
ABSTRACT
Despite numerous national campaigns, frailty remains under-recognised in the hospital setting. We performed a survey of hospital-based clinicians across the UK to identify barriers to the identification and best practice management of frailty in hospital. A total of 402 clinicians were surveyed across a range of grades, specialties and hospitals. Responses highlighted variable awareness and personal understanding of frailty, particularly among junior doctors and clinicians in non-medical specialties. Although 74% of responders agreed frailty assessments should be undertaken for all older people admitted to hospital, only 36% felt this was currently feasible with available resources. Free-text responses highlighted limited education, the perceived subjectivity of frailty assessments, scepticism as to their utility in the hospital setting, and deficiencies in service provision. This was the first survey of UK hospital clinicians regarding frailty assessments. Results highlight multiple areas for improvement and engagement.
Introduction
Frailty describes a state of reduced physiological reserve with age. This manifests as a vulnerability to sudden decline in functional status in the face of seemingly minor stressors, for example a low-grade infection or recent change in medications.1 This results in a propensity to require urgent health services, often resulting in hospitalisation with longer than average length of stay.2–4 Comprehensive geriatric assessment (CGA) remains the gold standard method for identification and management of frailty.5 A holistic, multidisciplinary intervention, CGA has been shown to improve patients’ chances of being discharged to their own home, reduce length of stay and prevent complications in hospital.6,7
Frailty assessments both in the inpatient and outpatient hospital setting are becoming increasingly common. The British Geriatrics Society (BGS) recommends that ‘all encounters between health and social care staff and older people in community and outpatient settings should include an assessment for frailty’.5 Specifically for older people with urgent or emergency care needs, the multi-agency endorsed Silver Book recommends ‘the presence of one or more frailty syndrome (falls, immobility, delirium, dementia, polypharmacy, incontinence, end of life care) should trigger a more detailed comprehensive geriatric assessment’.8 This essentially translates into a screening approach at the hospital front door.
Despite numerous national campaigns, frailty remains under-recognised in the hospital setting.9 There are also huge regional variations in the delivery of care for older people with frailty presenting to hospital, as highlighted by the 2016 NHS Benchmarking report.10
Identifying the underlying factors to explain these deficiencies could help target future strategies to promote best practice. To investigate this further, we performed a survey of hospital clinicians across the UK.
Methods
Survey development
The survey was developed iteratively by a multidisciplinary collaborative working group. Questions were constructed based on the clinical phenotype of frailty. Domains included personal understanding of frailty, identification of frailty, assessments for frailty, management of frailty and education. Statements requiring agree/disagree/not sure responses were chosen, and additional free-text comments were included to allow a broader discussion of viewpoints.11 A pilot paper survey was performed, with alterations made as per feedback received. All completed surveys remained anonymous, with no request for personal identifiers. Ethical approval was not required.
Sampling method
The survey was distributed to hospital-based clinicians between April and September 2016 in two stages. Initially, paper surveys were distributed at local events across various sites in north-west England (primarily teaching/departmental meetings). Following this, replicate online surveys were created (SurveyMonkey® UK) and electronic links were emailed via the British Geriatric Society regional secretaries, the Royal College of Physicians Future Hospital Programme site leads and local trust mailing lists available to the authors. Regional distributers were asked to disseminate the online surveys to all clinicians working at an NHS acute hospital site.
Analysis
Quantitative data were managed and analysed using IBM SPSS Statistics software. By virtue of being a survey design, only descriptive statistical methods were used. All authors undertook qualitative analysis of free-text comments. Retrospective thematic coding was used to categorise responses manually by each author independently, then together as a group to finalise common themes.12
Results
Responder characteristics
In total, 402 clinicians were surveyed across a broad range of grades, specialties and UK hospital sites (see Table 1 for responder characteristics). Junior doctors were defined as any clinican working below the level of specialty trainee.
Characteristics of survey responders
A summary of survey responses is shown in Table 2.
Survey responses summary
Personal understanding of frailty
Statements 1a–1c received mixed responses. Of those who answered ‘not sure’ to statement 1a ‘I fully understand the meaning of the clinical term frailty’, only 35% (n=38) subsequently agreed with the statement ‘I am unsure what frailty means’ (38% disagreed). Free-text comments collected for statements 1a–1c suggested a number of responders felt their personal understanding of frailty sat somewhere in between these two statements.
Of the consultants surveyed, 60% (n=108) agreed with statement 1a, compared with 55% (n=42) of specialty trainees and 38% (n=36) of junior doctors.
Identification of frailty
Regarding statement 2b ‘I feel confident identifying frailty’, 64% (n=115) of consultants, 60% (n=46) of specialty trainees and 35% (n=34) of junior doctors agreed. Despite this, 71% (n=68) of junior doctors reported the presence/absence of frailty affected their clinical decision making.
Across the consultant body, 94% (n=29) in geriatric medicine agreed, compared with 71% (n=30) in acute medicine, 61% (n=11) in anaesthetics and 41% (n=7) in the surgical subspecialties.
Assessments for frailty
The majority of responders (74%, n=298) agreed with statement 3b ‘Frailty assessments should be undertaken for all older people admitted to hospital’; however, only 36% (n=144) agreed this was currently feasible. Only 38% (n=68) of consultants, 30% (n=23) of specialty trainees and 42% (n=41) of junior doctors agreed ‘it is currently feasible to assess all older people admitted to hospital for frailty’. Of note, this statement had a high number of ‘not sure’ responses.
Management of frailty
Despite 44% of all responders agreeing with statement 4a ‘all hospital inpatients identified as frail should be reviewed by a geriatrician’, only 12% felt this was feasible. This varied by hospital site, ranging from 0–26% (across sites with ≥10 responders).
Education
The majority of responders across all grades agreed more training on frailty was required: 61% (n=110) of consultants, 88% (n=68) of specialty trainees and 90% (n=86) of junior doctors.
Free-text comments analysis
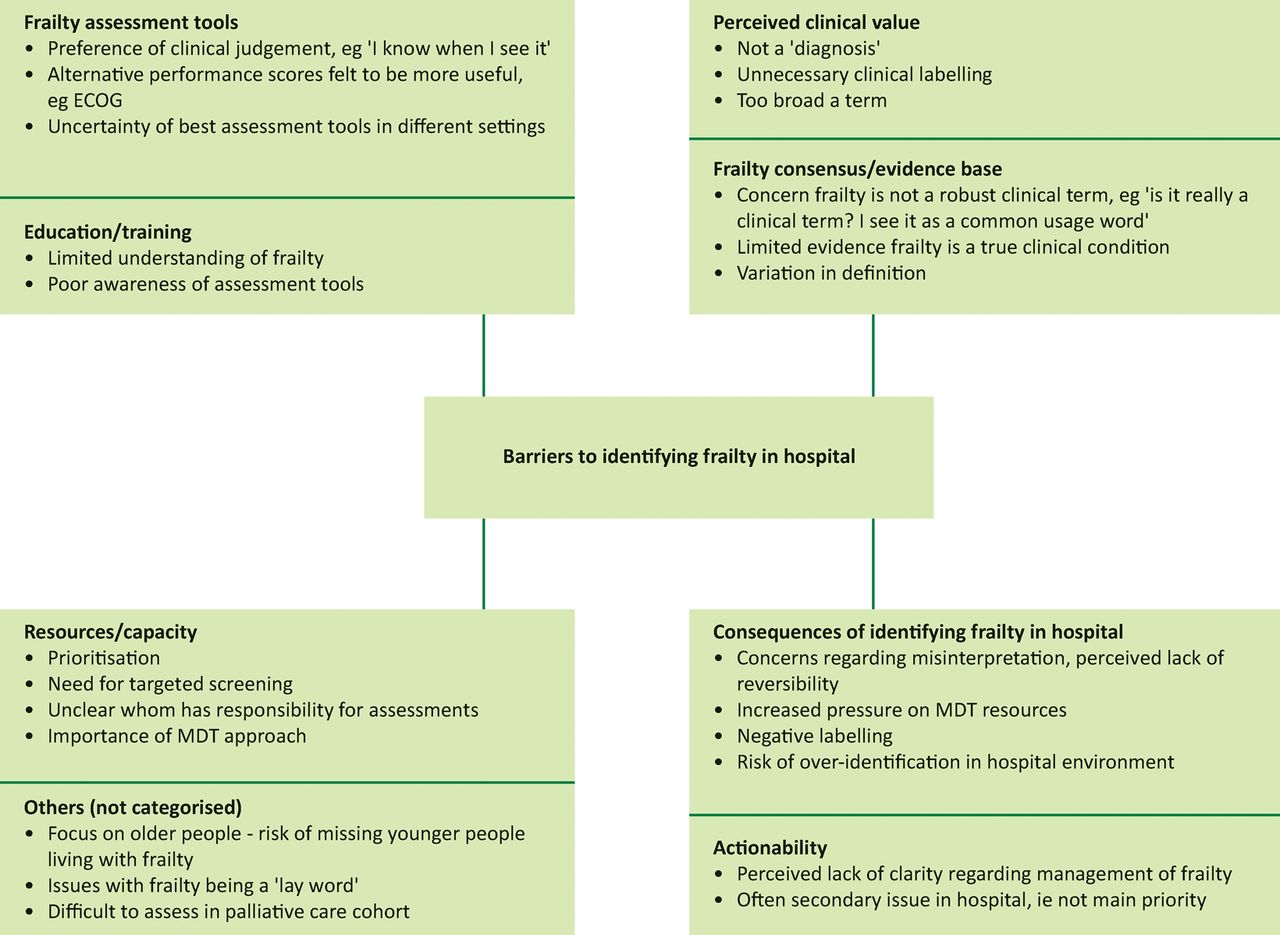
Fig 1 illustrates the main themes identified through review of free-text comments by the authors.
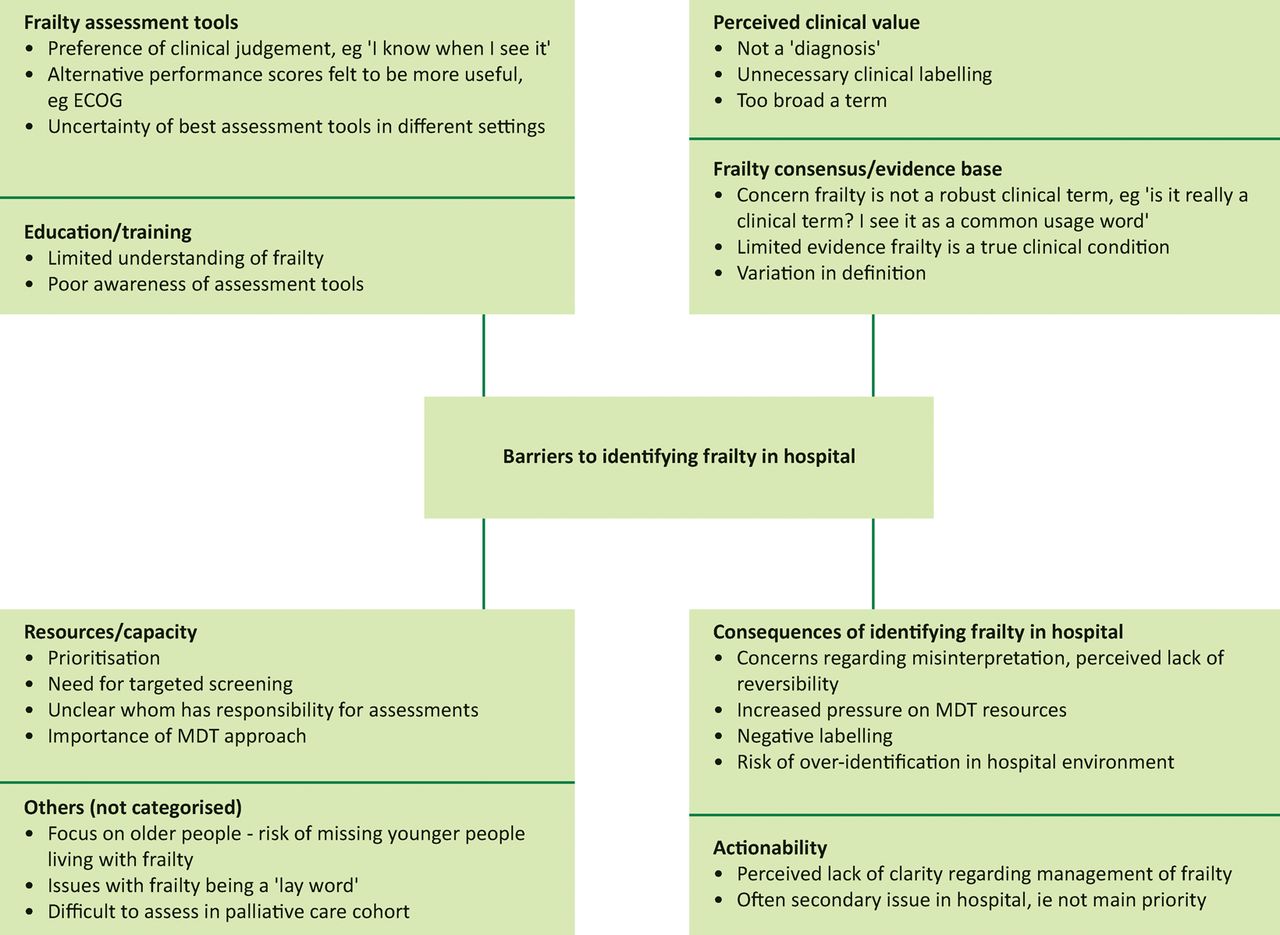
Thematic analysis of survey free-text comments regarding barriers to identifying frailty in hospital. ECOG = Eastern Cooperative Oncology Group; MDT = multidisciplinary team
A number of comments highlighted the concern that frailty lacked credibility as a recognised medical syndrome. For example, one reviewer commented ‘I think the term frailty should not be used in clinical practice as it can’t be defined’, and another ‘it is not a precise clinical condition’. A second strong theme that emerged from the comments was the value of identifying frailty through experience and perception, rather than formal tools. Many commented on the so-called ‘end of the bed’ assessment.
A number of responders cited issues surrounding service capacity and the perceived utility of frailty assessments in the hospital environment. For example, ‘We simply do not have the resources to do this’ and ‘Although it would be possible to assess every patient, it would require a large amount of educational and supervisory investment to ensure the assessment was meaningful’.
A lack of specialist inpatient geriatrician provision was also highlighted.
Discussion
This survey demonstrates that although significant progress has been made in improving identification and management of frailty in hospital, multiple barriers remain. Deficiencies in training and inadequate resources/clinical time highlighted in this survey are likely contributing to difficulties surrounding implementation of guidance incorporating frailty assessments into routine hospital clinical practice.
This survey suggests most clinicians rely on clinical judgement to identify frailty. Review of comments identified a tendency to use ‘end of the bed’ assessments. Less than a quarter of respondents use validated frailty assessment tools. This is concerning when important clinical decisions rest on the outcome of a subjective assessment, which can be misleading in hospital. Easy to use, validated frailty assessment tools (such as the CSHA Clinical Frailty Scale13) are now widely available.
An interesting and unexpected finding from the survey was the perception by some clinicians that frailty was a clinical syndrome with little foundation. This may be due to poor dissemination of evidence, deficiencies in training or a combination of both. However, this scepticism should not be dismissed. The difference between the robust criteria used to describe physical frailty in the research setting and operational definitions of frailty syndromes in usual clinical practice may have led to a weakening of perceived credibility. That said, the scientific case for frailty is largely accepted.
Clinical guidelines suggest all older patients admitted to hospital should be routinely assessed for frailty and, if identified as frail, undergo timely CGA. However, as demonstrated by this survey, for many hospitals this is simply unachievable with the current resource availability.
Frailty is traditionally seen as a condition within the domain of geriatric medicine; therefore, it was intriguing to note that an equal number of consultant geriatricians responded ‘agree’ and ‘disagree’ to the statement ‘all hospital inpatients identified as frail should be reviewed by a geriatrician’. Guidelines are clear in recommending CGA, but not whether this assessment specifically needs to involve a geriatrician. There is a national drive for hospitals to provide acute frailty services with some opting for nurse-led multidisciplinary team in-reach services and others being supported by consultant-led multidisciplinary teams.7,14 The best way to design these services remains an ongoing area of debate.15
This survey found a clear deficiency in understanding of frailty in the surgical subspecialties, a concern given the high number of patients with frailty presenting to these service (eg hip fracture cohorts).16 Hospitals integrating frailty pathways into standard workflows therefore need to be mindful of the need to remain inclusive across all areas of the hospital structure. This survey would support the viewpoint that frailty should be viewed as a cross-disciplinary issue, triggering a drive to upskill the entire workforce rather than introducing systems that simply trigger onward referral.
This survey was targeted at clinicians only. While frailty assessments can be performed by any trained member of the multidisciplinary team, practice and expected competencies vary widely. A focus on clinicians was therefore chosen in order to produce meaningful results with clear recommendations. Most responders to this survey agreed nursing and therapy staff, as well as clinicians, should be responsible for identifying frailty in hospital, highlighting the cross-disciplinary nature of these assessments. Future surveys should therefore be expanded to include the entire multidisciplinary team.
Limitations of results
Survey design
A true/false statement-based survey design was chosen to optimise clarity of responses. A well-known limitation of this method is the risk that none of the available statement options accurately represented the responder's true standpoint – as demonstrated in statements 1a–c. The phrase ‘identified as frail’ in question 4 is poor terminology. As a long-term condition, this should read ‘identified as living with frailty’.
Sampling method
A lack of access to national mailing lists limited distribution. Unfortunately, because of numerous survey links being ‘forwarded on’, we are unable to assess actual response rate. The impact of sampling/non-responder bias is therefore difficult to judge. Based on direct response rate from primary distributers, we estimate response rate to be 15–20%.
Responder mix
Most responses came from north-west England. However, the authors do not feel this significantly impacts on the generalisability of results, as the sample included a good mix of hospital sites, responder grades and specialties. The sample included an over-representation of clinicians working within geriatric medicine and specialty trainees. These responder groups tended to have a greater understanding of frailty and frailty assessments, thus results may be skewed.
Conclusions
This survey has highlighted a number of issues relevant to the care of older patients in hospital:
the perceived validity and utility of frailty as a clinical syndrome
the apparently limited awareness and uptake of frailty assessment tools
the apparently limited capacity within the hospital system for identifying and managing frailty.
These findings represent multiple target areas for improvement. Education is clearly deficient, so we would recommend frailty be given a stronger emphasis on the undergraduate curriculum to cement these principles early in medical education. This should be reinforced by workplace-based training, in particular the application of frailty assessments in clinical practice. Use of validated frailty assessment tools should be promoted in clinical environments, particularly those that care for high numbers of older patients. Finally, robust investment in front-line services for older people presenting to hospital is integral to support the provision of comprehensive care as standard.
Conflicts of interests
The authors have no conflicts of interest to declare.
Author contributions
Conception and survey development: JKT and RH
Data collection: all authors
Data analysis and write up: all authors.
Joanne Taylor tweets using the moniker @JoTaylorMCR1
Acknowledgements
The authors would like to thank John Dean, East Lancashire Hospitals NHS Trust, for advice and guidance regarding the development and distribution of surveys and Charlotte Kirk, Western Sussex Hospitals NHS Trust, for advice and assistance with survey distribution.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.