
ABSTRACT
Handover has long been identified as a potential source for error that can have direct consequences for patient care. The current weekend handover system at University College Hospital, London, involved a verbal handover meeting with a variety of methods used to collate information. A new handover system was introduced that involved the pre-population of a spreadsheet before attending the handover meeting. Doctors involved in the handover process were canvassed for opinion before and after the introduction of the new system, and logistical data were collected. The new system reduced the amount of time spent preparing for, and delivering, handover, and was deemed to be safer and to improve adherence to the Royal College of Physicians’ guidelines for handover, including specification of level of doctor to perform handover and prioritisation of handover.
Introduction
Effective, safe and comprehensive handover is an essential aspect of providing patient care. International research has identified poor handover as a major contributing factor to potential harm. Handover guidance has been issued by the Royal College of Physicians (RCP) and the Royal College of Surgeons (RCS), and by the UK General Medical Council in an attempt to reduce risk.1–6
The change to doctors’ working hours with the adaptation of 7-day working has resulted in more frequent handover episodes between medical colleagues. The weekend handover is often the most complex – frequently with complete changeover between medical staff caring for patients. This results in significant potential for human error and, as a consequence, negative impacts on patients.7
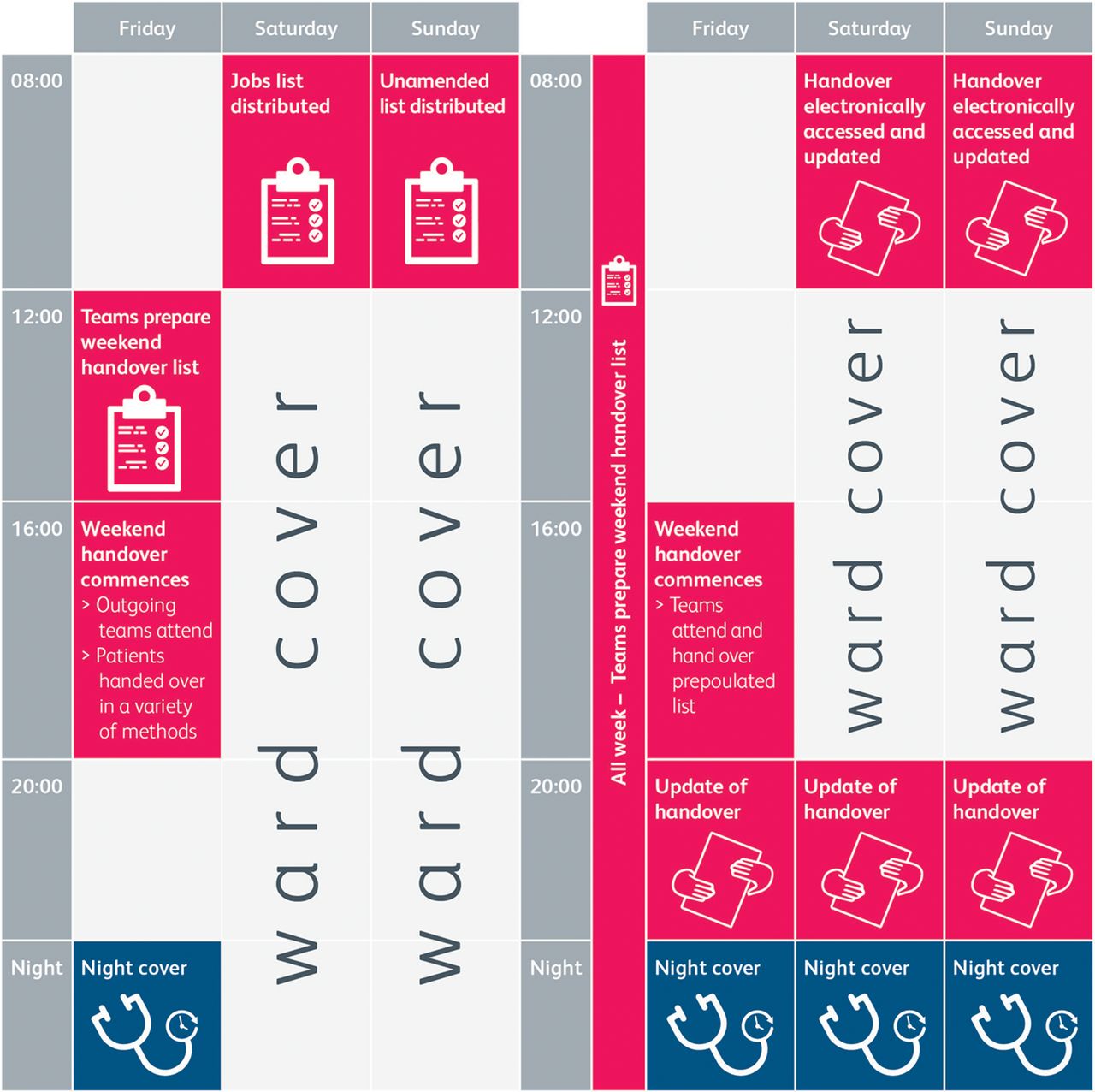
Although overarching principles of handover are the same nationwide, each hospital varies in size, specialties, team members and resources. As a result, handover delivery continues to be variable.7–13 University College Hospital, London, is a large, quaternary-referral teaching hospital with over 650 inpatient beds at its main site. Specialties include a respiratory medicine team, three medicine for the elderly teams, four gastrointestinal teams and a clinical pharmacology team. The weekend medical cover was provided on a rota basis with two first-year postgraduates (FY1s), a second-, third- or fourth-year postgraduate (FY2/CMT) and a fifth-year postgraduate or higher (ST3+) from these specialties (Fig 1). Handover for the weekend system comprised a Friday afternoon meeting, where outgoing junior doctors provided paper ward lists for all of their patients and outlined those who would require intervention over the weekend. Tasks to be completed over the weekend were then consolidated onto a spreadsheet by the incoming team, paper copies of which were distributed (Fig 2).
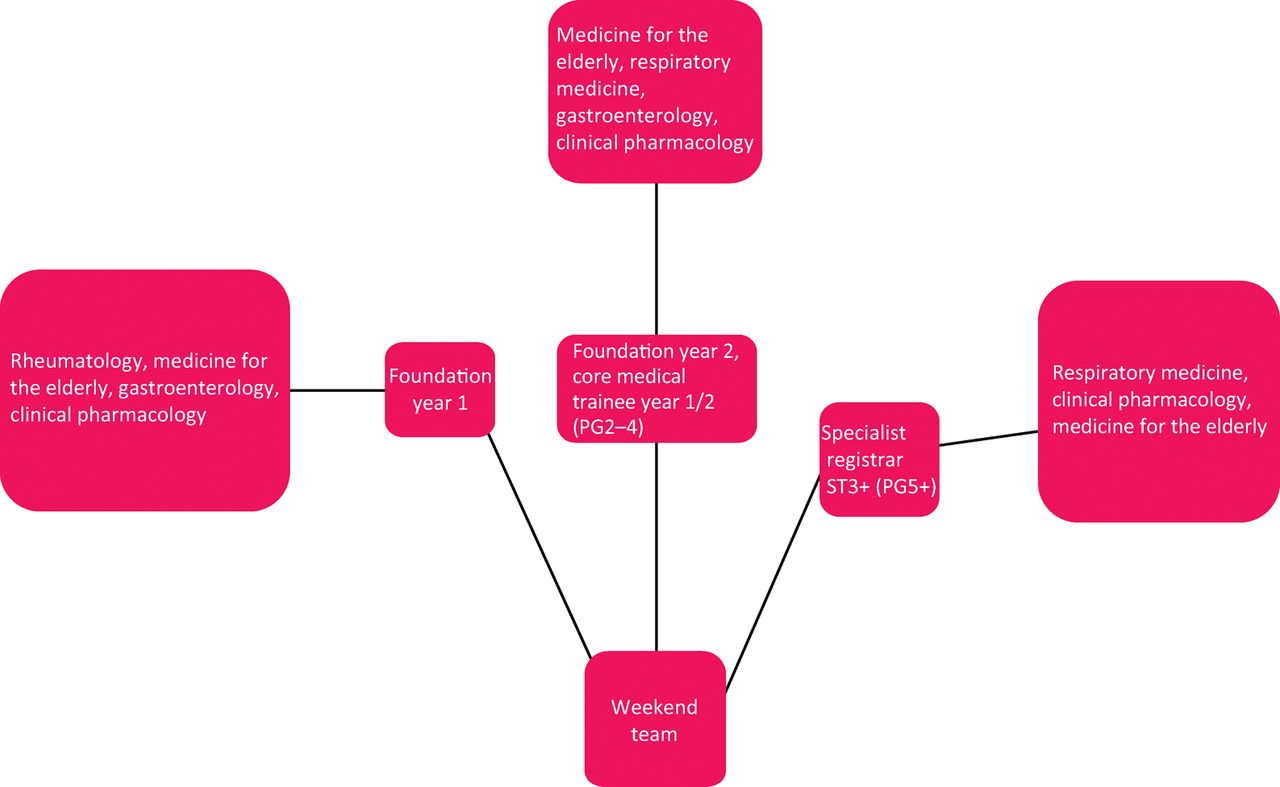
Overview of weekend team make-up.
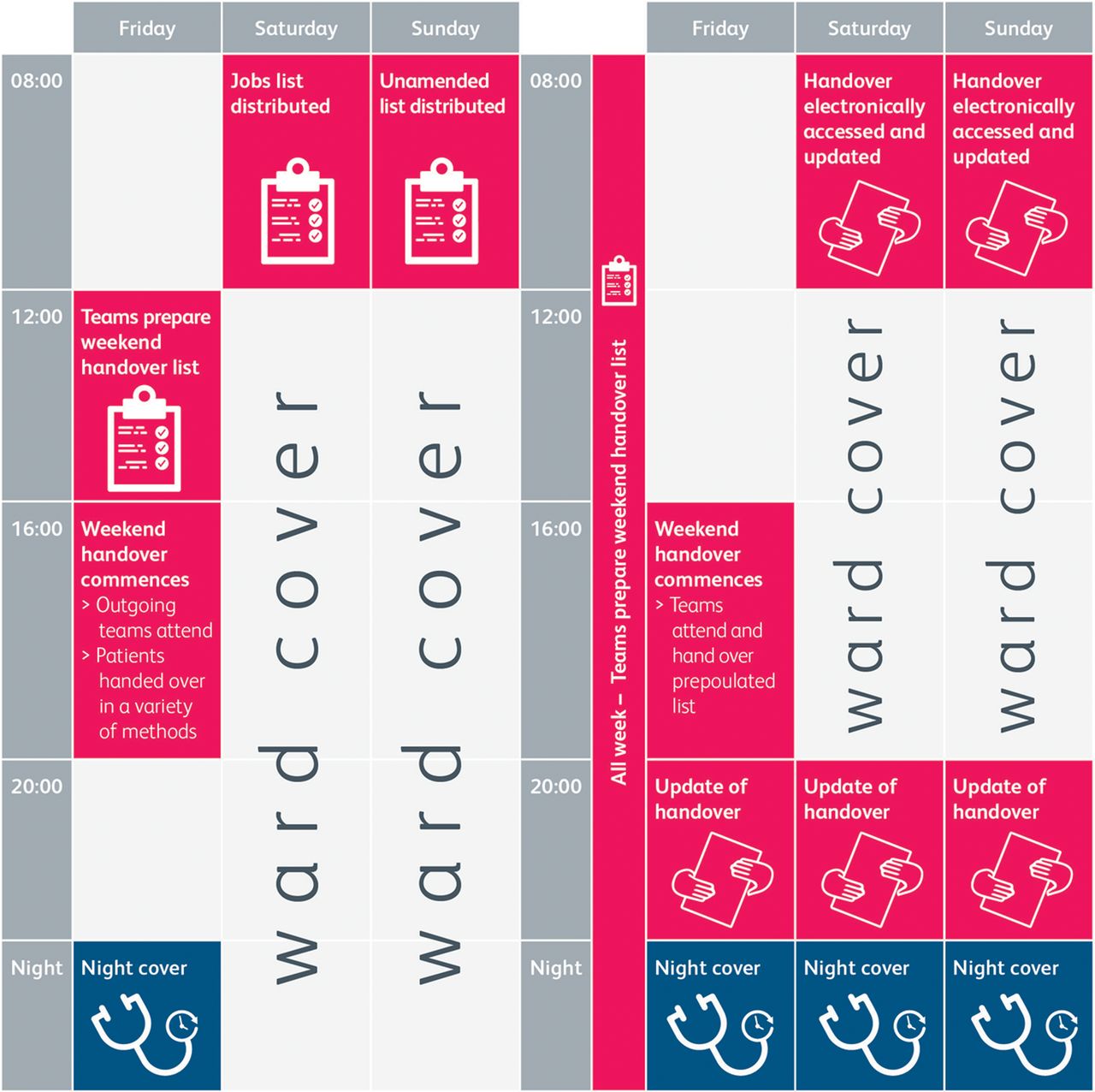
Process map of handover before and after introduction of new system. aThis change in process results in handover taking less time complete.
The system required improvement. The nature of the meeting was unstructured, protracted and time inefficient. Preliminary research showed that the time spent attending handover meetings was often inappropriately long and unproductive, with teams queuing to hand over and often staying past the end of their shifts. The lack of a structured handover form provided great interdoctor variability in terms of the data recorded. Further preliminary data showed that this was often noncompliant with the guidelines suggested by the RCP (Table 1).
SMART aims for handover development
Comparison of compliance with Royal College of Physicians’ guidelines before and after introduction of new handover system
Once the consolidated handover had been produced and distributed, there was no way to update the spreadsheet, preventing team members from accessing a ‘live’ version to add new tasks and to mark others as completed, or to feedback to the weekday team returning after the weekend.
Aims
We developed an electronic handover pro forma that could be accessed by multiple doctors simultaneously, allowing standardised pre-population before attending the handover meeting. We wanted to have 100% compliance not only with the new electronic system from all outgoing teams to standardise the handover process, but also with the guidelines set out by the RCP. Using the new system, we aimed to reduce the time spent both preparing and delivering handover (Box 1).
Methodology
Questionnaires were issued to all 23 doctors working on the general medicine weekend ward cover rota. Data collected included opinion on importance of handover, current method of handover, time spent preparing handover, time delivering handover, number of patients handed over, prioritisation of tasks, identification of level of doctor to perform task, and opinions on the safety of the handover system.
The electronic system was created by a cohort of doctors, which included a medical consultant, medical registrars, core medical trainees and foundation doctors. The system was created using Microsoft Excel and was saved on a shared drive on the hospital network, to which only named doctors had access. The file was password protected. A new file was created from an existing protected template each week.
After data collection, the new electronic system was introduced. Three months after the initial introduction, the same cohort of doctors then recompleted the same questionnaire.
After the initial introduction of handover, we optimised the electronic handover template over a 2-month period. Changes orientated around making mandatory data entry fields and ensured that all necessary information was correctly recorded. Several technical issues with regards to the joint sharing and saving of the spreadsheet were identified and addressed.
A ‘how to’ guide was produced for doctors who were new to the system. This orientated particularly around the use of Microsoft Excel, how to create a new handover file and how to complete it. We also provided advice on filtering the form and printing.
Results
After the introduction of the new electronic system, doctors completed the same questionnaire as previously. Twenty-three questionnaires were returned, representing all the foundation doctors and core medical trainees during one medical rotation. The results are outlined below.
Compliance with Royal College of Physicians’ guidelines
The new handover system had 100% compliance with the guidelines issued by the RCP.
Importance of handover
After the introduction of the new handover system, the importance of the handover remained relatively unchanged. Most doctors felt that handover was very important (56.5% and 52%, foundation doctors and core medical trainees, respectively) or important (39.1% and 47%%, foundation doctors and core medical trainees, respectively). Before introduction, 4% of doctors felt handover was somewhat important.
Method of handover
All doctors completed the electronic spreadsheet and attending the handover. Before the introduction of the new system, a variety of methods had been used, including formal handover (18.9%), verbal handover (45.9%), handwritten handover (21.2%) or electronic handover (21.6%).
Time preparing for handover
The introduction of the electronic handover reduced the amount of time spend preparing for handover. Before the introduction of the new system, the mean time spent preparing was 24 min. After the introduction of the new system, this had reduced to 18 min; a reduction of ∼6 min or 25%.
Time spent in handover
A similar reduction in time was seen with time spent in handover. Before the introduction of the electronic system, the mean time spent handing over was 22.5 min, compared with 12.4 min after the introduction. This resulted in a reduction of ∼11 minutes or 45%.
Percentage of patients handed over
The introduction of the new system also saw a statistically significant reduction in the number of patients handed over. Before the introduction of the new system, a mean of 58.7 patients were handed over, which reduced to 46.5 after the new system was introduced; a reduction of 12.2 patients or 21%.
Prioritisation of handover
Before the introduction of the new handover system, myriad techniques were used to highlight the importance of jobs, with 17.4% never identifying importance, 43.5% of patients verbally handed over, 13% writing the importance, and 30.4% both writing and verbally communicating importance. This changed to 0%, 0%, 4.3% and 95.7%, respectively.
Identifying roles for handover
Identification of the doctor required to perform the job in the handover was present in 82% of patients before the introduction of the new handover, and increased to 91% of patients after the introduction.
Safety
Before the introduction of the new system, 65.2% of doctors thought that the handover process was safe, which increased to 100% after the introduction.
Discussion and limitations
The methods, practices and culture of handover varies widely throughout both the UK and internationally, with a variety of different methods used, including verbal,8 written9,10 and electronic systems7,11,14–16. After appraising the literature for the types of system previously introduced, we adopted a new electronic system. This aimed to address the unstructured nature of weekend handover and effectively produced a time-effective solution, which should translate into improved efficiency, as shown by the reduction in time spent creating and delivering handover. We hope that this will have future ramifications for medical staff, and help to alter the culture within teams with regards to handover.
Lessons learned
The introduction of a new electronic system allowed more complete and accurate data recording for handover, which was easily accessible from a range of sites around the hospital simultaneously, resulting in comprehensive data being available quickly. The introduction of the new system was received positively by the current cohort of doctors and improved their overall sense of safety with regards to handover. By highlighting handover as an issue, we were also able to educate doctors about what issues needed handing over; we felt that this helped reduce the total number of jobs handed over.
The reduction in time of handover also helped junior doctors comply with the European Working Time Directive by allowing them to finish their shifts in a timely fashion.
Future aims for the project include integration of the system into junior doctor induction, ongoing assessment of correct usage of the system, along with adaptations as needed.
Limitations
Future work with regards to the development of handover orientate around education and technological. With regards to education, the importance of handover and how to practically deliver a handover needs to be instilled in all doctors from a junior level upwards. This study highlighted fundamental flaws within the process and reasoning behind handover by junior doctors, and we aim to address this in future studies. Ideally, the system would also undergo further changes to allow an even more user-friendly interface, with ‘pop-up’ box entries to overcome technological issues.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.