
ABSTRACT
An evaluation was performed to assess efficacy and resource utilisation of an elective inpatient alcohol detoxification service at a large inner-city teaching hospital. Abstinence rates at 3, 6 and 12 months post-detoxification were 68.1, 44.7 and 36.2%, respectively. Relapse was associated with referrals from acute hospital services, previous detoxifications, longer time between referral and admission for detoxification, presence of alcohol in the blood on the day of admission and requirement for benzodiazepines during withdrawal. The service operates within the national 18-week referral target and runs at a cost substantially lower than that of residential alcohol detoxification facilities but with similar sobriety rates.
We demonstrate that elective detoxification with specialist follow-up provides an effective service both in terms of patient outcomes and resource use. Further investment in these services at both local and national level should be considered.
Introduction
In 2012, costs in the UK associated with alcohol-related health disorders, crime, loss of workplace productivity and domestic or familial problems were estimated at £21 billion.1 Societal harm associated with alcohol use is substantial.1,2 Despite the generalised decrease in alcohol consumption,3 the percentage of the population still drinking in the ‘increased risk’, ‘dependent drinking’ and ‘high risk drinking’ groups remains significant.4 In addition, the number of deaths related to alcohol use is increasing5 and when compared with the relative decline in other health care sectors, mortality6 and cost4 related to liver cirrhosis is increasing. Improved management of alcohol dependence may help to reduce this societal burden.
Patients presenting to hospital with alcohol withdrawal are often managed by an acute non-elective admission. We have previously demonstrated that an alternative approach of admission avoidance for unplanned alcohol detoxification accompanied by rapid access outpatient assessment with regular support and education and subsequent elective admission for detoxification results both in reduced length of the detoxification stay and less frequent subsequent alcohol-related readmissions.7
The West Midlands Poisons Unit (WMPU) is based within Sandwell and West Birmingham Hospitals NHS Trust (SWBH) and provides an elective alcohol detoxification service, aimed particularly at patients committed to sobriety but who are deemed unsuitable for community detoxification, such as those with no social support, those with significant co-morbidities and/or a history of alcohol withdrawal seizures. The protocol combines pre- and post-detoxification outpatient assessment and support with elective inpatient detoxification using symptom-triggered benzodiazepine dosing. It has previously been shown that this approach is well tolerated and leads to decreased benzodiazepine requirements and shorter length of stay when compared to fixed dose benzodiazepine regimens.8–10 The impact of medical outpatient management both pre- and post-alcohol detoxification is less well characterised, though there is evidence that engagement with outpatient services following detoxification from substance abuse in general decreases the likelihood of relapse in the following year.11 An evaluation of abstinence rates at 1 year, resource utilisation and service performance was conducted, both to assess efficacy of the service and to identify potential areas for improvement.
Methods
Patient inclusion and baseline data collection
This was a retrospective review of case notes for patients who underwent elective inpatient alcohol detoxification under the care of the WMPU clinical toxicology team between 01 July 2014 and the 01 November 2015. The review was registered as an audit (registration number: SG295) with the SWBH clinical effectiveness team who facilitated access to medical records. Data retrieved included basic demographic details, referral route, alcohol and smoking history, compliance with appointment attendance prior to and following admission and documented history of previous alcohol detoxifications.
Primary outcome – service efficacy
As a proxy measure of abstinence and ‘successful’ detoxification, clinic attendance, admission to acute medical units and presentations to the emergency department relating to alcohol withdrawal or intoxication were investigated for 1 year following elective admission. Entries to medical records during outpatient follow-up documenting recurrence of persistent drinking or admissions relating to intoxication or withdrawal symptoms were regarded as a relapse. In the absence of alcohol-related admission and where follow-up with declaration of on-going abstinence was available, patients were regarded as abstinent. Abstinence rates were determined at 3, 6 and 12 months after inpatient elective detoxification.
Secondary outcomes – service performance and resource use
Time from referral to first outpatient appointment and detoxification was recorded and the number of pre-detoxification appointments (new patient then follow-ups) were determined per patient. Length of stay of admissions was determined. The number of outpatient follow-up appointments offered post-detoxification and the time following detoxification to the first outpatient review was recorded. Finally, clinic attendance rate was also investigated, both pre- and post-detoxification.
Data analysis
Analysis was performed using GraphPad Prism version 7.00 for Windows. Data were assessed for Gaussian distribution using D'Agostino-Pearson tests. Where data were normally distributed, unpaired two-way parametric t-tests were performed and means ±standard deviation (SD) reported. Where data were not normally distributed Mann-Whitney two-way non-parametric t-tests were performed and medians (inter-quartile range (IQR)) reported. Correlations (Pearson's r) of factors that were significantly different between the relapse and abstinent groups and the number of days abstinent were calculated to examine the significance of any relationship. Logistic binary regression analysis explored the respective contribution of the latter group differential factors on the primary outcome of achieved abstinence at 1 year.
Results
Patient demographics
Data from 57 patients were collected. Ten patients were excluded, five due to incomplete follow-up and five due to self-discharge or incomplete detoxification during the inpatient stay. Forty-seven patients were included in all subsequent analyses (male, n=31; female, n=16; mean age, 48.0±10.1 years). Most patients were white British (78.7%; the remainder were 2.1% white Irish, 2.1% white Polish, 12.8% British Asian, 4.3% British African-Caribbean).
The median number of alcohol units consumed daily based on initial history was 26.0 (IQR 19.0–38.8); 84% of the patients were also cigarette smokers. Eighteen patients (38%) had undergone previous detoxifications. Of these, 61% had undergone previous detoxification at the WMPU.
Service efficacy
Following discharge, 68.1% (n=32), 44.7% (n=21) and 36.2% (n=17) of the 47 patients remained abstinent at 3, 6 and 12 months, respectively (Fig 1). At 12 months, age and sex distribution in the relapsed (n=30) and abstinent group (n=17) did not differ significantly. Discovery of relapse in 30 patients was by self-declaration or intoxication at outpatient appointment (46.7%), acute medical admission (26.7%) or emergency department attendance (26.7%). Fifty-six per cent of patients in the relapse group had undergone previous detoxifications, compared to only 26% of the abstinent group. In addition, the relapse group had undergone a significantly greater number of previous detoxifications per patient than the abstinent group (p<0.05; Fig 2). In the relapse group the median number of days abstinent was 80.5 (IQR 36.5–127.0); however, no association was observed between number of previous detoxifications and days abstinent (r=-0.27; p>0.05) and no significant predictive value of number of previous detoxifications on ultimate abstinence at 1 year was demonstrated (supplementary material S1).

Relapse rate. Percentage of patients that remained abstinent and relapsed at 3 (68.1%; n=32), 6 (44.7%; n=21) and 12 months (36.2%; n=17).
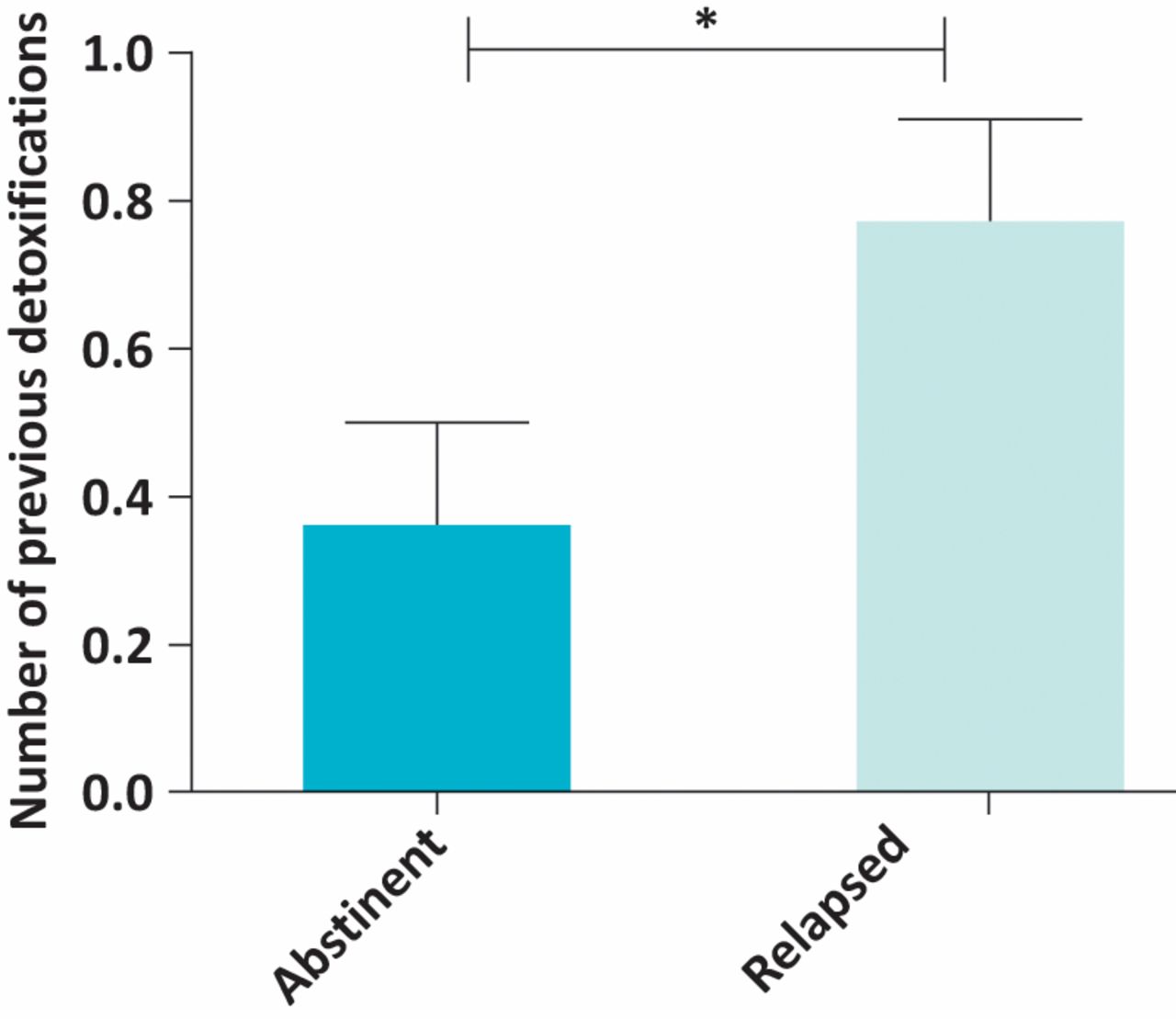
Previous detoxifications. Number of previous detoxifications per patient; patients in the relapse group had undergone significantly more previous detoxifications per patient (p<0.05; 0.77±0.7) when compared to those in the abstinent group (0.35±0.6).
The elective detoxification service protocol stipulates that patients should attend with an undetectable blood alcohol concentration (<10 mg/dL) on the morning of admission. This follows a pre-admission period of outpatient support to safely reduce daily alcohol intake, culminating in patients having their ‘last drink’ the day before admission. Patient engagement with this process is considered vital to ensure commitment to change and to reduce the risk of delirium tremens during admission. Patients presenting to their admission appointment with blood alcohol concentration >10 mg/dL were defined as ‘failed’ admissions. These patients were sometimes offered admission at a later date. Five patients presented to their initial admission appointment with ‘failed’ blood alcohol concentrations (range 22–298 mg/dL). Of these ‘failed’ admissions, 100% went on to relapse at 12 months.
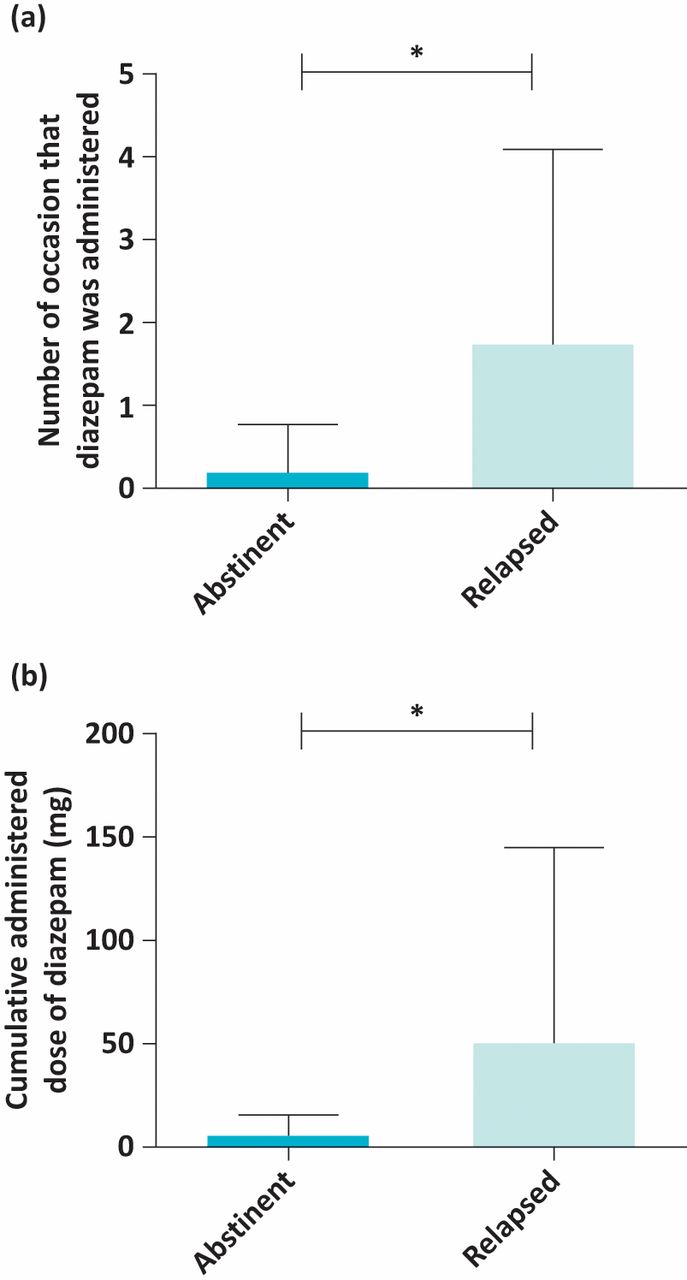
Benzodiazepine prescribing during the elective inpatient detoxification was investigated between the two outcome groups. The proportion of patients requiring diazepam administration in the relapse group (47.6%) was greater than that observed in the abstinent group (9.1%). More specifically, the number of occasions that diazepam administration was required per patient (relapse group = 1.7±2.4 occasions; abstinent group = 0.18±0.6 occasions; p<0.05; Fig 3) and the total cumulative dose of diazepam administration per detoxification (group median 60 mg (IQR 20–120 mg); relapse group = 48.4±96.1 mg; abstinent group = 3.6±12.1 mg; p<0.05; Fig 3) were significantly greater in the relapse group compared to the abstinent group. No association was observed between cumulative dose and number of occasions dosed with diazepam or days abstinent (r = -0.24; p>0.05) and no significant predictive value of dose of diazepam and number of occasions dosed with diazepam on ultimate abstinence at 1 year was demonstrated (supplementary material S1).
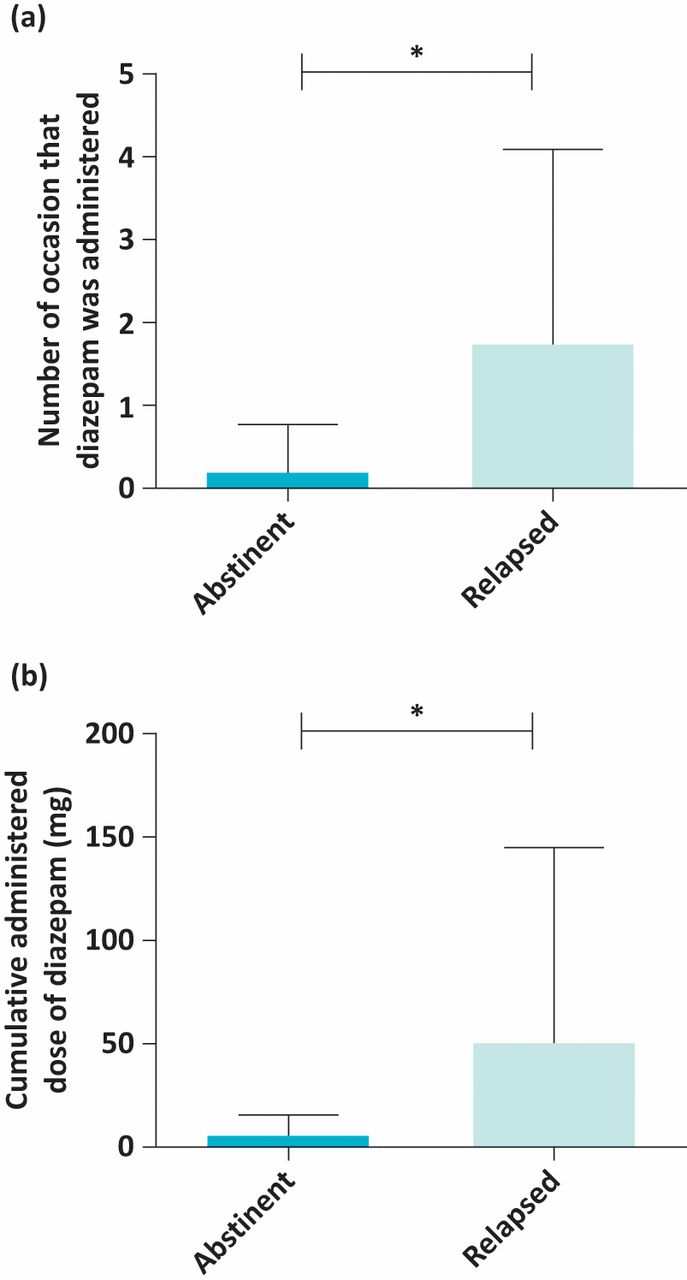
Benzodiazepine prescribing patterns. a) Cumulative diazepam administration – patients in the relapse group required a significantly larger cumulative dose of diazepam (p<0.05; 48.4±96.1 mg) during their elective inpatient detoxification when compared with the abstinent group (3.6±12.1 mg). b) Number of occasions of diazepam administration – patients in the relapse group required administration of diazepam on significantly more occasions (p<0.5; 1.7±2.4) than those in the abstinent group (0.18±0.6).
Service performance and resource use
Referral routes are demonstrated in Fig 4. The majority of patients who remained abstinent at 12 months had been referred by their general practitioner (GP; 88.2%), with only one in six patients referred by the acute medical unit remaining abstinent at 12 months (Fig 4).
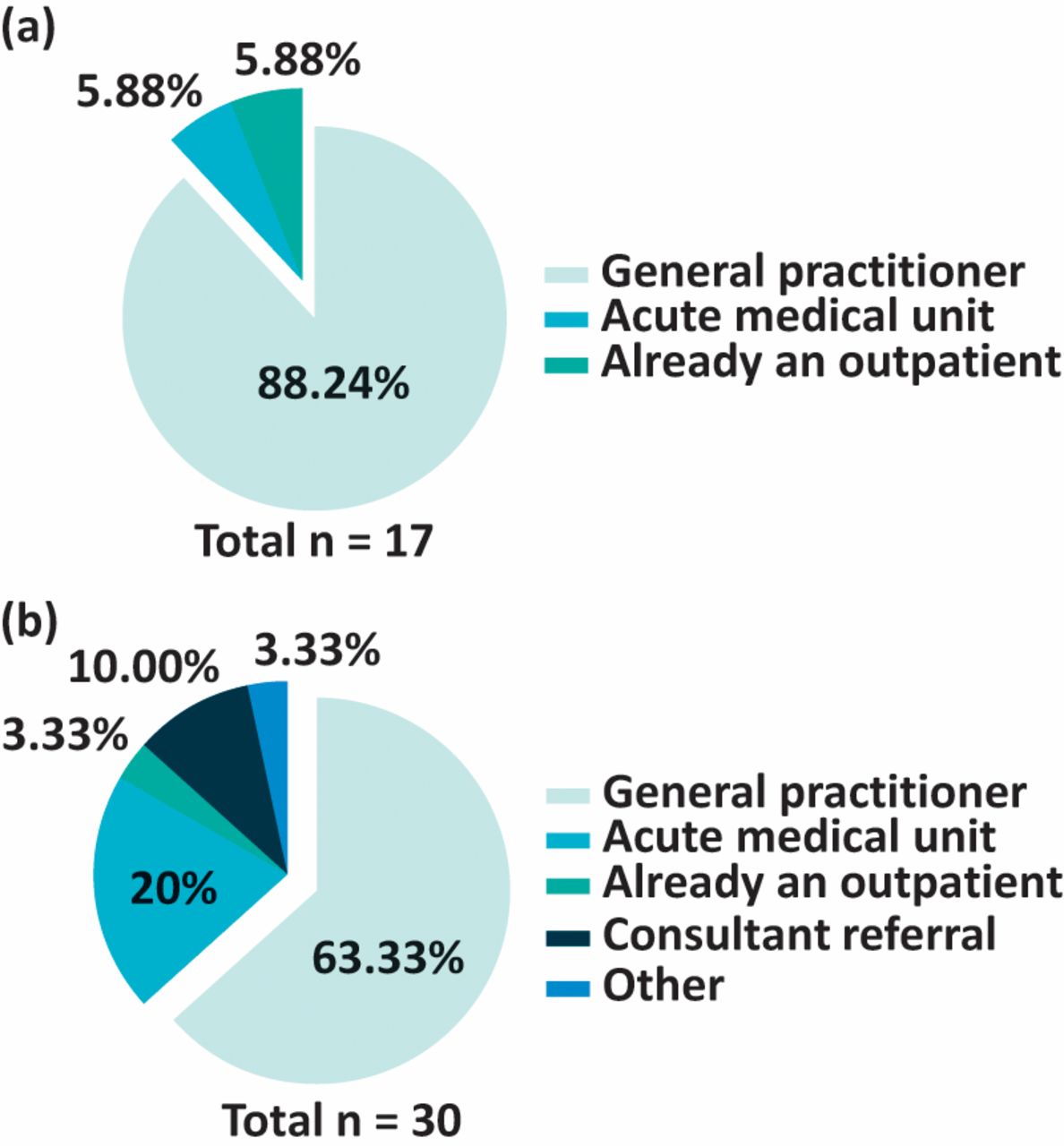
Referral routes. a) Referral routes across patients remaining abstinent at 12 months. b) Referral routes for those relapsing at 12 months.
A summary of patient time-lines in the elective detoxification program is presented in supplementary material S2. The time from referral to admission for detoxification was significantly greater in the relapse group (median 47.0 days (IQR 29.5–98.0); p<0.05) when compared to the abstinent group (median 31.0 days (IQR 11.0–53.0)).
The percentage of patients attending their first post-detoxification follow-up appointment in the relapse group was 63.3%; 13.0% (four patients) did not return to clinic at all. In contrast, in the abstinent group 94.1% of patients attended their first follow-up appointment and only one patient failed to return at all (but remained in contact with support services).
Discussion
An elective inpatient detoxification service was evaluated in terms of efficacy and resource use. Following elective admission and detoxification, the abstinence rates at 3, 6 and 12 months post-detoxification were 68.1, 44.7 and 36.2%, respectively. This compares favourably to a meta-analysis of the efficacy of acamprosate in maintaining abstinence in which abstinence at 6 months was 36.1% with acamprosate therapy and 23.4% with placebo.12 In contrast, the WMPU post-detoxification support is motivationally based and acamprosate was not used. Owens et al reported a 12-month abstinence rate of 53% in patients receiving baclofen therapy as an adjuvant to maintaining sobriety while attending a joint liver and alcohol treatment clinic in Liverpool.13 However, only 113 of the original 219 patients in the cohort were included in the analysis due to non-attendance or non-adherence with the medication, and thus the 12-month abstinent rate on an intention to treat basis was 27%. In comparison, for the WMPU patients the 12-month abstinence rate on an intention to treat basis was 17/57 (29.8%) and without the use of drug therapy.
It is noteworthy that patients admitted to WMPU often required minimal or no pharmacological intervention during admission. This occurred in association with robust pre-admission outpatient assessment and clarification of individual commitment to change combined with support to reduce alcohol consumption prior to a planned admission. We have previously demonstrated that when compared with conventional, non-elective, methods of managing alcohol withdrawal in acute medical services, the elective inpatient service is likely to be superior in terms of its long-term abstinence and readmission rates.7 Our experience suggests that detailed outpatient assessment and preparation prior to an inpatient detox, accompanied by support and engagement with a dedicated hospital alcohol service is an efficacious method of providing long-term abstinence from alcohol without the need for further pharmacotherapies. In addition, the observation that with this approach many patients required little pharmacological intervention during their elective admission has prompted the development of an ambulatory alcohol detoxification service as an alternative/combination option to inpatient care.
The number of patients requiring benzodiazepines in order to successfully complete their elective detoxification was greater in the relapse group compared with the abstinent group. In addition, the relapse group had undergone significantly more previous detoxifications compared with the abstinent group. In agreement with our findings, Malcolm et al demonstrated a poorer outcome in patients in terms of number of days spent drinking and number of heavy drinking days in those who had undergone previous detoxifications.14 Together, this information can be used to further optimise the detoxification service whereby patients with previous detoxifications could be more intensely followed up during the pre-admission period to ensure adequate relapse prevention preparation. Alternatively, these individuals may be identified as being better suited to residential programmes for a longer supervised rehabilitation period, albeit such services are scarce and expensive.
The elective detoxification service performs within national targets with respect to waiting times for non-emergency consultant-led treatment, with patients being seen both in outpatients and as an inpatient well within the 18-week referral to treatment pathway recommendations. Patients referred to the service by their GP were admitted for detoxification faster following referral and were more likely to remain abstinent at 12 months when compared to those referred by acute medical units or the emergency department. This is consistent with a degree of pre-referral assessment by the family doctor with greater assurance of motivation and commitment to lifestyle change than those referred following an acute emergency presentation.
The outpatient non-attendance rate before detoxification was comparable to the national average.15 However, following detoxification the proportion of unattended appointments increased. The proportion of patients not attending their first outpatient follow-up after detoxification was notably greater in the relapse group, and suggesting that early engagement with motivational support is important in maintaining sobriety.
Cost estimation
The estimated cost of detoxification was calculated using the following algorithm:Cost of new patient appointment (£200) + (cost of outpatient follow-up appointment (£112) x number of pre- and post-detoxification outpatient appointments) + cost of admission appointment (£168) + (cost per day of acute medical unit2 bed (£539) x length of stay of detoxification admission).
The median cost per patient from initial referral to 12-month follow-up was £2,769 (IQR 2,377–3,746); this did not differ between those that remained abstinent (£3,084 (IQR 2,309–3,656)) and those that had relapsed (£2,748 (IQR 2,377–3,802)) during the 12-month follow-up period. The total cost for all patients was £173,388 with the abstinent group representing 31.0% of this resource use and the relapse group representing 69.0%.
The National Treatment Agency for Substance Misuse (NTASM) suggest that an alternative to the elective detoxification service such as inpatient residential rehabilitation services cost commissioning groups around £600 per week, with the average stay being approximately 13 weeks.16 We demonstrate that for £53,698, 16 patients remained abstinent for at least 12 months. The same level of abstinence at residential services would cost in excess of £124,800. In addition, the NTASM suggest that for every 10 patients that undergo residential rehabilitation, only three successfully overcome their dependency.16 As such, it could be suggested that the elective alcohol detoxification service provides a similar outcome of abstinence (∼36%) for a far lower cost. The proposed development of an ambulatory detoxification option as part of the expanded in-house alcohol team offers potential further cost savings in the future.
Limitations and future work
This study has several limitations; the numbers are small, compromising statistical power, and as a retrospective case-control design it is vulnerable to confounds and bias, notably it considered only patients who had engaged and proceeded through the referral process to the point of admission for detoxification. These participants had successfully engaged with the pre-admission ‘work-up’, which included, where necessary, some reduction in daily alcohol consumption. The median declared daily alcohol intake at presentation of study participants was modest at 26 units, consistent with this group being less seriously heavy drinkers. This is further reflected in the observation that the median total dose of diazepam per detoxification admission was only 60 mg. Future work should prospectively include all referrals to the service and assess more definitively how best to identify those for whom admission to hospital is the best management option. This would require review not only of the source of referral but also take into account patient factors including mental health, employment and housing status, presence of family or other social support etc. These factors could be utilised in a multivariate analysis not only to inform patient selection and management pathway planning but also in reviewing and predicting relapse risk and hence assist in relapse prevention planning.
Since completion of this study, SWBH has invested in an in-house alcohol team to support and expand the service developed by the clinicians of the WMPU. The new team, now working across two sites, comprises four alcohol specialist nurses, two alcohol practitioners and an administrator. This team has enabled several improvements to the elective detoxification pathway described here. For example, the present study suggested that early engagement with follow-up after admission for detoxification was positively associated with maintenance of sobriety. The SWBH alcohol team has enabled an expanded rapid-access outpatient assessment service with greater availability of pre- and post-detoxification review appointments, including telephone support where appropriate. It is anticipated that highly motivated patients with low risk of medical complications could be offered ambulatory detoxification with daily outpatient review by a nurse prescriber and/or consultant clinical toxicologist, with the associated cost benefits of no inpatient stay. The new team has initiated detailed prospective data collection, including socioeconomic and health factors, that will facilitate future multivariate analysis to improve patient care and resource utilisation. The impact of this team on the elective detoxification pathway will be reported in future publications together with data regarding other aspects of an in-house alcohol team including admission avoidance, improved patient experience and better interaction with existing community-based alcohol services.
Conclusions
The present study demonstrates that an elective inpatient detoxification service is a cost-effective, efficacious method of providing long-term abstinence. Maintained abstinence at 12 months was more likely in those with undetectable blood alcohol on the day of admission, those with fewer previous detoxifications and those referred by their GP. Those who maintained sobriety also had a lower requirement for benzodiazepines during admission. The absence of a predictive association between the individual factors and long-term abstinence using logistic binary regression likely represents the multi-factorial nature of achieving on-going sobriety. We propose that a specialist-led elective alcohol detoxification service offers improved patient outcomes and cost savings for the health service, both in the short term with regard to the cost of achieving sobriety and in the longer term as a result of a reduced overall burden of alcohol dependence.
Acknowledgements
We would like acknowledge the generous elective bursary contribution from the Sands Cox charity which financially supported Darren Quelch during this research. In addition, we would like to acknowledge Dr Faraz Saleem for his help with data acquisition during the study.
Supplementary material
Additional supplementary material may be found in the online version of this article at http://futurehospital.rcpjournal.org :
S1 – Elective alcohol detoxification table.
S2 – Elective alcohol detoxification figure.
- © Royal College of Physicians 2019. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.