
ABSTRACT
In some healthcare systems, patients are cared for by single organ, or single system, specialists; this undeniably has a place in high-quality, effective patient care. A patient who is having a myocardial infarction would understandably want to be under the care of a cardiac specialist to ensure their treatment is effective, evidence based, and up to date. However, in the current climate of an ageing population, long-term chronic diseases and patients with multiple comorbidities, we are in need of generalist inpatient physicians too. After all, a frail, cognitively impaired, diabetic octogenarian with advanced renal impairment who is having an acute coronary syndrome is very different from a middle aged individual with an acute coronary syndrome. Hospitalist medicine in the USA provides this high-quality generalist inpatient medical care. This article explores the model at Rush University Medical Center in Chicago and any lessons we in the UK could learn from them.
Introduction
The NHS is facing challenges on an unprecedented scale: an ageing population, people with chronic illnesses living longer and many patients having multimorbidity. Patients’ length of stay (LOS) is now shorter than it has ever been and thus probably more intensified.1 Clinicians should have the necessary knowledge and skills to care for such patients. It was for these reasons that I decided to explore an alternative existing system like hospitalist medicine and evaluate if any aspects are translatable to the UK.
In 1996, Dr Robert Wachter, chief of medicine at the University of California San Francisco Medical Centre (UCSF) and Dr Lee Goldman, chair of UCSF’s Department of Medicine, coined the term ‘hospitalist’.1 In naming a physician whose practice is dedicated to caring for a patient during the entirety of their hospital stay, they started a new movement. Prior to this, primary care physicians would manage these inpatients in addition to their regular outpatient commitments. They would review patients on a regular basis (usually daily, but this varied between practitioners) and would fit this in between their outpatient commitments. This has never been the case in the UK, where primary care and secondary care have always been clearly delineated.
Hospitalists usually care for all medical inpatients and, in some organisations, every single inpatient, 24 hours a day, 7 days a week. Earlier this year, hospitalist medicine was formally recognised by the Centre for Medicare and Medicaid Services (CMS) with a dedicated billing code.2
The requirement for hospitalists arose when junior doctors in the USA were subjected to working hours restrictions. In order to ensure compliance with these restrictions, senior physicians would end up spending more time in the hospital and on the wards.3 There was also a financial impetus for hospitalists as CMS made a decision to reimburse organisations on a fixed-term, discharge diagnosis rate instead of a daily fee. As a result, it was more cost effective to reduce a patient’s LOS and have a higher turnover of patients.4
The UK found itself in a similar situation when the European Working Time Directive and the emergency department 4-hour targets came into force.5 A new specialty, acute internal medicine (AIM), was proposed by the Royal College of Physicians in 1996 to facilitate this change in working practice. Almost 20 years later, the field of acute medicine is the UK’s fastest growing specialty with approximately 600 trainee and recently trained physicians.5 In 2002, there were more than 20,000 hospitalists in the USA, a size comparable to cardiologists. By 2015, the numbers had more than doubled to approximately 48,000.2,6
Both of these relatively new specialties provide generalised care for patients; AIM caters for patients in a dedicated unit (acute assessment unit), usually in the first 48–72 hours of their inpatient stay, before they are transferred to a specialist ward and team. The hospitalists on the other hand, work hospital wide.
The Winston Churchill Fellowship
As a trainee in AIM, I have always been interested in exploring systems that share parallels with ours. AIM is a relatively new specialty and should be utilising every opportunity to learn and develop from those around us. In 2015, I was awarded a prestigious Winston Churchill Travelling Fellowship to learn more about hospitalist medicine at Rush University Medical Center in Chicago, Illinois.
Rush University Medical Center
Rush Hospital is based in outer Chicago, where there are two other hospitals within a 3-mile radius. The hospital has approximately 50 medical admissions per day. There are 130 medical beds and the hospitalist medicine faculty consists of 38 physicians, including six nocturnists (these are hospitalists who only cover night shifts), who contribute to the rota. There are eight hospitalist teams covering general medicine.
Tables 1 and 2 provide more details regarding the structure of the teams.
The teams that are on call in a day and the maximum number of patients they will admit
4-day rolling rota for a hospitalists’ team
Surgical co-management
In 2007, Rush commenced its co-management service; this is shared perioperative care. The surgeon remains the patients primary doctor; however, the hospitalists review the patients daily, can write prescriptions and make decisions related to the patients’ care. In addition, there are daily pre-assessment clinics run by the co-management team. This service has similarities with orthogeriatrics care in the UK.
The studies on the effect of co-management on patient safety are limited in number and scope. The Mayo clinic undertook a study in 20057 and this revealed there was no difference in LOS and adverse patient effects. Those who benefitted from co-management were patients who did not have any complex medical issues. However, this was a relatively small study and undoubtedly further research is required in this field.7
There is a wider evidence base for hospitalist medicine as a whole, which will be discussed in this article.
Physician associates and advanced nurse practitioners
Physician associates are more established in the USA than the UK, where they are a relatively new concept. These clinicians provide physicians and their teams with assistance. The physician associates see patients independently on their own ward rounds and some also have their own unsupervised clinics.
The observation unit admits patients who are low risk and require admission for less than 48 hours. The unit is run by the hospitalist medicine faculty. The admission criteria are comparable to that of ambulatory care units in the UK. One attending physician and one advanced nurse practitioner run the department. The advanced nurse practitioners have the ability to review patients daily, perform procedures, such as pleural drains and ascitic drains, and make discharge decisions.
Interviews
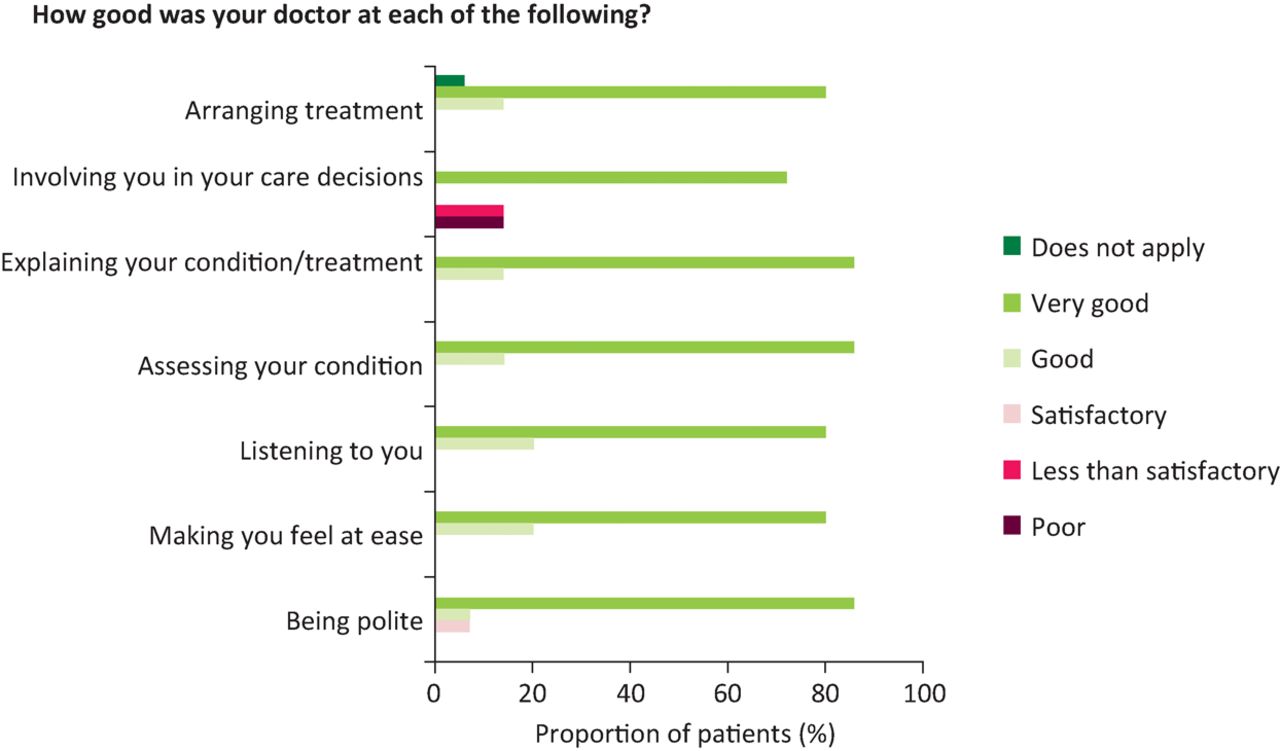
In December 2015, structured qualitative interviews were conducted with a small number of patients admitted under hospitalist medicine at Rush over a 2-week period. These interviews were recorded, transcribed and thematically analysed. As part of this process, patients were also given the UK General Medical Council patient satisfaction questionnaire to anonymously complete; Fig 1 illustrates some of these results.

Results for question 4 of the General Medical Council patient satisfaction questionnaire. This was conducted as part of the patient interviews at Rush University Medical Center. Generally, the majority of patients answered good or very good to the questions. A small proportion of patients did not feel they were adequately involved in decisions regarding their care.
Interviews with patients revealed that, as a whole, they were happy with the care they received from the hospitalists and from Rush. Attending physicians, upon meeting patients for the first time, would identify themselves and would provide patients with a business card containing their picture, qualifications, specialty and contact details. Thus, patients were always aware who their attending physician was. The majority of patients thought their hospitalist had an appropriate range of knowledge and communicated well with them. Patients did not mind moving ward if necessary as long as the communication between the different care providers was good and they did not have to keep repeating their medical history. There was a minority of patients who would have preferred their primary care physicians to care for them while in hospital as they had a more established relationship with them. Two patients, who both had long-term chronic illnesses preferred to be under the care of a specialist. They associated being a specialist with being more knowledgeable and more respectable. They did not mind if the specialist asked other physicians for assistance if the problem was outside of their area of expertise.
Many of the hospitalists I spoke to chose this specialty as they enjoy the variety of cases they see, like inpatient medicine and have more flexibility to pursue other areas of interest, such as teaching and management. The applications for hospitalist residents/attendees are always oversubscribed at this organisation. Unfortunately, some hospitalists worry that they are not respected as much as their specialist colleagues, that they are often seen as ‘super-residents’ – likened to staff and associate specialist grade doctors in the UK. It was difficult to objectively quantify this perception and this could potentially be an area of further work looking into perceptions of hospitalist medicine by hospitalists and non-hospitalists as well as patients.
The more senior hospitalist faculty members believe that as their specialty is becoming more established, there is an acknowledgement and familiarity with the role of hospitalist physicians, thus leading to recognition and respect. In addition, some hospitalists have created a niche for themselves, creating their own unique selling point. For example, one of the hospitalists at Rush has become an expert in perioperative anticoagulation management and as he is always present is able to provide prompt advice to surgical colleagues.
All the other specialists I spoke to held the hospitalist medicine faculty in high regard. They respected the consultations, which they believed were appropriate the majority of the time, and felt the hospitalists excelled at providing inpatient care.
Although primary care physicians took some time to get used to the new way of working with the arrival of hospitalist physicians, once it was more established they felt that they were able to focus on their outpatient practice without losing time or revenue.
What does research show?
While co-management has not been shown to reduce LOS in days, hospitalist medicine has reduced a LOS index compared with other specialties without compromising the quality of care it provides to patients.8 LOS index is calculated by the observed LOS divided by the expected LOS for a given condition, a score of greater than 1 indicates that patients are staying in hospital longer than expected, a score of less than 1 means they are staying in for less than the expected time.
Many institutions, have shown that usually the patient satisfaction scores are similar to or, sometimes, even better than for other physicians, while the readmission rates, mortality and complication rates are lower compared with other internists and primary care practitioners.9,10
According to Rush’s own performance metrics (Rush University Medical Center Information Services Division), the average LOS in 2001, prior to the hospitalist medicine faculty being fully established, was 6.031 for all staff groups. In 2015, the LOS was 4.27 and the LOS index was 0.84 for patients cared for by hospitalists.
Conclusion
A direct comparison of the two healthcare systems is not possible as the structure and financing of the two healthcare systems is very different, for example the USA has an insurance-based system whereas the UK is tax-payer funded.
The current hospitalist model in the USA is not directly translatable to the UK mainly because of our limited general medicine workforce, but a similar structure may be more appropriate – especially in smaller, rural district general hospitals.
There are certain aspects that are more feasible in the short term and these would include the introduction of a model similar to co-management. There is a lack of perioperative medical care in the UK except in the field of orthopaedic geriatric care. Orthogeriatrics emerged as a result of older orthopaedic patients with multimorbidity requiring specialised geriatric care to improve their outcomes. On the other hand, general surgical patients on the whole have traditionally been younger with fewer comorbidities thus able to be managed by surgeons without additional medical input, by and large. Our population is changing and ‘younger’ patients now also present with multimorbidity. Hence, generalists should be able to provide services such as pre-assessment clinics for complex patients, ward reviews during the perioperative period and advice on early rehabilitation.
From my experience, general medical on calls are getting busier year on year, with a heavy burden on the admitting team, so perhaps a reshuffle of the on-call team structure may be necessary. Adopting a ‘long-call/short-call’ type structure in the UK and distributing new patients between a few teams may have patient benefits through ensuring no team is overburdened. In addition to this, those acute assessment units that have the benefit of having a large team could be divided into several sub-teams and adopt a ‘rolling 3-day’ structure and distribute the workload (for example a separate ‘take team’ and ‘post-take team’). The former approach works at Rush University Medical Center and the latter one has been introduced into a few hospitals in the UK. The outcomes from these innovative UK centres will decide whether this system can be rolled out more generally UK-wide.
The UK is in the process of implementing a nationwide 7-day service programme; this requires innovative working practices to ensure consistent patient care 7 days a week. For this, a more generalist approach is required in order to ensure that hospitals have the capacity in each service to provide consistent 7-day care. Hospitalists have the potential to be a useful innovation in the delivery of the 7-day service programme.
There is an increasing role for both advanced nurse practitioners and physician associates in the UK. Some hospitals are already adopting such models. This is a group of clinicians who, if we provide the correct training, can assist with the increasing care requirements in our hospitals, including supporting a 7-day service.
Compared with many other developed nations, the healthcare we provide in the UK ranks highly in many of the aspects of the Commonwealth Fund international survey of 2014.11 In order to ensure we continue to be at the forefront of delivering efficient, high-quality care, we need to be constantly evolving and learning lessons from our international counterparts.
Conflicts of interest
The author has no conflicts of interest to declare.
Acknowledgments
I would like to thank the Winston Churchill Memorial Fund for sponsoring the fellowship. Thank you to Dr Amir Jaffer (Head of Hospitalist Medicine, Rush University Medical Center) and Dr Omar B Lateef (Chief of Medicine, Rush University Medical Center) for allowing me to shadow and interview their faculty and for providing their valuable insight into hospitalist medicine.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.