
ABSTRACT
Effective hospital readmission risk prediction tools exist, but do not identify actionable items that could be modified to reduce the risk of readmission. Polypharmacy has attracted attention as a potentially modifiable risk factor for readmission, showing promise in a retrospective study. Polypharmacy is a very complex issue, reflecting comorbidities and healthcare resource utilisation patterns. This investigation compares the predictive ability of polypharmacy alone to the validated HOSPITAL score and LACE index readmission risk assessment tools for all adult admissions to an academic hospitalist service at a moderate sized university-affiliated hospital in the American Midwest over a 2-year period. These results indicate that the number of discharge medications alone is not a useful tool in identifying patients at high risk of hospital readmission within 30 days of discharge. Further research is needed to explore the impact of polypharmacy as a risk predictor for hospital readmission.
Introduction
Hospital readmissions are common and expensive, with nearly 20% of Medicare patients being readmitted to a hospital within 30 days of discharge at an overall cost of nearly US$20 billion per year.1 Because of this high frequency and cost, hospital readmissions are a target for healthcare cost savings in the Medicare Hospital Readmission Reduction Program (HRRP). Therefore, healthcare organisations are investing considerable resources into efforts to reduce hospital readmission.
The underlying risk factors for hospital readmission are diverse. Studies have identified age, ethnicity, lack of outpatient healthcare provider, major surgery, medical comorbidities, length of hospitalisation, previous admissions, failure to transfer important information to the outpatient setting, early discharge and the number of discharge medications etc are associated with hospital readmission within 30 days.2–5 However, clinicians still struggle to predict the patients who are at high risk of hospital readmission.6
Readmission risk assessment can be accomplished with a variety of assessment tools that range from multidisciplinary patient interviews to simple screening tools using a handful of variables.4,7–9
The easy to use HOSPITAL score is one such screening tool.10 The HOSPITAL score uses seven readily available clinical predictors (haemoglobin level at discharge, discharge from oncology, sodium level at discharge, procedure during hospitalisation, index admission type, number of hospital admissions and length of stay) to accurately identify patients at high risk of potentially avoidable hospital readmission within 30 days (Table 1). This score has been internationally validated in a population of over 100,000 patients at large academic medical centres (average size of 975 beds) and has been shown to have superior discriminative ability over some prediction tools.8,10,11
HOSPITAL score
Another simple prediction model for predicting hospital readmission which uses both administrative and primary data is the LACE index.12 The LACE index uses four variables: length of stay, acuity of the admission, comorbidity of the patient and emergency department use in the duration of 6 months before admission.12 This model has been internally validated using data collected from 4,812 patients discharged from 11 community hospitals in Ontario, and it was externally validated using administrative data collected randomly from 1,000,000 discharges.12 The LACE index has been shown to have moderate discrimination in studies conducted in North America with over 26,000 Medicare admissions,13 110,000 discharges in the Chicago, Illinois area 14 and 600 patients in a community hospital.15
Despite this accuracy, these risk identification tools do not identify modifiable risk factors for hospital readmission.10,16,17 Identifying and evaluating potentially modifiable risk factors for readmission, such as polypharmacy, is a focus of active investigation.2,18,19
The role of polypharmacy as an independent risk factor predicting 30-day readmission is a recent debate. 20,21 Morandi et al studied the risk of readmission to elderly patients admitted to a rehabilitation facility and found that having a prescription of seven or more medications significantly increased the risk of hospital readmission within 30 days (hazard ratio (HR) 3.94; 95% confidence interval (CI) 1.62–9.54; p = 0.002).22 Another study showed that polypharmacy increases the risk of hospital admission with a dose-response relation (5–9 drugs: odds ratio (OR) 1.18; 95% CI 1.12–1.24; ≥10 drugs: OR 1.54; 95% CI 1.42–1.66).23
Our study compares the HOSPITAL and LACE readmission scores with number of medications on discharge as predictors for 30-day readmission in a university affiliated hospital in the American Midwest.
Materials and methods
All eligible adult medical patients discharged from the Southern Illinois University School of Medicine (SIU-SOM) hospitalist service from Memorial Medical Center, a university-affiliated tertiary care centre from 01 January 2015 to 01 January 2017 were studied retrospectively to determine if the number of discharge medications was a significant predictor of all-cause (avoidable and unavoidable) hospital readmission within 30 days. Exclusion criteria included transfer to another acute care hospital, leaving the hospital against medical advice or death. The endpoint of within 30 days of hospital discharge for all-cause readmission was chosen because it is the measure used by the Medicare HRRP.
Data on age, gender, diagnosis related group, International Classification of Disease (ICD) diagnosis codes, emergency department visits in the last 6 months, length of stay, hospital readmission within 30 days, discharge medications, and the other variables in the HOSPITAL score (Table 1) and LACE index (Table 2) were extracted from the electronic health record in a de-identified manner for analysis. Missing laboratory data (haemoglobin and sodium from the day of discharge) were coded to be in the normal range as was done in the international validation study of the HOSPITAL score.11
LACE index
Quantifying medications at the time of hospital discharge was accomplished in the same manner as outlined by Picker and colleagues by counting all medications prescribed at the time of hospital discharge, excluding over the counter medications or nutritional supplements.2
The study hospital does not have a distinct oncology admitting service. To address the increased risk of readmission in oncology patients found in other studies using the HOSPITAL score, this study classified patients with oncology related diagnosis ICD codes to have been discharged from an oncology service. Because data is only available from the study hospital, readmissions at other hospitals were not detected.
Institutional review board review for this study was obtained from the Springfield Committee for Research Involving Human Subjects. This study was determined not to meet the criteria for research involving human subjects according to 45 CFR 46.101 and 45 CFR 46.102.
Statistical analysis
The number of medications at discharge, the HOSPITAL score and LACE index were investigated as predictors of all-cause hospital readmission within 30 days. Qualitative variables were compared using Pearson χ2 or Fisher's exact test and reported as frequency (%). Quantitative variables were compared using the non-parametric Mann–Whitney U test and reported as mean ±standard deviation.
The HOSPITAL score and LACE index were calculated for each admission. HOSPITAL scores of 0–4 points were classified as low risk for readmission (5%), 5–6 points as intermediate risk (10%), and >7 more points as high risk (20%) based on the initial validation study of the HOSPITAL score.10
LACE indexes ranged from 0–19, with an expected probability for readmission of 0% to 43.7% based on the initial validation study of the LACE score.17
Discharge medication numbers ranged from 0–12 or more, with expected probabilities of readmission based on the work of Picker and colleagues.2
These readmission risk predictions were used to calculate a Brier score to evaluate the accuracy of each predictor. Two sided p-values <0.05 were considered significant. Variables from univariate analysis with a p-value of 0.05 or less were evaluated using multivariate logistic regression with stepwise backward variable selection.
Most statistical analyses were performed using SPSS version 22 (SPSS Inc, Chicago, USA).
The Brier score was calculated with R version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
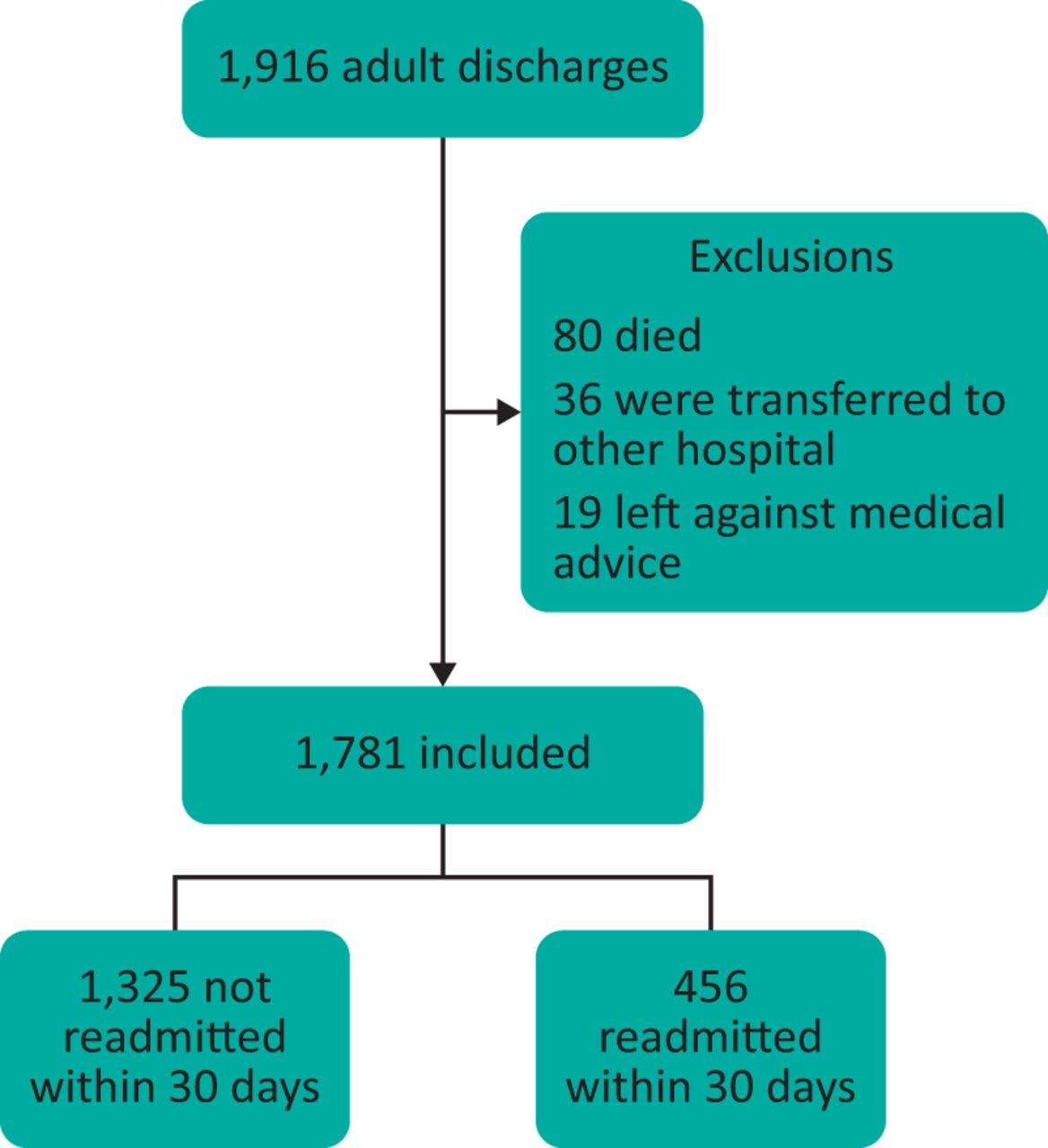
During the study period (2 years), 1,916 discharges were recorded for the SIU-SOM hospitalist service. The analysis includes data for the 1,781 discharges for 1,410 individual patients that met inclusion criteria (Fig 1). Of these discharges, 456 (27%) were readmitted to the same hospital within 30 days. The overall study population was 47% female, had an average age of 63 years and spent an average of 7.9 days in the hospital.
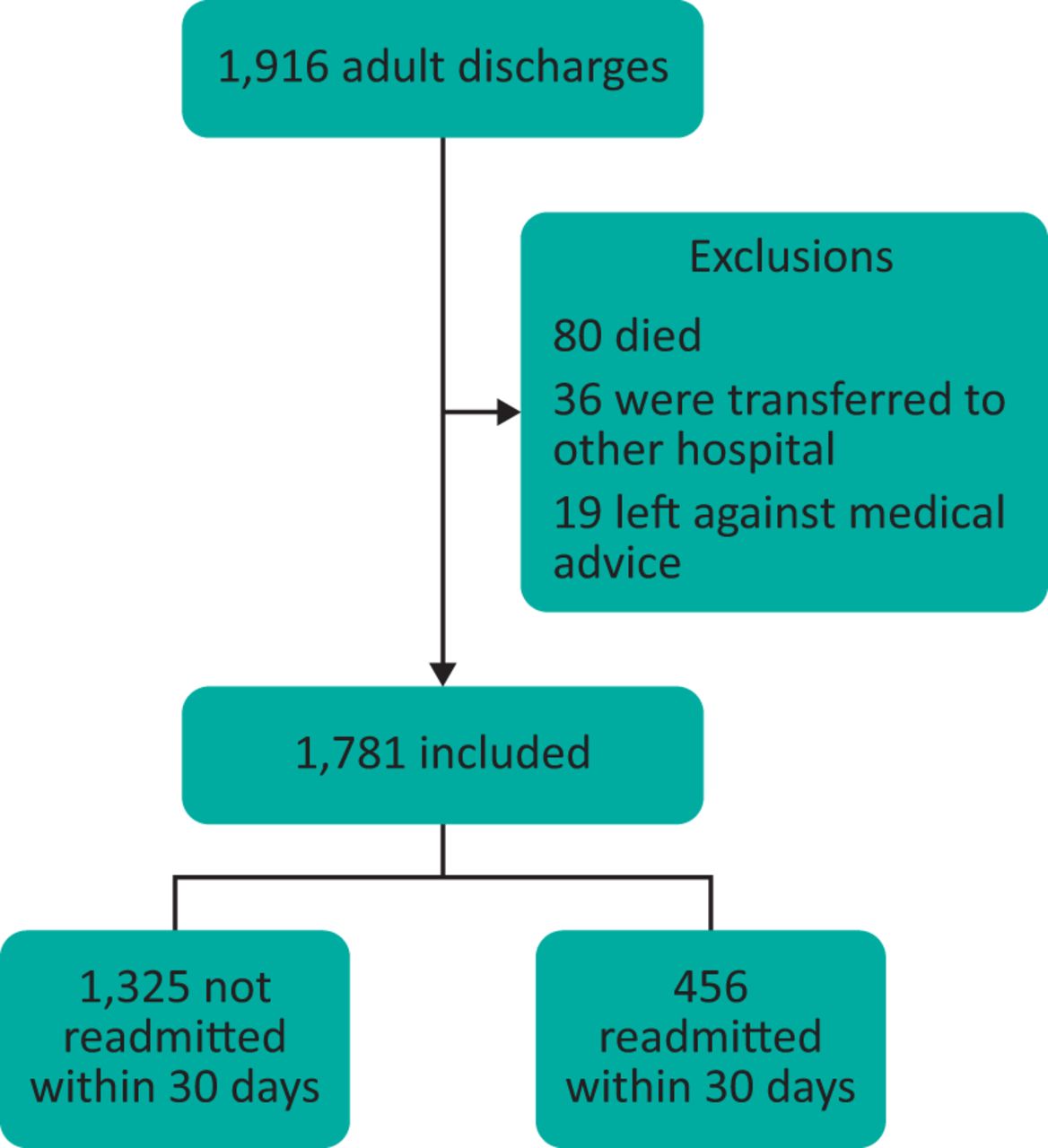
Study flow diagram.
The patients readmitted within 30 days of discharge were more frequently admitted to the hospital in the last year, evaluated in the emergency department in the last 6 months, had higher HOSPITAL scores, higher LACE index values, higher Charlson comorbidity scores, and had more medications at the time of discharge. The medical comorbidities of a history of myocardial infarction, congestive heart failure (CHF), cirrhosis, diabetes and renal disease were seen more frequently in readmitted patients. These differences were statistically significant in univariate analysis (Table 3). Multivariate analysis did not show the number of medications at the time of hospital discharge to be a risk factor for hospital readmission (Table 4).
Baseline characteristics of the study population by 30-day readmission status
Multivariate logistic regression of potential risk factors for hospital readmission within 30 days of discharge
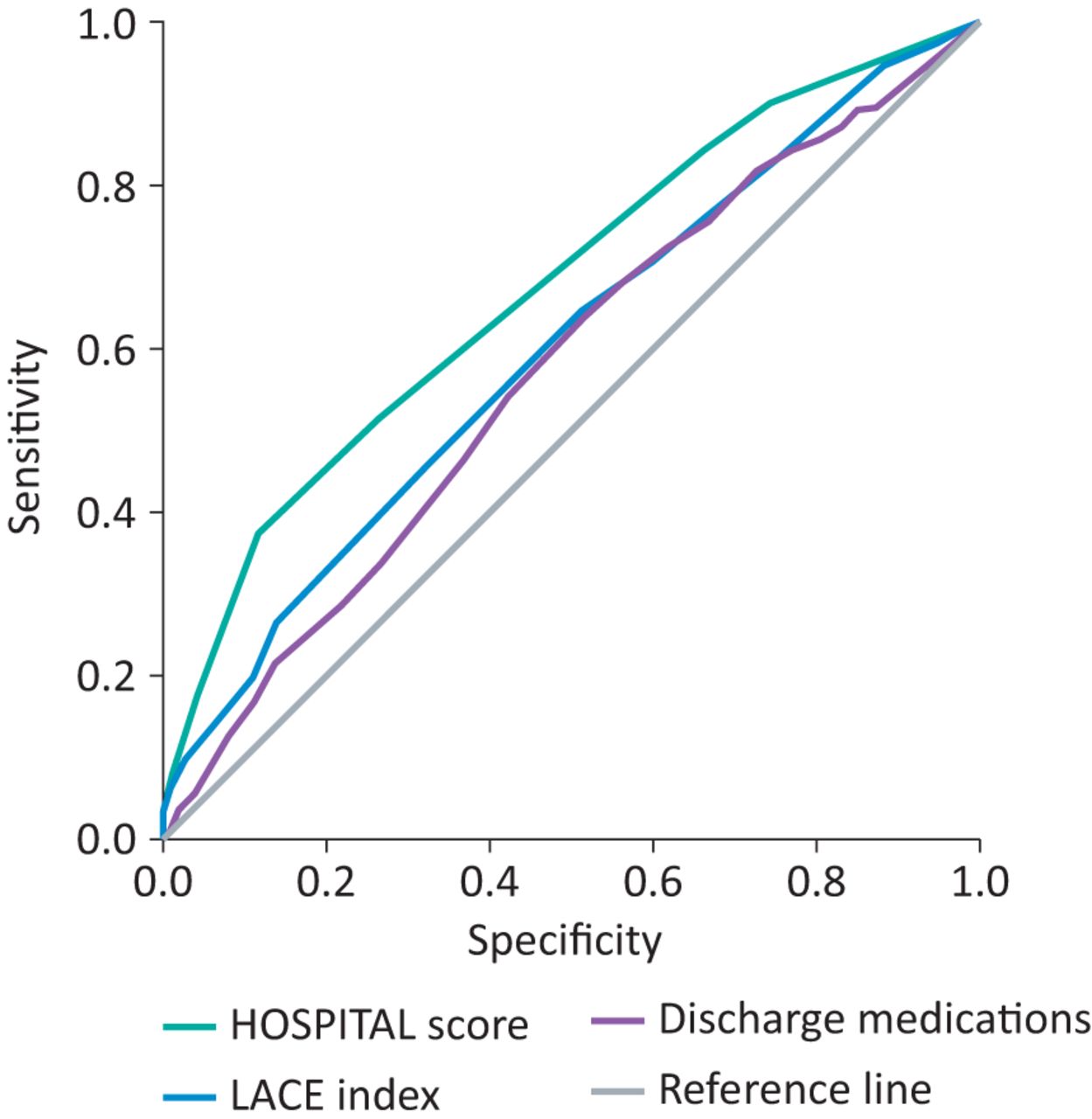
A receiver operating characteristic evaluation (Fig 2) showed that the HOSPITAL score and LACE index had fair discrimination for hospital readmission in this population. The HOSPITAL score had a C statistic of 0.675 (95% CI 0.65–0.70), a Brier score of 0.217, and a Hosmer–Lemeshow goodness of fit test showed a χ2 value of 10.36 with a p value of 0.035. The LACE index had a C statistic of 0.598 (95% CI 0.58–0.64), a Brier score of 0.212, and a Hosmer–Lemeshow goodness of fit test showed a χ2 value of 6.15 with a p value of 0.292. The number of discharge medications had a C statistic of 0.571 (95% CI 0.54–0.60), a Brier score of 0.200, and a Hosmer-Lemeshow goodness of fit test showed a χ2 value of 10.13 with a p value of 0.182.
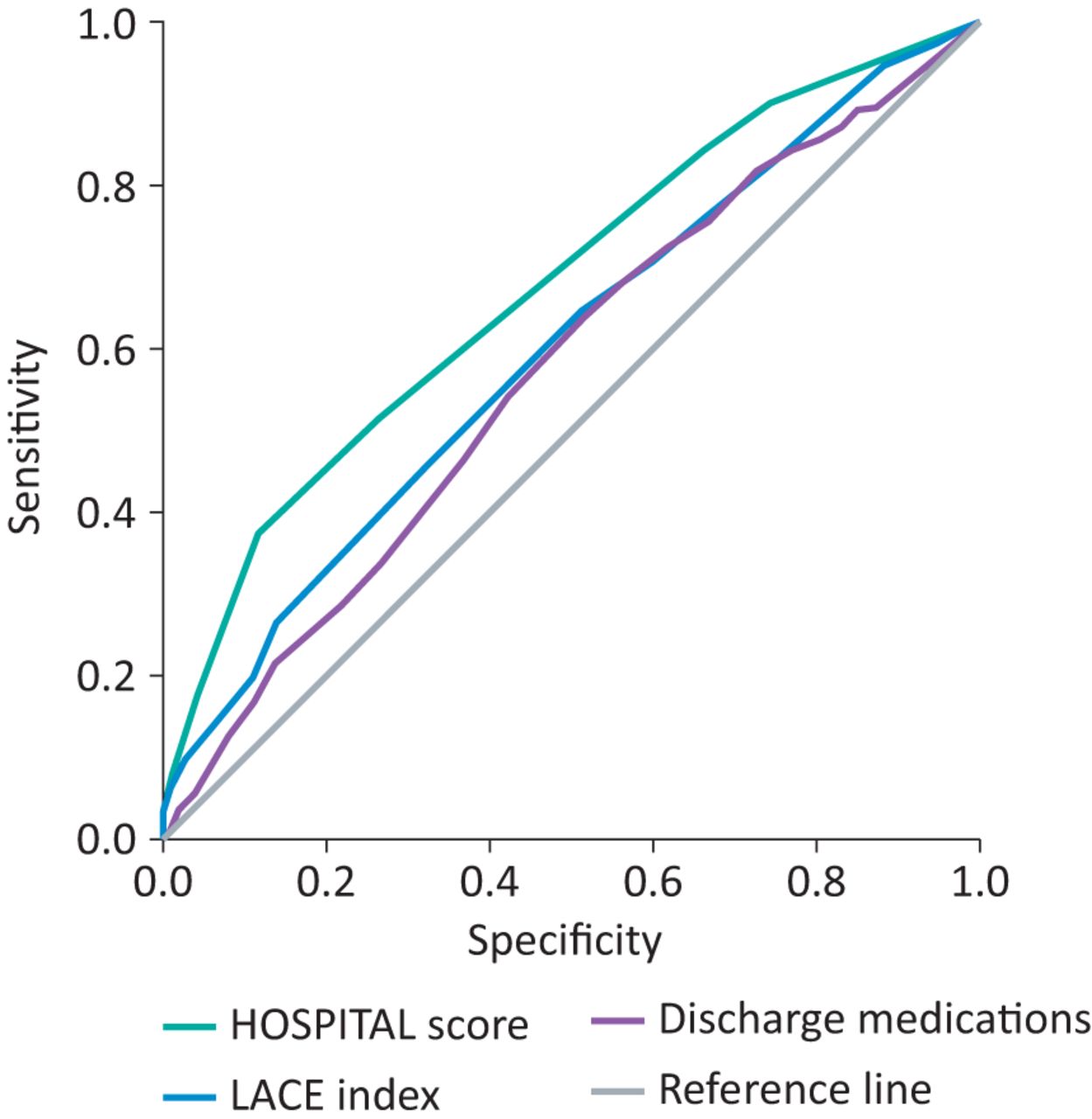
Receiver operating characteristic curves for the number of discharge medications, HOSPITAL score and LACE index.
Discussion
In the current study, we compared the use of HOSPITAL score, the LACE index and the number of medications upon discharge for predicting all-cause of hospital readmission in our study population. We found that the number of medications prescribed upon hospital discharge is not a significant predictor of hospital readmission in a moderate sized not-for-profit university-affiliated tertiary care hospital in the American Midwest. The appropriateness of medication therapy should not always be assessed by the number of medications alone. Complex multiple drug treatment regimens are often required for medical conditions such as CHF and diabetes, which were more prevalent in the patients readmitted to the hospital within 30 days of discharge. The higher Charlson scores and a higher prevalence of medication intensive comorbidities such as diabetes in the group readmitted to the hospital within 30 days of discharge is likely to be causal of the polypharmacy. However, only CHF and renal disease appear to be statistically significant predictors of hospital readmission in multivariate analysis.
Interpretation of these findings is complicated because there is no agreement on a standard cut-off point for the number of medications prescribed in the definition of polypharmacy. Problems arise when more medications are prescribed than are clinically required. The concurrent use of multiple drugs or more drugs than medically necessary is polypharmacy.24 Various arbitrarily chosen cut-off points are used to evaluate prevalence and 30-day hospital readmission in several studies.25,26 Many studies in ambulatory care define polypharmacy as a medication count of five or more medications. The prevalence of polypharmacy in age >65 years, the concomitant use of five or more medications, was 51.9% at hospital admission and 67.0% at discharge, and it was not associated with a poor hospital outcome.25 Often, the hospital readmission predictors include polypharmacy (≥6 medicines).26
The study that looked at polypharmacy (≥6 medicines) showed an estimated odds ratio for readmission for high Charlson scores of 1.7 (95% CI 1.1–2.6) and of 2.1 for polypharmacy (95% CI 1.3–3.7). The model yielded a readmission risk estimate of 6% if neither a high Charlson score nor polypharmacy was present, 9% if only the Charlson score was high, 12% if only polypharmacy was present, and 19% if both were present.26
Picker et al identified more than six discharge medications to be independently associated with 30-day readmission.2 The results of our study differ from other published work in the role of polypharmacy, and hospital readmission risk is likely due to significant differences in our study population and other populations. The overall readmission rate (27% vs 21%), average age (64 vs 55 years), Charlson comorbidity score (6 vs 5), length of stay (8 vs 4 days) and number of medications at time of discharge (12 vs 7) were significantly higher in those readmitted to the hospital when compared with the data reported by Picker and colleagues.2 Several of these differences (age, Charlson score and length of hospital stay) are known predictors of increased hospital readmission risk and are components of the HOSPITAL score and LACE index.8,10,17
The performance of the established and validated HOSPITAL score and LACE index in our study was comparable to prior investigations at this centre27,28 and validation studies of the HOSPITAL score11,13 and LACE index.13,17 Local practice details such as no distinct oncology admitting service and infrequent laboratory testing on the day of hospital discharge likely reduce the accuracy of the HOSPITAL score in this setting. Despite these factors, the predictive ability of the HOSPITAL score was comparable to validation studies of the HOSPTIAL score.11,13 Missing laboratory values needed for the calculation of the HOSPITAL score were addressed using the methodology used in the international validation study of the HOSPTIAL score by Donzé and colleagues.11
Our study has several important limitations. This study and the international validation study for the HOSPITAL score share an important shortfall by only identifying readmissions within 30 days at the same hospital.11 This limitation was overcome in the LACE index original validation study by contacting the patient 30 days after discharge of the hospital to determine the readmission status.17 Furthermore, our study is retrospective, single centre, focused on medical patients, small sample size and shaped by local practice patterns (no oncology admitting service, few elective admissions, infrequent laboratory testing on the day of discharge). These local factors could lead to underestimation of the risk of readmission with the HOSPITAL score. The high rate of readmission is likely because the study hospital deals with the underserved high-risk populations in the region. The generalisability of these results may be reduced because of these limitations.
Conclusions
Our study demonstrated that the number of discharge medications alone does not appear to be a useful tool for a moderate sized community hospital to identify patients at high risk of hospital readmission within 30 days. Other risk scoring systems such as the HOSPITAL score and LACE index are more effective at identifying high-risk patients. Our study further supports the need for more research to explore polypharmacy as a risk predictor for hospital readmission. Evaluating the interaction of specific medical comorbidities and medications may be a high-yield avenue for investigation.
- © Royal College of Physicians 2019. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.