
ABSTRACT
We set out to understand whether MedNav, a digital decision support tool, improves the quality of neonatal resuscitation practice in resource poor settings. A 6-month long trial in Uganda showed that adherence to good practice increased from a mean of 46% without MedNav to 94% with MedNav. The mean system usability score was self-assessed at 84.5%. While the younger midwifery team liked MedNav, it was unpopular with senior members of staff who felt that staff should not rely on support tools even if they improved clinical practice. Next steps include a larger scale study looking at neonatal survival outcomes and greater attention to the barriers that need to be overcome in order to enhance acceptance and adoption.
Introduction
The World Health Organization estimates that a quarter of neonatal deaths globally are caused by birth asphyxia1 (failure to initiate and sustain effective breathing at birth) and that effective resuscitation could potentially prevent a large proportion of these deaths. Globally, neonatal resuscitation quality is a problem, with error rates and deviation from the protocol of resuscitation by healthcare professionals varying between 16 and 55%.2 These studies were performed in high-income countries and while it is likely that the findings of our study may also be applicable in high-income environments this will need further research.
These issues are exacerbated in resource poor settings where finance, training, qualified staff and equipment are in short supply.
The ‘helping babies breathe’ initiative has had positive, evidence-based, global results affecting clinical outcomes.3 However, it relies on an intensive educational programme of training, master trainers, 3-day training courses specifically for birth attendants, 6-monthly refresher courses and focuses mainly on the initial stages of resuscitation.
Clinicians at Chelsea and Westminster Hospital recognised these issues and worked with a service designer and software programmer to develop a less resource intensive and intuitive alternative.
Solution/methodology
Our approach to these problems is based on the potential of technology to functionally support complex decision-making protocols, in real time, when a baby is born.
MedNav4 has been designed and developed to be the next generation of safety checklists, to avoid the lengthy training needed and to provide real-time, reliable and up-to-date guidance with an intuitive interface, as well as being able to capture contemporaneous audit data and medical documentation.
The service provides step-by-step support for individuals and teams based on the latest clinical advice (Fig 1).
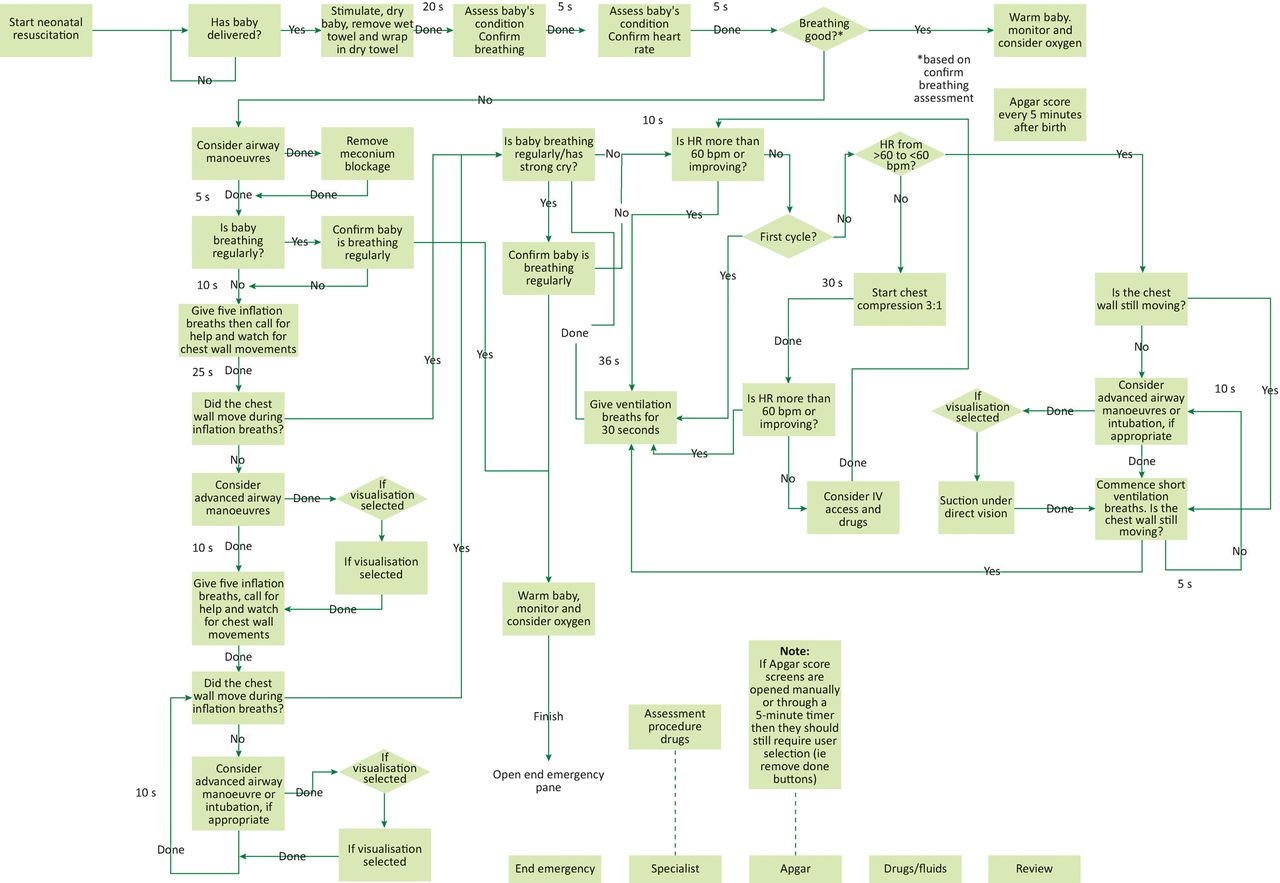
MedNav flow diagram for neonatal resuscitation. HR = heart rate; IV = intravenous.
It is a decision support and activity-prompting tool (Fig 2) that delivers visual and auditory prompts via a touchscreen device whose usability and ability to improve the quality of care has been proven through simulation trials in the UK.5 We set out to demonstrate that this was also the case in a low-income setting and to assess how the use of technology would be accepted.
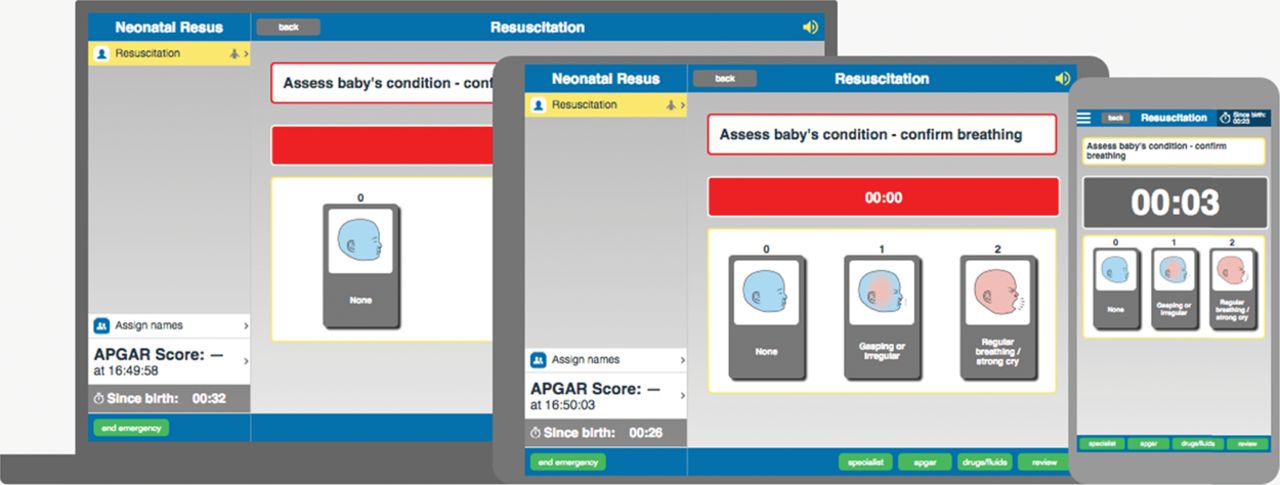
MedNav Neonatal interface on laptops, tablets and smartphones.
MedNav has been designed to operate on a range of low-cost devices, including mobile phones, Android and Apple tablets, and PCs. Once the application has been downloaded to the device, it does not need Wi-Fi to run. While a wired electrical connection is useful, mobile phones and tablet devices can operate without mains power for up to 24 hours before needing to recharge them. This makes MedNav suitable for remote locations with intermittent power supplies although battery backup using PV cells should be considered. The application is designed to be a home screen application running in standby mode so that all the midwife needs to do is to turn on the device from standby to start the protocol. During the trial, and prior to the birth of a baby, the Resuscitaire was checked and the tablet screen and application was turned on in preparation for the birth.
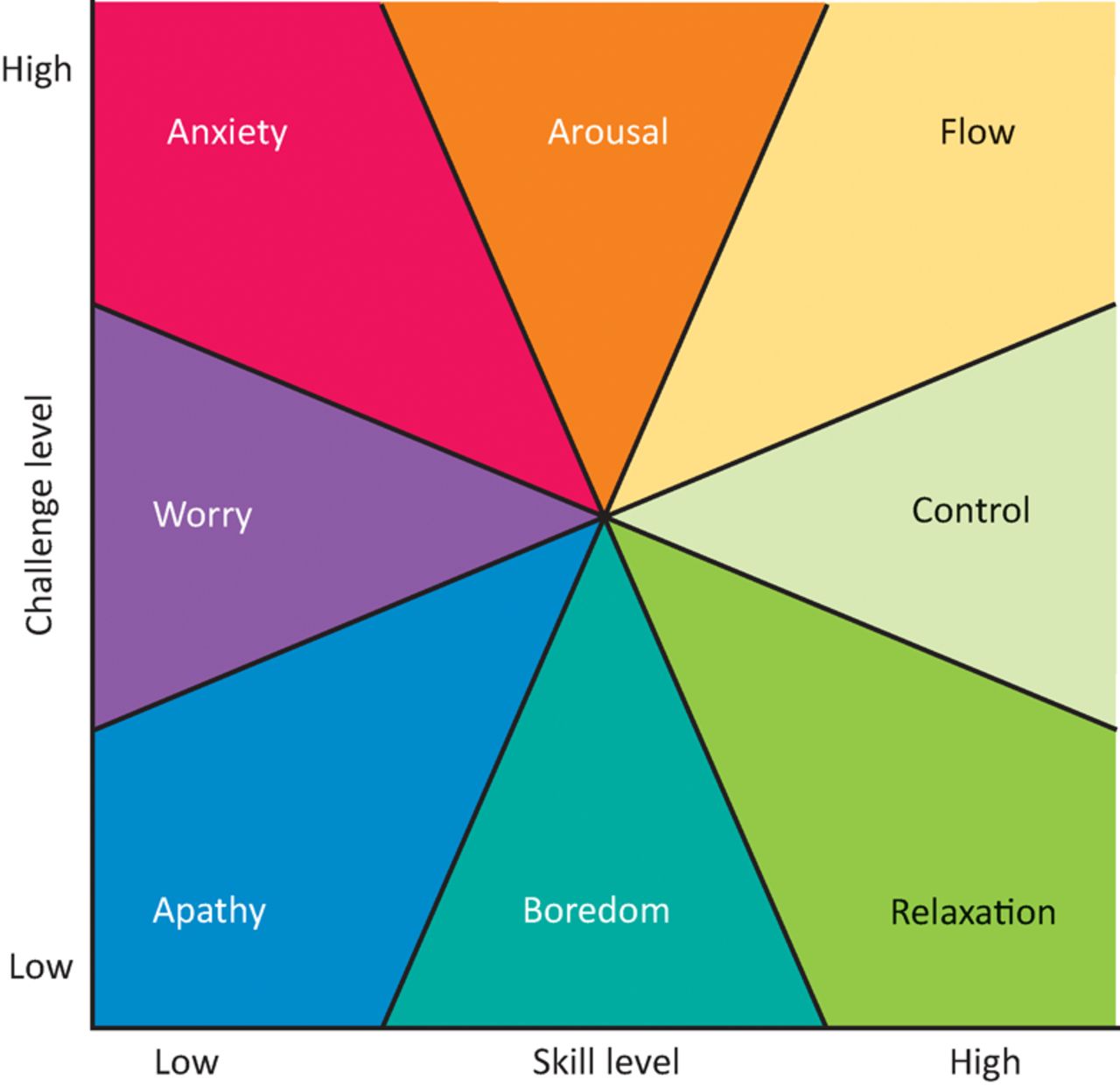
While digital and non-digital medical aids have been used in many clinical settings, we believe that MedNav has unique features that support a more human-centred approach to decision support tools. These include a focus on single tasks to promote a ‘state of flow’ (Fig 3);6,7 multimedia support, including words, images and audio prompts; timers to indicate appropriate lengths for specific activities; together with a recording function that allows teams to refer back to prior incidents for both auditing and training purposes.

Mental state in terms of challenge level and skill level, according to Csikszentmihalyi's flow model.7
To ensure that the service did not slow down the midwife's actions unduly, MedNav includes timers that are in keeping with national guidance. The visual and auditory cues move in line with this guidance and buttons only need to be pressed if tasks are completed before the screen moves forward automatically, or if the task requires a choice that is critical to deciding on the next step. Timers go red to indicate the need to make a decision.
During the trial period, one out of 20 of the MedNav supported resuscitations failed to support the midwife as the touch-sensitive buttons failed to respond to her touch. This may have been a result of excessive moisture on the glove or tapping the screen too quickly. Apart from this event, MedNav operated as expected and did not appear to interfere with successful assessment and support.
The trial was carried out at Kitovu Hospital in Masaka Region, Uganda, under the supervision of Dr Ed MacLaren – a research fellow at CW+, the health charity of Chelsea and Westminster Hospital – and with the support of senior doctor Maura Lynch, an Irish nun who was, until recently, superintendent of the hospital.
The study methods built on standard A/B testing but the sample size and data collection methods were simplified to enable rapid reporting and iteration. In the event, it took 6 months to capture a sample of 46 midwifes (20 using MedNav and 26 without MedNav). The number of resuscitations that we captured was dependent on a medical staff member being present to set up the go-pro camera that was used to capture video footage of the resuscitations.
We compared resuscitation without MedNav with resuscitation attempts using neonatal MedNav. The study was undertaken in the maternity theatre and focused on resuscitation of babies born by caesarean section.
Neonatal resuscitation training was provided prior to the start of the trial to all staff members to ensure that both the control groups and MedNav users had access to up-to-date skills. We ran informal and formal sessions to train team members, visiting all the departments a number of times to ensure that everyone had seen the service (Fig 4). There are deep-rooted factors at play in terms of adoption. Traditionally, team members learn through artistry and with limited experience of a systematic explicit step-by-step based approach of a technical rational approach to practice. Having a device that guided you to what to do next went against this traditional professional artistry view of practice and some found this difficult to adapt to.

Training on MedNav prior to use on the ward at Kitovu Hospital, Uganda.
While MedNav is still in beta development, the team who developed the service, including the authors of the article, have taken steps to commercialise the product to support its roll out and further development. Costs for the software vary between £50/annum for individual users to £6,000/annum for a large teaching hospital or distributed clinical team with up to 5,000 users. Hardware costs depend on the type of tablet and tablet holder that is chosen. In this study, we used an iPad and a commercially available tablet holder that cost approximately £550 plus installation by the hospital's onsite technician. We hope to subsidise charitable and resource poor services through cross-subsidies with income from resource-rich settings.
Outcome
Using the ideal resuscitation as a defined example, we isolated the 12 signal functions that would lead to appropriate, safe and efficient care (Box 1) – these covered assessment of the newborn and initial resuscitation.
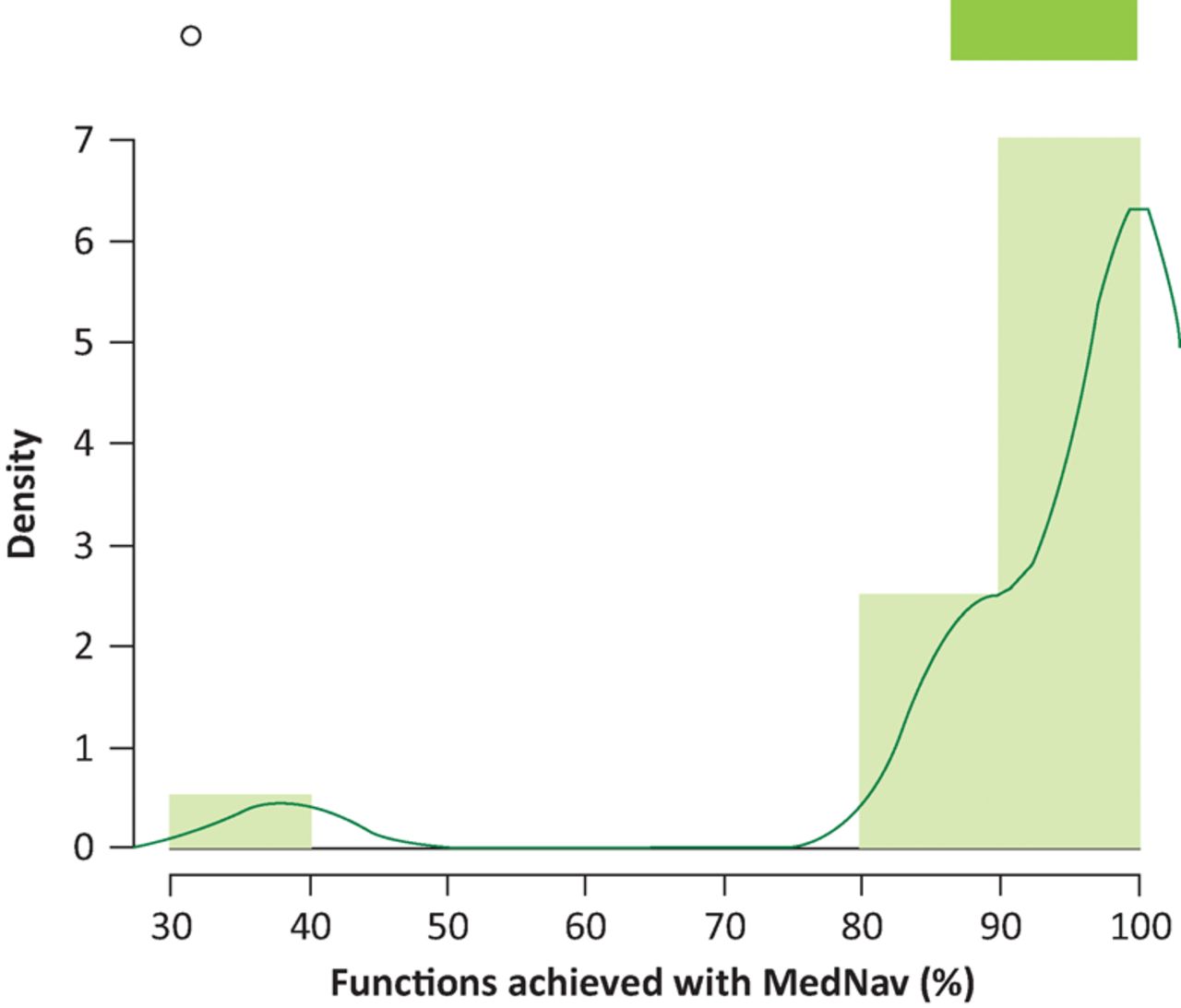
The control group achieved these signal functions with a mean of 46% (Fig 5) in comparison with the MedNav group, which achieved a mean of 94% (Fig 6). This difference adds to the growing body of evidence that MedNav has the power to help professionals in medical emergencies.
Signal functions for MedNav trial
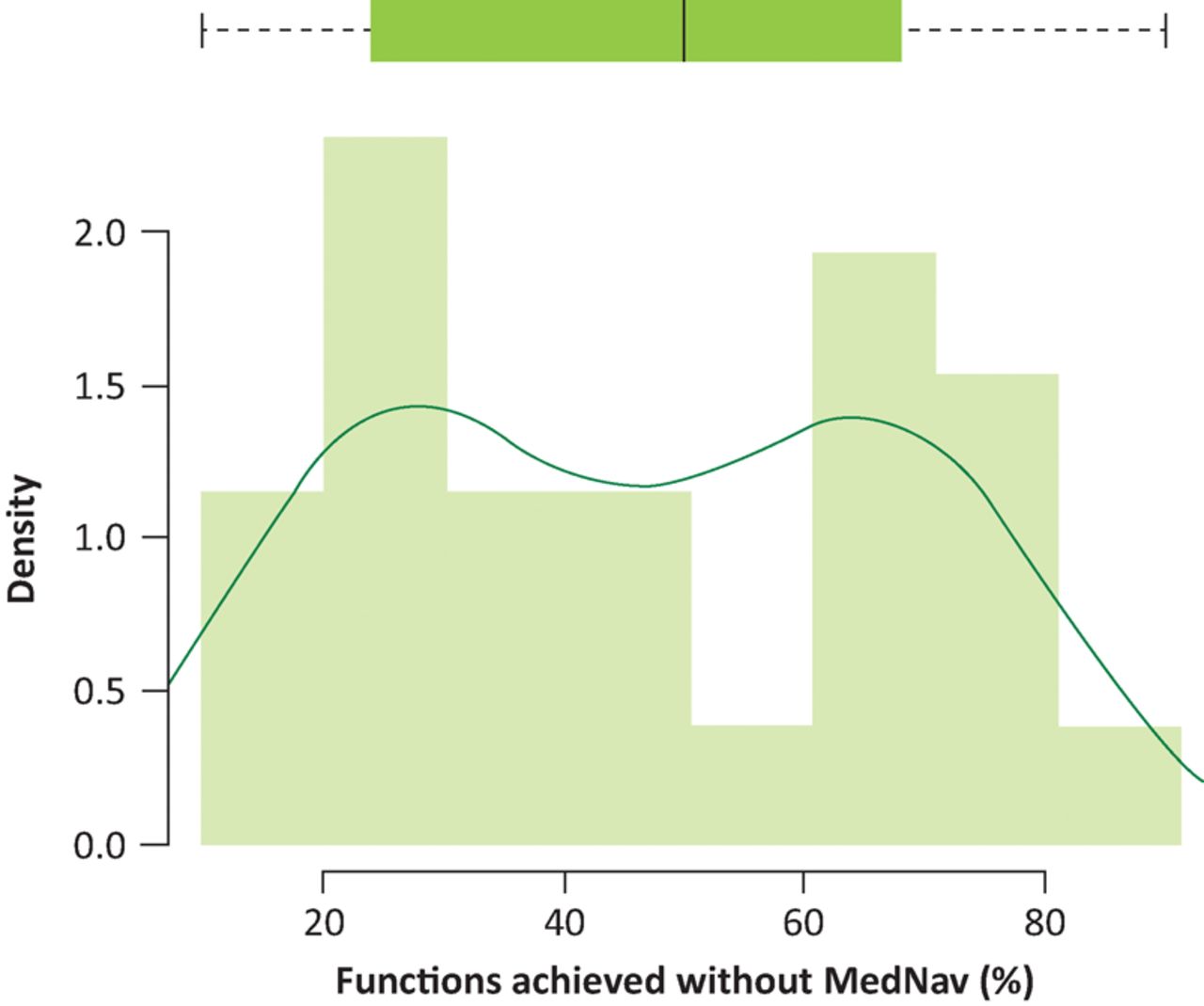
Functions achieved without MedNav. Mean = 0.46, standard deviation = 0.22.
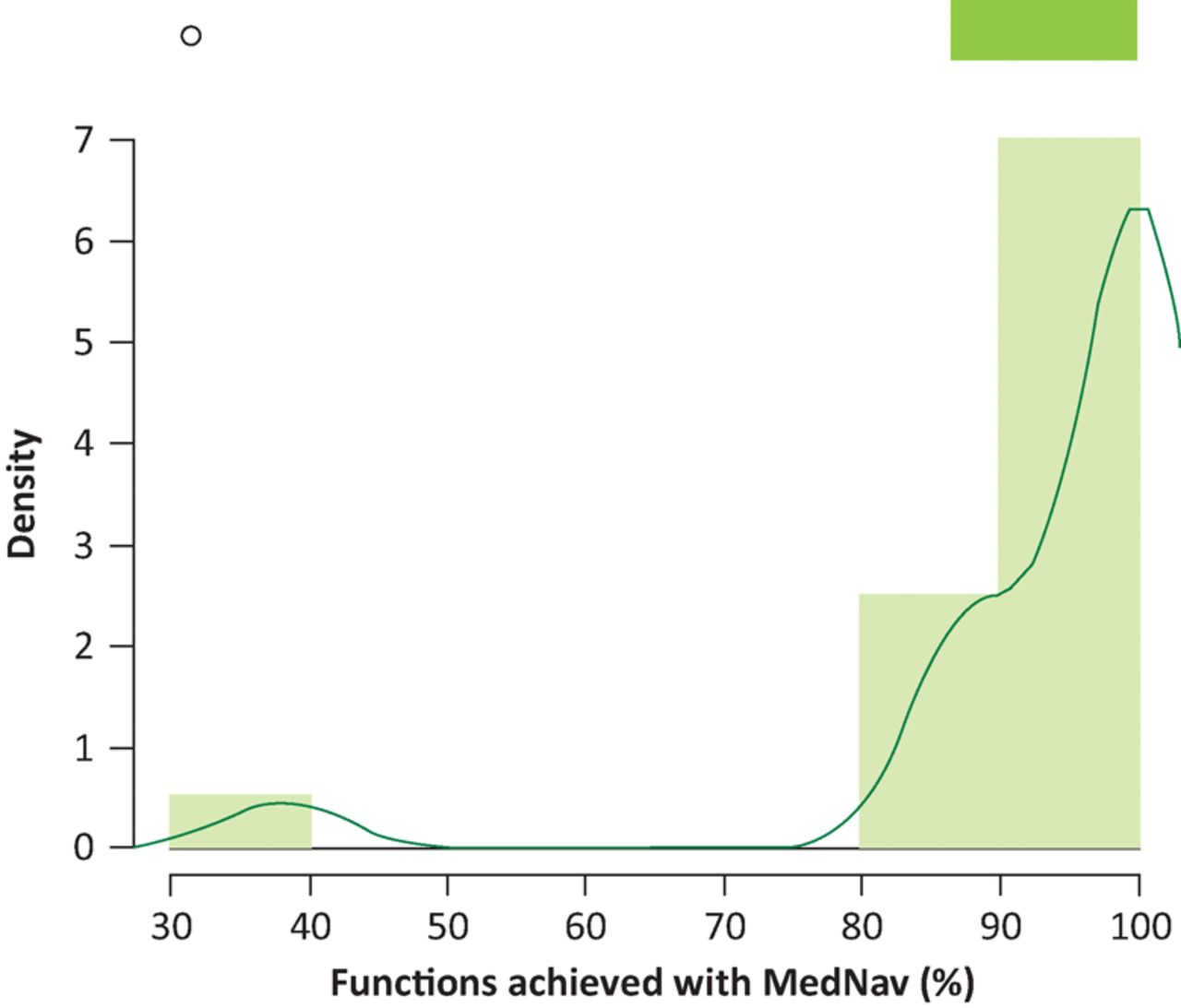
Functions achieved with MedNav. Mean = 0.94, standard deviation = 0.14.
We were also determined to find out how useable the platform was in a low-income setting and how we could adapt it to ensure that it is fit for purpose in the future. Using the validated System Usability Score (SUS),8 MedNav users returned a mean score of 84.5 out of 100 with a standard deviation of 10 (Fig 7).

MedNav trial distribution of System Usability Scores. Mean = 84.5, –standard deviation = 10.0.
Beyond these quantitative measures, we also carried out interviews to understand personal perspectives among the staff, as these will also determine the acceptance and adoption of new technologies.
There was a distinct difference between the younger and older midwives. The younger midwives were quicker to adapt and indeed really relished the use of MedNav while the older midwives didn't like being told what to do or having to interact with a screen. This may fit in with the younger staff having smart phones, but there is also quite a lot of pride associated with positions of power and respect in Uganda. One could make a case that by having MedNav telling people what to do, senior staff authority is undermined.
One neonatal nurse told us that ‘MedNav is nice but we should really just know what to do rather than being told’.
On the other hand, three of the newest midwives said that they thought MedNav was fantastic as they had so little teaching about neonatal resuscitation at midwifery school and really found it useful in guiding them in an emergency (Fig 8).

MedNav being used during neonatal resuscitation at Kitovu Hospital, Uganda.
Another barrier was the managerial team of the unit. The midwifery manager and lead consultant were not interested in the technology, which led to a slower adoption among other staff. These human challenges may well form a greater barrier to adoption than cost or technical integration issues.9
We have not developed a method to overcome cultural resistance to MedNav among senior staff and the managerial team, although we hope that continued use, the results of this study and the follow on analysis of changes in mortality rates over an extended period may help to build a bridge for its future acceptance and adoption.
Conclusion and next steps
These results demonstrate a significant improvement in following the newborn life support guideline for resuscitation when MedNav was used. This has great potential for low-income settings where access to continual professional development and training is limited. Neonatal MedNav has the potential to provide guidance at the time of resuscitation but also to help bridge the gap in medical education by reinforcing the correct practice each time that it is used.
We feel the benefit in low-income countries has the potential to be more significant than in a high-income setting. Staffing levels are dangerously low, so in an emergency there are very few responders. With MedNav acting as an interactive guide it goes some way to ameliorate this risk.
Our next steps include modifications to the service to take into account feedback from the staff; a 1-year study that compares neonatal mortality before and after the introduction of MedNav, both in the operating theatre and on the maternity ward; and a wider application through Saving Lives at Birth: A Grand Challenge for Development.10 In this call, we aim to not only gain a clear understanding of the changes to the quality of neonatal resuscitation in different healthcare settings, but also to understand changes to the service to support greater acceptance and adoption, including training and development, institutional and financial incentives and technical changes to the service platform.
Conflicts of interest
DP received payments from CW+ for the design and development of MedNav. All other authors have no conflicts of interest to declare.
Author contributions
All authors meet the ICMJE authorship requirements.
The authors tweet under the moniker @mednav_team
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.