU had increased beyond the capacity for timely discharge or transfer. There was crowding in the afternoons and evenings and the unit routinely remained open overnight.
Data from GP calls that were being managed by non-clinical call handlers showed that fewer than 5% of patients were being diverted to established alternative services. The scripted algorithms used by non-clinical call handlers did not direct patients to alternative services – partly because they were overridden by the referrer. An audit on the AMRU suggested that 28% of those arriving could have been cared for by services that were either available or could be made available with modest service reconfiguration.
Solution
GPs wished to avoid hospital assessment where possible and requested access to a consultant to help identify alternatives to an unselected medical admission. Over a period of 6 weeks, a clinical working group of two GPs, three consultants and two nurses were supported by data analysts and project managers to redesign the pathway from the GP to the AMRU and to potential alternatives. Over 6 weeks, acute medicine rotas were reorganised to provide consultant time for telephone triage, a service directory of existing alternatives to admission was updated and the new ‘telephone triage’ line was made live.
Between 9 am and 5 pm, a consultant physician was then available to discuss potential unselected medical admissions directly with the referring GP. Subsequently, the conversation between GP and consultant was made mandatory by the clinical leadership team involved. This was to ensure that GPs were making use of existing alternatives to an unselected medical assessment or admission – navigating the patient to care in the ‘right place, first time’. A web application – the Nottingham Care Navigator – was then developed to provide access to centralised referral guidelines and contact numbers for all specialties and services, which could provide alternatives to unselected medical admission.1
Outcome
AMRU attendances
Since 10 November 2014, 32 acute and general physicians have worked 545 days of telephone triage and taken over 15,000 calls. 89% of calls were handled by acute physicians. Data capture has been complete on 531 days, meaning that data from November 2014 to the end of December 2016 are substantially complete – there is no record of outcomes for 6 days and there are 8 days where only 4 of 8 hours of data were recorded.
There were 26 calls per day in 2014, 28 in 2015 and 30 in 2016. Mondays and Fridays were busier (32 calls) than Tuesdays to Thursdays (27 calls).
Overall, 72% of all potential unselected medical admissions were discussed at telephone triage. Of those discussed, only 58% needed to come to the AMRU on the same day. The GP was able to manage 16% following telephone discussion alone, 24% were directed to alternative specialties (7% as outpatients, 17% as inpatients) and 2% were seen on the AMRU the subsequent day.
28% of potential unselected medical admissions were not discussed at telephone triage prior to arrival on the AMRU. The majority of these calls came between 5 pm and 10 pm when many alternatives to admission become unavailable. Extending telephone triage beyond 5 pm was not considered to be cost or clinically effective.
The proportion of calls managed through advice alone increased from 8.2% in 2014 to 13% in 2015 and 19.5% in 2016. The proportion of calls that translated into medical admissions reduced from 64% in 2014 to 59% in 2015 and 56% in 2016. The numbers diverted to specialties other than acute medicine has fluctuated between 21 and 26%.
Of all patients presenting to the AMRU (those following telephone triage, those presenting after the triage line closes and a small number from other sources), 57% now require admission and 43% are dealt with as ambulatory cases – ie discharged without an overnight stay.
There has been a marked and sustained drop in AMRU attendances (Fig 1). Re-audit of the AMRU following the implementation of the telephone triage service showed that fewer than 5% of people attending the AMRU could have their needs met elsewhere in the system (28% previously). The numbers attending the AMRU subsequent to June 2015 (Fig 1) have not changed substantially.

Acute medicine receiving unit (AMRU) attendances before and after telephone triage.
LCL = lower control limit; UCL = upper control limit
AMRU processes
The relief from crowding enabled efficiency improvements in the AMRU. Between August 2014 and May 2015, the mean time from admission to nurse triage dropped from 30 minutes to less than 15 minutes, medical clerking from 125 to 56 minutes and senior review from 181 to 115 minutes. Average length of stay dropped from 5 hours 48 minutes to 3 hours 28 minutes for ambulatory care and from 8 hours 48 minutes to 3 hours 47 minutes for those who were admitted.
These efficiencies increased ambulatory care rates for those patients where no alternative had been found through telephone triage. The ambulatory care rate of 43% in the AMRU has been maintained despite the number of patients navigated to alternative services.
Fig 2 shows substantial improvements in patient experience for those who presented to the AMRU following the introduction of the telephone triage. To ensure that all comments were recorded, cards that contained positive and negative comments were counted in both categories.

Patient feedback before and after telephone triage.
Fig 3 shows that there has been no corresponding step change in numbers presenting to the emergency department. The graph also includes data following the subsequent introduction of surgical triage into the admissions system.
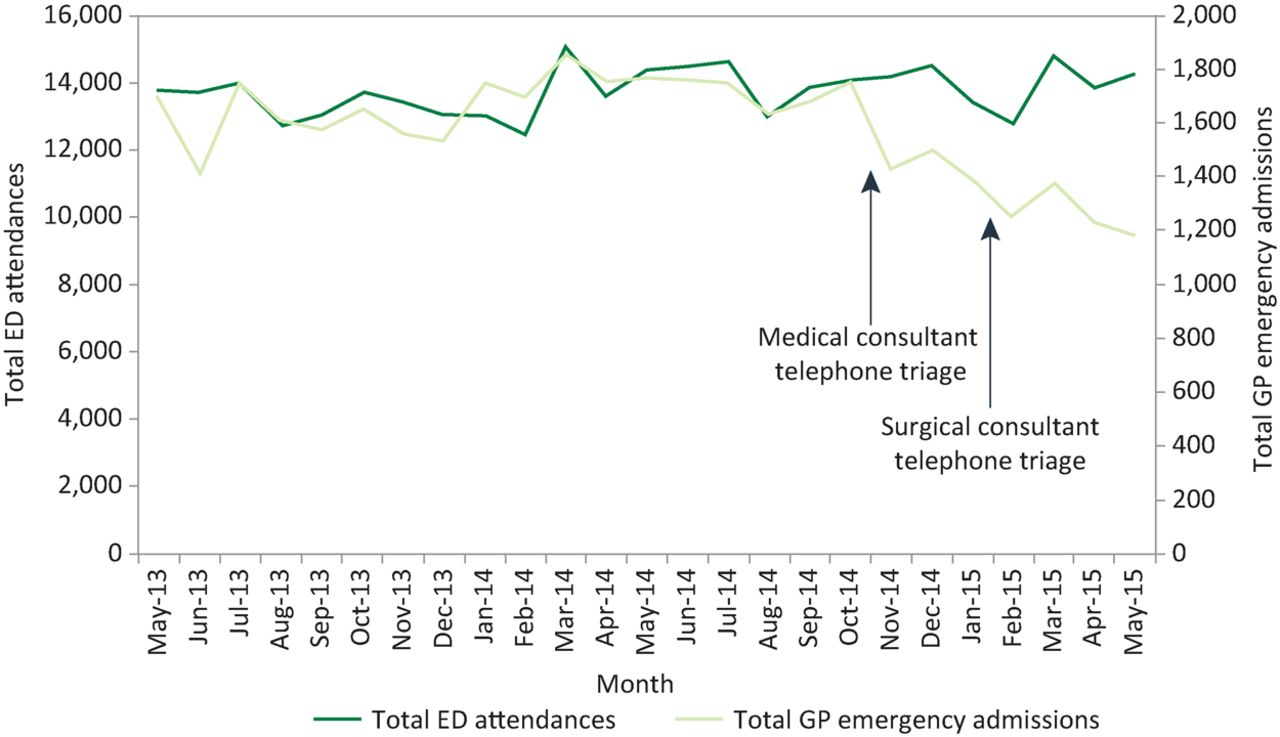
GP emergency admissions and emergency department (ED) attendances before and after telephone triage.
Discussion and conclusions
Previous process improvements had removed many steps in the process of GP referral for medical assessment in hospital. No readily available source of urgent clinical advice for GPs was then available. Alternatives to urgent acute medical assessment were under-utilised and demand for unselected medical assessment and admission through acute medicine continued to rise.
This article describes the consequences of (re)introducing a clinical conversation between the primary care provider (usually a GP who has assessed the patient and has a full understanding of their clinical problems) and a consultant in secondary care (in this case, an acute physician with expert knowledge of alternatives to unselected medicine). These conversations are now supported by the Nottingham Care Navigator app for Android and iPhone, which lists services and contact details.
The reduction in GP-directed admissions seen in acute medicine has been mirrored in other high volume services in Nottingham, such as emergency general surgery (Fig 3) and acute oncology – which have also developed direct telephone lines to support GPs and patients, respectively. These services have shifted care from hospital admission toward telephone or ambulatory care. Assessment units have become less crowded and ambulatory processes more efficient. Patient and staff satisfaction with care have risen.
The emergency general surgery and acute oncology services are not discussed in detail as part of this report. Call volumes are lower in surgery, allowing the surgeon to undertake other duties in parallel to providing telephone triage. The acute oncology advice line primarily provides support to avoid emergency admission after chemotherapy and is staffed by specialist nurses.
The financial cost of providing the service in acute medicine is approximately £157,000 per year based on salaries for a consultant solely taking telephone calls from 9 am to 5 pm, administrative support and the cost of a networked computer, telephone and estate. This may reduce as ongoing process improvement reduces the need for administrative support.
Some estimates of financial savings can be made. For example, the telephone triage service substituted an admission with advice to the GP for 16% of calls (1,219 patients) or an outpatient appointment with a consultant for 7% of calls (498 patients). Conservatively, if admission avoidance saved 1,717 overnight admissions for these patients at a nominal unit cost of £400, telephone triage saved the health and care system over £500,000 once the cost of outpatient attendances are taken into account.
In addition, 17% of patients were admitted directly to specialties rather than acute medicine and the ambulatory care rate for acute medicine continues to run at 43% – maintaining quality of care while respectively mitigating excess length of stay and the need for admission.
Finally, previously pressing financial and clinical pressures within the AMRU have been reduced to a great extent. Staffing now matches workload more closely and has not needed to increase. Recruitment and retention have improved. Patient and staff feedback suggests that the quality and timeliness of care have improved.
This paper demonstrates that (re)introducing a clinical conversation into urgent referral pathways reduces admissions and moves patient care to the right place, first time, more of the time. Within the current commissioning system, a tariff per call can be calculated to provide an additional financial incentive for providers of acute care to reduce admissions – an approach being used in a number of areas.
Conflicts of interest
The authors have no conflicts of interest to declare.
Acknowledgements
We would like to acknowledge Dawn Lapworth, Lynne Lee and Sophie Edwards who supported the development and implementation of this service.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
{kind=link}