
ABSTRACT
With the development of the internet, the ability to cascade information at scale and pace has transformed knowledge transfer. Social media, both as an ethos and as the individual platforms that facilitate the development of communities of practice, has created new possibilities in medical education, policy and research. This article explores the role of social media in a new digital world through the lens of its applicability, connectivity and scalability.
When ‘logon’ was entered to start an experimental connection between two research institutes in America in 1969 the system crashed. Despite this setback those tentative steps were the forerunner to Tim Berners-Lee creating the world wide web, which by 2017 contained 4.51 billion pages.1
The transfer of information now occurs on an unprecedented scale in social, economic and political networks. A natural consequence of this connectivity was the development of technological platforms to bring users closer together and share knowledge. Social media is a term used to encapsulate this process but social media are also specific entities, ie the platforms you can share information by (the most commonly known in the western world being Facebook and Twitter).
Social media appears to have had a profound impact on medical practice and those who use it regularly will attest to the advantages of free transfer of information and being participants in communities without hierarchy. Dr Bertalan Mesko compared the then and now of information seeking in a medical context (Table 1).2
Difference in Dr Mesko's online activities
Some, including those reading this manuscript, will find this approach simplistic, perhaps a little dubious and observe that academic evidence of direct patient benefit is relatively scant. In its defence both the evidence-based medicine and quality improvement movements faced similar challenges in the initial phases of their evolution and it should be remembered that social media is still a relatively new phenomena. However, social media is not a means unto itself and should not be seen as a compulsory part of medical practice, ie it is unlikely in the future that all healthcare professionals will have a Twitter handle or write a blog. But to just dismiss social media is as folly as debating whether biros or fountain pens are better for writing in clinical notes. Access to knowledge, the core benefit of social media in medicine, is always likely to remain an individual choice in the same way as you have a choice in how to write. As long as you are acting in accordance with regulations and standards (not breaching professionalism guidance or, to overstate the analogy, using black rather than red ink) then whether you maintain your continued medical education via textbooks, lectures, e-learning, Twitter or any of the other millions of educational platforms available to you doesn’t matter. There are probably no right or wrongs (even if there are organisational or institutional preferences for how you should learn and engage), just different approaches and methods.3 While the advantages of social media are inherently obvious to those who are ‘heavy’ users, the immersive experience required to judge benefit is difficult to encapsulate via written description alone. It is possible though to summarise how social media, as an element of 21st century digital media, is and are beneficial using the following domains: applicability, connectivity and scalability. These will be discussed in turn, but should not be seen as isolated constructs. There are large inter-dependencies making the whole far more than the sum of its parts.
Preferred delivery of education (applicability)
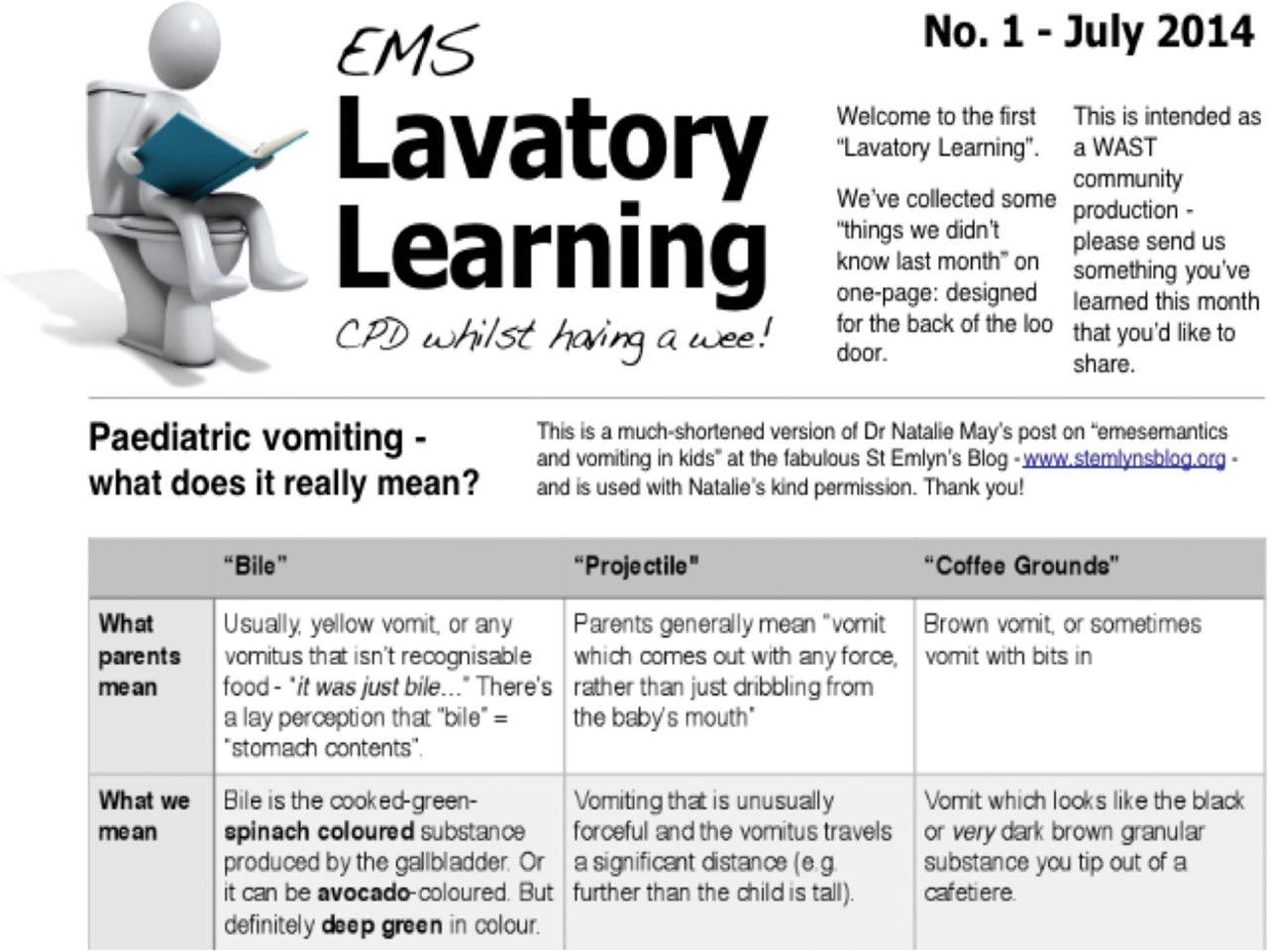
Little direct evidence can be found that individuals have distinct learning styles (visual or auditory etc).4 However, having a perceived learning preference does occur. Social media has allowed a variety of pedagogical methodologies to flourish in response to this. None are particularly novel (the spoken word is not a new invention) but the blog, podcast and vodcast (a narrated presentation) have blossomed given the plethora of (free) platforms available with which to present information. In the specialties of emergency and critical care alone there were only two recognised blogs and one podcast in 2002. In 2013, this had risen to 141 blogs and 42 podcasts.5 There are different styles either dependant on the personality and experience of the presenter or the format by which the information is presented (podcasts may be individual narrating or involve conversations between two or more people). The on-demand nature of these resources means clinicians can access the information they require in their own time and at their own pace. Whether it be listening to a podcast on the way to work, reading a blog during a break or watching a video of a conference presentation during a teaching session, the option of asynchronous learning is now fully realised (Fig 1).

Example of online learning material. From Linda Dykes (@mmbangor). www.scribd.com/document/232298675/EMS-Lavatory-Learning-No-1-July-2014.
There have been concerns expressed that these unregulated and non-peer-reviewed processes promote poor practice and may be dangerous. These risks are present, but are no different than the current system of peer review, which often relies on the opinion of no more than one or two clinicians.6 Post-publication peer review, a method that is difficult to credibly implement in traditional academic medicine because of the time frames involved, happens in almost real time via social media. An example of this is the Skeptics Guide to Emergency Medicine (SGEM: http://thesgem.com/the-sgem-hot-off-the-press/) run by Dr Ken Milne. The SGEM hot-of the-press process is an amazing example of how digital platforms can influence dissemination of research (Box 1).
SGEM hot off the press process
Ultimately, key articles of relevance to particular specialties spread rapidly because of the connectivity of the individuals involved. These organic communities of practice have been instrumental in the success of social media.
Immersion in communities of practice (connectivity)
Free open access medical education (FOAM)7 is an international movement that has brought together people from many backgrounds and specialties. It describes the production of educational materials in a variety of forms that are openly accessible. The concept of FOAM was defined in a pub (much like all great innovations) although there are earlier examples of small networks of individuals sharing educational content with wider communities. Dr Mike Cadogan coined the term during an international emergency medicine conference. It has come to represent a focus point for critical care and emergency medicine communities in particular. The term encompassing not just the materials produced but the bringing together of enthusiasts who design and digest them. It has developed into a digital community of practice as demonstrated by examination of the hashtag #FOAMed.8 Communities of practice were defined by Wegner9 as ‘groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly’. A key construct is that the learning is not necessarily intentional.
FOAM, along with patient-derived digital communities such as #chroniclife, are social movements almost entirely derived within social media yet have all the attributes of a community of practice, with the potential benefits they confer on professional and patient outcomes. These communities of practice may rapidly develop into social movements. Kate Granger is a doctor who passed away in 2016 having been diagnosed with a rare form of cancer. She was responsible for the #hellomynameis movement that began with her encapsulation of how frustrating it is when healthcare staff don’t introduce themselves. Her campaign, which started on Twitter and has had over 1,500 million impressions and 80,000 contributors, continues to spread throughout the world (Fig 2).10
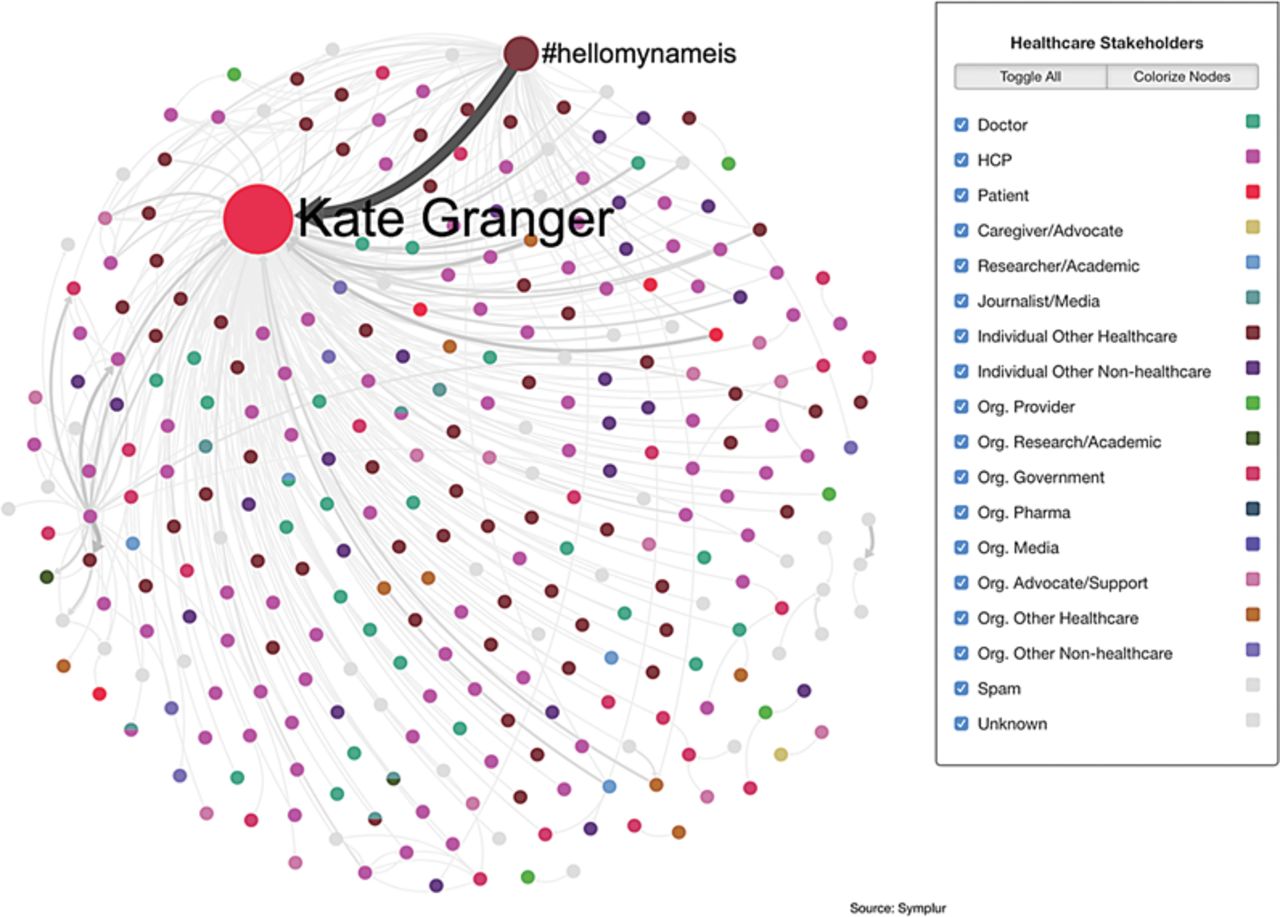
#Hellomynameis participants. From Symplur Signals.
Amelioration of the knowledge translation gap (scalability)
The combination of user-controlled education, directly applicable to learning needs, with the connectivity that social media allows the spread of knowledge translation at scale. Blogs, podcasts and videos can be produced in a fraction of the time that journal articles and letters of correspondence can be published. As the now retired Dr Joe Lex famously quoted:11If you want to know how we practised medicine five years ago, read a textbook.
If you want to know how we practised medicine two years ago, read a journal.
If you want to know how we practise medicine now, go to a (good) conference.
If you want to know how we will practise medicine in the future, listen in the hallways and use FOAM.
Social media has a crucial role to play in the transfer of evidence. Three new types of scholar are beginning to emerge:
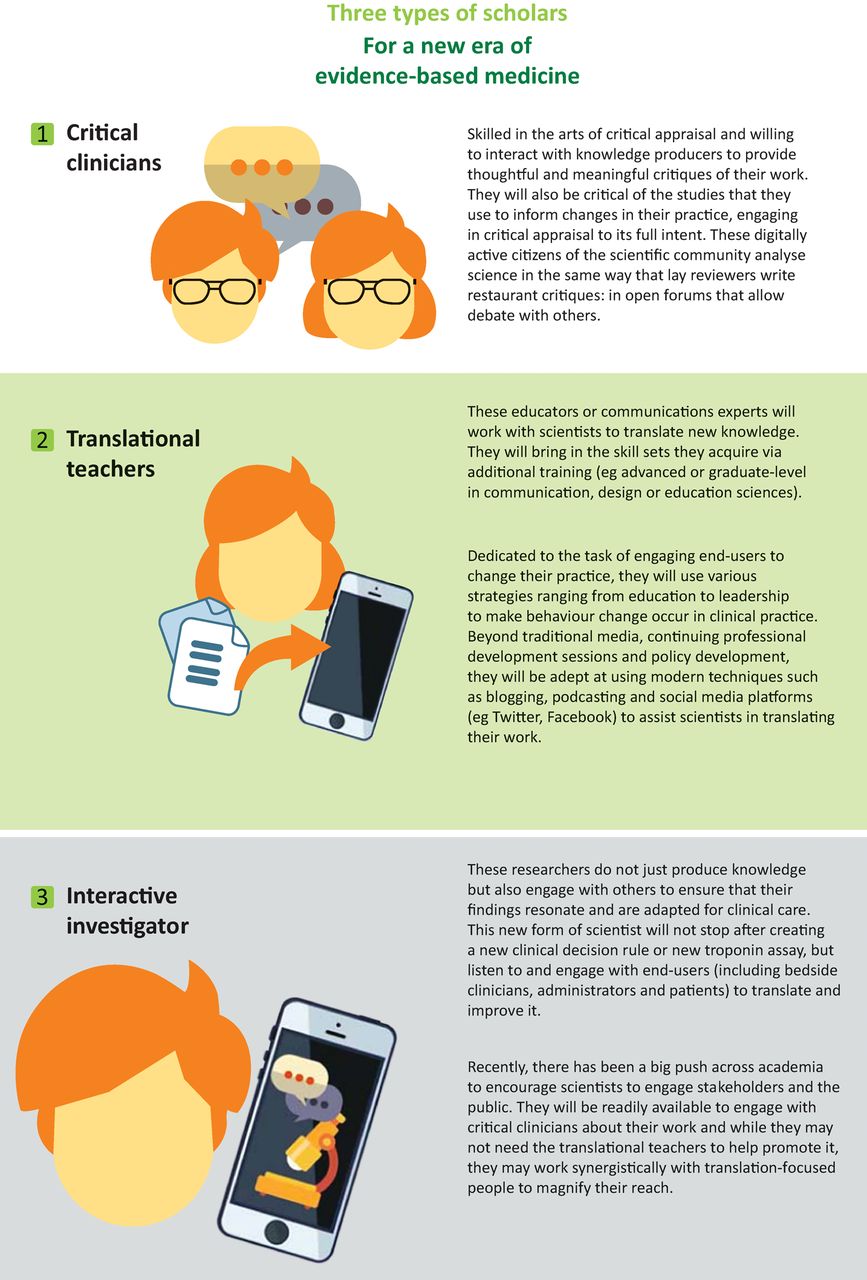
Three new types of digital scholar. Original concept from Chan et al.10
Social media has the ability to make research and policy applicable and relevant to an audience far wider than has ever been possible. For both professionals and patients there now exists the unrivalled opportunity to engage and inform. It is not without risk as the boundaries of individual professionalism often become strained when communication occurs via a digital medium rather than direct contact. Many fear social media could well become synonymous with anti-social media if professional values are not upheld online, as well as offline. However, the greatest challenge facing healthcare's interaction with social media is fear of the unknown. Hospital trusts still continue to block YouTube, Google and other similar sites with absolutely no evidence they do harm. The absolute numbers are difficult to quantify but conditions such as ‘At no time should social media sites be accessed from trust equipment (whether at work or outside of work)’ do exist.13 The poor behaviour of a few individuals is holding back whole swathes of the healthcare workers who, if allowed to, could network and access information in a way local hospital organisations would not be able to keep up with.
Conclusions
The applicability, connectivity and scalability of information available via social media cannot be ignored by those with leadership roles involving digital health. Social media should never be mandated, but neither should it be suppressed. The ability to create new collaborations and novel educational opportunities, for both patients and professionals, should be facilitated not frowned upon.
Conflicts of interest
The author has no conflicts of interest to declare.
Damian Roland tweets under the moniker @damian_roland
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
{kind=link}