
ABSTRACT
Increasing demand and growing complexity of the delivery of healthcare is associated with worsening performance in safety, delivery, quality and affordability. Systems engineering (SE) is an established body of knowledge that is widely used outside healthcare in domains such as aerospace and communications. Healthcare represents a complex adaptive system (CAS) and a combination of ‘hard’ and ‘soft’ systems engineering techniques have been successfully combined and piloted in primary, community and secondary care improvement projects as part of an emergent programme for developing embedded NHS capability in healthcare systems engineering. The current barrier to wider adoption appears to be a gap in awareness, belief and capability but the mounting evidence from a growing number of healthcare systems engineering (HCSE) practitioners is that this capability chasm can be crossed.
Background
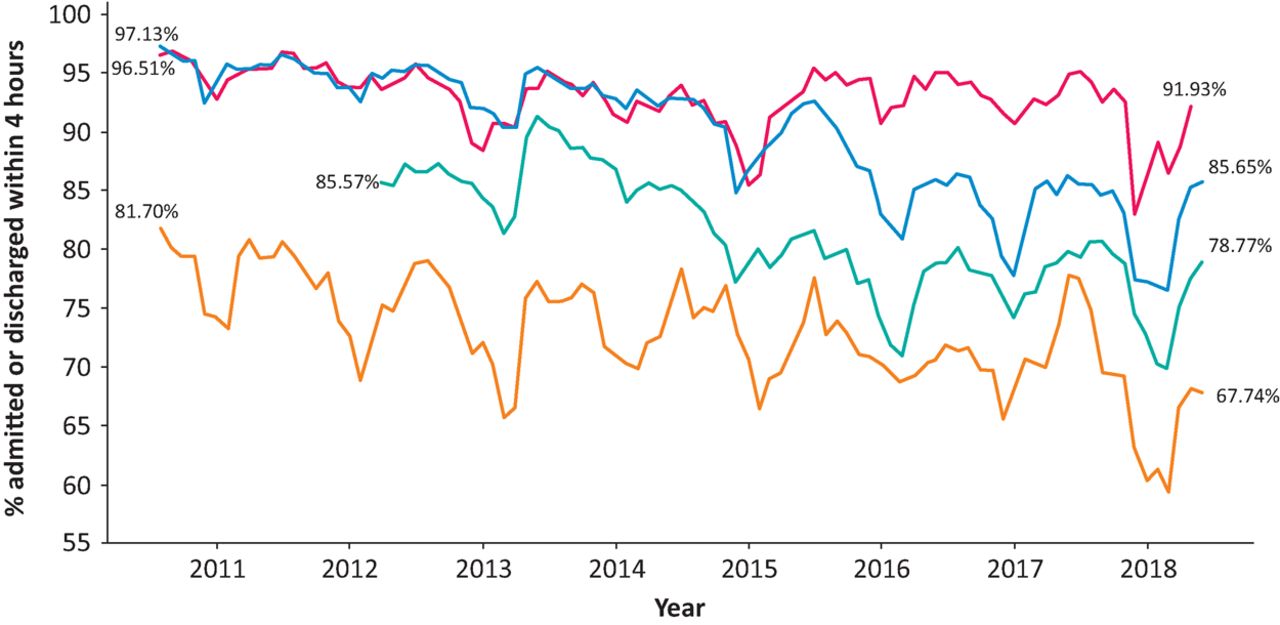
The global trends of increasing population, age, multiple long-term conditions, advancing knowledge, new technology and medical specialisation have combined to create an increasingly complicated system of healthcare provision and inexorably rising costs. At the same time, economic limits to growth in healthcare spending has created increasingly complex and chaotic system behaviour and progressively worsening whole system performance. In unscheduled care, the 4-hour target performance shows deterioration in both safety and quality, particularly during the winters (Fig 1).
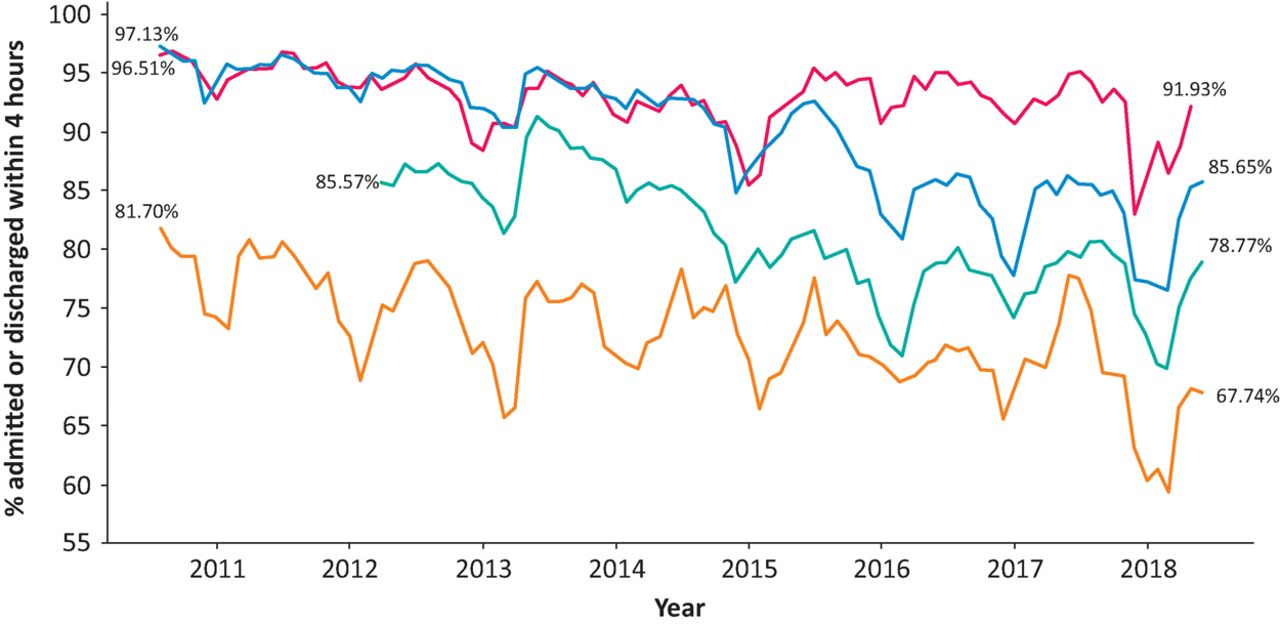
Time series chart of monthly UK A&E 4-hour target yield from 2010 to 2018. Red = Scotland; blue = England; teal = Wales; orange = Northern Ireland. A&E = accident and emergency
Source: https://public.tableau.com/profile/england.a.e.performance#!/
The NHS in the UK is a complicated network of patients, purchasers and providers that must continually evolve to meet emerging demands and shifting constraints. The objective evidence shows that our collective ability to do this is falling short of what is wanted, so a fresh perspective appears to be required.
Systems engineering
A system is commonly defined as ‘a collection of hardware, software, people, facilities, and procedures organized to accomplish some common objectives’ and the science of how to engineer systems emerged in the 1950s in the domain of defence and aerospace.1 This form of systems engineering (SE) is termed ‘hard’ and it underpins many things that we take for granted such as energy generation and distribution, transport and logistics, digital computers, mobile telephones and the Internet. SE is now a taught subject,1 has been codified into the international standard ISO 152882 and there are established training paths to certification and accreditation. However, despite the world-changing benefits of hard SE, the diffusion of this know-how into healthcare appears to be limited to the development of high technology medical products such as computed tomography (CT) and magnetic resonance imaging (MRI) scanners.
Limitations of the hard SE approach became apparent when they were applied in the ‘softer’ social sciences and the concept of ‘wicked problems’ emerged.3 This paralleled the development of a range of ‘soft’ systems improvement methods,4 but despite this encouraging start, these soft approaches have not enjoyed the same degree of success. The reasons for this are becoming clearer.
Complex adaptive systems
In the 1970s, there was a paradigm shift in our understanding of natural systems with the emergence of complexity science and chaos theory. Using the rapidly developing power of digital computers, it became feasible to simulate complicated passive systems, such as the weather, and to reliably predict how they will evolve over time ie weather forecasting.
Early computer simulations of active systems included models of ant colonies that behaved very realistically and ‘complex adaptive system’ (CAS) is now used to describe such a system. One unexpected finding was that complex, coordinated, goal-seeking behaviours can emerge naturally from a population of interacting agents who use a small set of simple rules; no predetermined plan or centralised coordination was required.5
Innovators who translated these principles into the healthcare context found that there was a wide spectrum of applicability, and that the traditional reductionist approach only works for a limited set of problems that tend to be at the ‘hard’ end of the SE spectrum.6
So, at the dawn of the new millennium, the scene was set for SE to be applied in health and social care, but significant cultural barriers remained:
awareness of the SE body of knowledge, ie both hard and soft SE
belief that a blend of hard and soft systems methods can work in healthcare, ie robust evidence
capability to diagnose, design and deliver significant and sustained improvements in healthcare.
Healthcare SE (HCSE)
In the period from April 2001 to April 2013, first the Modernisation Agency (MA) and later the NHS Institute for Innovation and Improvement were advocating the science of improvement. They were inspired by the newly formed Institute of Healthcare Improvement (IHI)7 which in turn was a spin-off of the total quality management (TQM) movement that emerged in the 1980s. A core tenet of these ambitious NHS programmes was to develop evidence-based methods and to embed improvement capability within NHS organisations. This work continues under the auspices of NHS Improvement.
The NHS employs around 1.3 million people, so it is inevitable that some will also have been exposed to formal SE methods. One of these is Dr Kate Silvester who trained as an ophthalmologist, then left the NHS to retrain as a manufacturing system engineer with Lucas and Airbus, and later rejoined the NHS as part of the MA. In 2009, Kate was commissioned by the Health Foundation to run in a 3-year project with Warwick and Sheffield NHS Trusts and successfully demonstrated the benefit of teaching manufacturing engineering methods to NHS staff.8 Another doctor-engineer is the author of this paper who trained as a computer systems engineer in the early 1980s, and later qualified as a doctor and followed a career in general and vascular surgery. In 1999, when I was appointed to a consultant post, I naturally applied these improvement-by-design methods to improving the clinical service that I inherited, with significant improvements in clinic flow, finish time and later a sustained 31% increase in clinic productivity.9,10
During this time, it became clear to both Dr Silvester and I that there was a gap in the current quality improvement (QI) offering; there was no foundation of a flow engineering science underpinning it.
One element of the HCSE approach is the diagnose-design-decide-deliver sequence which creates a bridge between the future purpose and the present problem. The first step is to accurately diagnose the reasons the current design is not fit-for-purpose and then to only redesign those parts that require it. Another element is to test the proposed designs using a range of simulation techniques to create a prognosis of the expected future performance and use that to inform the decision of which design to implement.
In 2014, we had the opportunity to work with Monklands Hospital in Lanarkshire to train and coach a small, embedded team of doctors, nurses, managers and data analysts in the principles and practice of improvement-by-design. The problem that NHS Scotland wanted us to address was the deteriorating accident and emergency (A&E) performance. The diagnostic step revealed a push-carveout design that reduced their resilience to demand variation and which generated unstable and unpredictable queues and delays. The proposed solution was a pooled-pull design that was validated using a controlled experiment in September 2014. Figure 2 shows a step change in January 2015 when the Monklands microsystem design team (MDT) implemented the new A&E flow process that they had designed and validated. Ongoing monitoring over the subsequent 4 years shows that the improvement has been sustained.
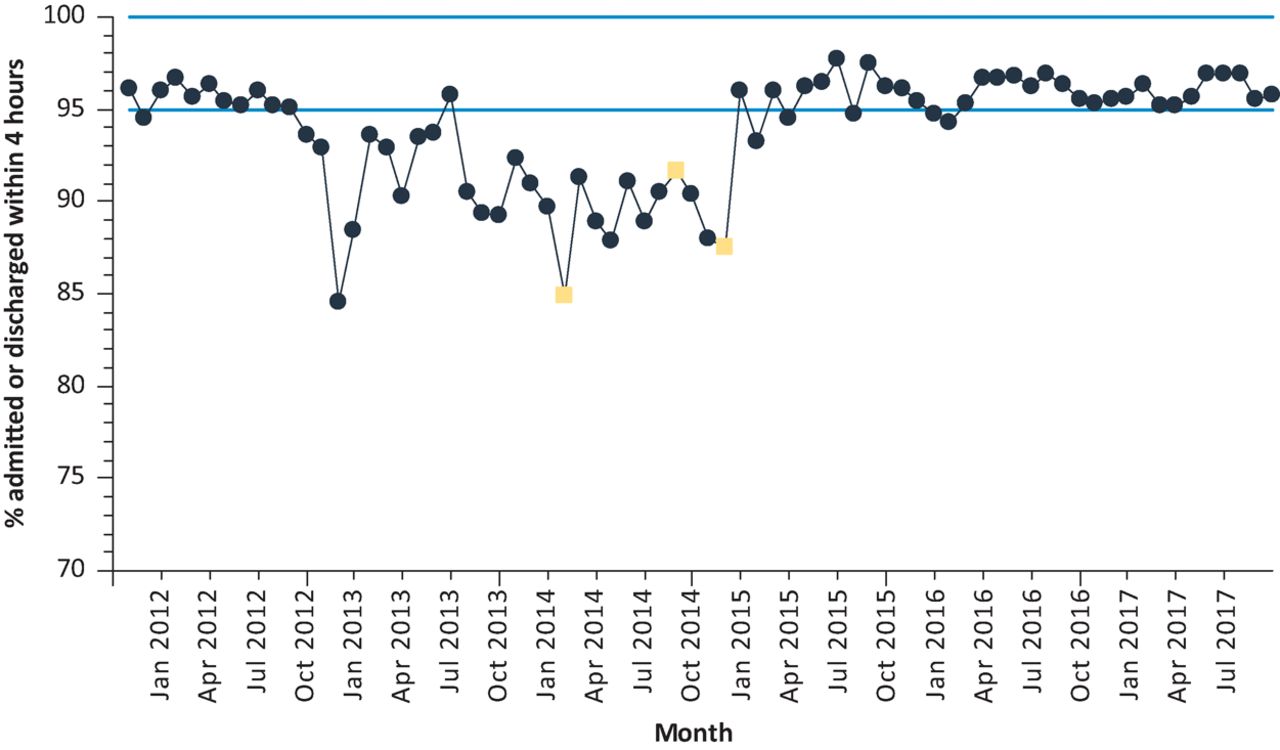
Time-series chart of the monthly A&E 4-hour target yield for Monklands Hospital from December 2011 to November 2017. The HCSE level 1 training for the embedded microsystem design team commenced in February 2014, the redesigned A&E process was piloted in September 2014 and was fully implemented in January 2015 (yellow boxes). Source: NHS Scotland. Blue lines = specified limits of required performance (95–100%) A&E = accident and emergency
Awareness of the potential of SE in healthcare has grown elsewhere because, despite the success of the IHI in promoting safety and QI science, there were still deep concerns about the health of the US healthcare system. In May 2014, the President’s Council of Advisors on Science and Technology (PCAST) prepared a report entitled Better Health Care and Lower Costs – Accelerating Improvement Through Systems Engineering, and one of the six recommendations was ‘train health professionals in new skills and approaches’.11 In the UK, the Royal Academy of Engineering organised a series of exploratory workshops, in collaboration with the Royal College of Physicians, to bring systems engineers and NHS staff together to explore the common ground, and the tangible output is the Engineering Better Care report that was published in August 2017.12
The future
The first chapter in any system engineering story is the needs analysis, and the need here is clear: an NHS that is capable of healing itself and keeping itself healthy.
With the benefit of hindsight, and the evidence already available, it is becoming clear that the NHS stands to benefit significantly from developing its own embedded capability in both hard and soft SE to complement its existing safety and QI skills. HCSE is an emerging discipline and there are currently no standard training programmes or accredited courses in the UK, nor any published plans to create any.
One recurring theme has become apparent: attempting to teach HCSE principles from a theoretical perspective did not work well because the language and concepts are too unfamiliar and too abstract. What worked much better was teaching SE pragmatically using real-world projects to provide the concrete, practical, hands-on learning opportunities.
An innovative blended-learning programme has emerged through the efforts of a small, but growing, informal community of improvement practitioners (CHIPs) who have seen the early results and who wanted to learn how to do it themselves. The HCSE programme augments existing operations management (OM) and QI training, is structured into levels based on competency and experience and includes the requirement to be willing and able to train and coach others (Table 1) – ie create a knowledge cascade that can support growth at scale and pace.
Sample of the HCSE core curriculum
To date, over 500 people have completed the online foundations course, over 100 have commenced the level 1 HCSE training which includes a requirement to publish at least one case study. There are currently HCSE teams active in England, Wales and Northern Ireland and the first wave of level 2 HCSE practitioners are about to ‘graduate’. This is a critical milestone because a required level 2 competency is to have trained and coached others through the level 1 programme. The level 1 training would fit well into a postgraduate vocational programme for anyone aspiring to have a management role. The level 2 training would fit a masters-level programme for anyone intending to lead improvement work focused on safety, flow, quality or productivity.
One recently published HCSE level 2 project delivered a significant reduction in length of stay for unscheduled emergency, elderly admissions as a result of a primary care-led early-assisted discharge design.13 Other published HCSE level 1 case studies include outpatients,14 diagnostics15 and chemotherapy.16
So, perhaps one day we will have a well-defined set of HCSE competencies, accredited training, individual practitioner certification, a recognised career path and possibly even chartered healthcare systems engineers working in a self-improving NHS.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.