
ABSTRACT
Objectives In 2015, three London cardiac centres, with different transfusion infrastructure support, merged to form the Barts Heart Centre. We describe the impact on transfusion rate, blood usage and interoperator variation.
Design Data was collected on all adult patients undergoing cardiac surgery during 2014 as well as 2016, using the National Institute Cardiovascular Outcomes Research (NICOR) data set.
Measurements and main results Over the two time periods, a total of 3,647 cardiac procedures were performed (1,930 in 2014 and 1,717 in 2016). There were no significant differences in type of surgery or patient comorbidity between the two epochs of time. Overall, red blood cell transfusion at 24 hours and until hospital discharge reduced significantly in 2016 (odds ratio 0.77; 95% confidence interval 0.68–0.89; p=0.0002). Interoperator variability (adjusted for comorbidities) reduced after merger from standard deviation 0.394 (standard error (SE) 0.096) to 0.269 (SE 0.082), p=0.001.
Conclusion Clinical and organisational factors can improve transfusion service.
Introduction
Transfusion of blood components during cardiac surgery is associated with morbidity and mortality resulting in substantial costs for the NHS in the UK.1 In 2011, the National Comparative Audit of Blood Transfusion captured 6,140 patients at 66% of UK cardiac surgery centres, demonstrating high transfusion rates: red blood cells (RBC) were administered to 43%, 52% and 72% of patients undergoing coronary artery bypass grafts (CABG), valve repair/replacement surgeries, and CABG and valve repair/replacement surgeries, respectively.2 However, the use of blood components varied widely between centres, most likely due to limited evidence for administering blood transfusion to patients undergoing cardiac surgery.
In March 2015, three London cardiac centres, the London Chest Hospital (LCH), St Bartholomew’s Hospital (SBH) and the Heart Hospital (THH), merged to form the Barts Heart Centre (BHC) on the St Bartholomew’s Hospital site, serving approximately 10% of the UK population and operating as one of the busiest cardiac surgery centres in Europe. The service reorganisation and merger of three hitherto separate teams required careful review of protocols and standardisation of practices. Provision of blood transfusion services differed pre- and post merger, in terms of organisation and infrastructure.
Prior to the merger, only the SBH site had onsite remote blood fridges allowing clinicians to access RBC from the fridge without contacting the transfusion laboratory, while plasma and platelet components were being provided by offsite transfusion laboratories at all three sites.
Following the merger, the intention was to open an onsite transfusion laboratory that served the new BHC 24 hours a day, 7 days a week and that all transfusion protocols and guidelines were harmonised in line with the national guidelines and the new structure.6 The aim of this cohort study was to describe the impact of the merger on the overall incidence of any blood transfusion in patients undergoing cardiac procedures at 24 hours, 72 hours, and until discharge, or death, or 30 days (whichever occurred first); the overall blood usage and wastage; and anonymised interoperator variation in blood transfusion rates and intraoperator changes in practice after the merger.
Methods
This was a cohort comparison study analysing prospectively collected data on patients undergoing cardiac surgery at three sites between 01 January and 31 December 2014, and at the BHC between 01 of January and 31 December 2016. The study met the criteria for service evaluation under the Health Research Authority decision tool and was registered and approved by our clinical effectiveness unit (Reference 8300).
Data definitions and data collection
All adult patients (over the age of 18 years) undergoing any cardiac surgery were identified through the National Institute for Cardiovascular Outcomes Research (NICOR) database (www.ucl.ac.uk/nicor/data/datasets), which prospectively stores data on patients’ preoperative comorbidities, the type of cardiac surgery and whether the surgery was elective, urgent or emergent in nature. Unique patient identifiers from the NICOR database were used to extract the transfusion data using the bank manager database for THH, and laboratory information management system (LIMS) Clinisys Winpath version 5 (CliniSys, Chertsey, UK) for other sites. All patient and operator identifiable data in this research database were then de-identified before analyses proceeded and analysts were blinded to these source data.
In the UK, it is a legal requirement that all hospital blood transfusion laboratories have a system in place to document the final destination of every blood component issued (under The Blood Safety and Quality Regulations 2005), so that any probable recipient-related transfusion complications can be traced back to donors and that appropriate measures can be taken.3 These records must be kept in the transfusion laboratories for 30 years. In order for laboratories to comply with above legal requirements, all hospitals have implemented electronic recording of all events in the transfusion chain, using LIMS. The following transfusion information was retrieved: date and time when blood components were issued, product code, product type and ‘episode unit status’ ie used, expired, returned or wasted.
Transfusion services
Prior to the merger, transfusion support was different across different sites.
SBH had an onsite transfusion laboratory daily from 8am to 8pm. Outside this time period, the Royal London Hospital, which was ∼2 miles away, provided laboratory support as required with RBC stored on site in blood fridges as well as two pools of platelets always on standby on a platelet agitator. Fresh frozen plasma (FFP) was issued by the laboratory as required.
LCH had no onsite laboratory, and the Royal London Hospital which was 1.5 miles away provided transfusion support at all times, with onsite remote blood fridges holding RBC stocks only and a platelet agitator storing two pools of platelets. FFP was provided on demand from the main laboratory.
THH had no onsite laboratory, and blood components were provided by the University College Hospital (1.3 miles away) with the following support – onsite remote blood fridges issuing RBC with another back-up fridge containing Group O negative RBC, pre-thawed FFP and a platelet agitator with pools of platelets as required.
SBH and LCH used the same transfusion protocols for the peri- and postoperative period. There was no preoperative haemoglobin optimisation programme for elective surgeries. In the perioperative period, a thromboelastography (TEG) guided protocol was used to manage bleeding patients. Guidance for other blood components remained the same pre- and post merge, as per national transfusion guideline triggers.6 Protocols regarding antiplatelet therapy and the use of cell salvage (autologous transfusion of blood collected from the operating field) before and after surgery were the same for all sites, pre- and post merger. All clinical staff working at the three sites, moved to BHC in 2015, and there were no significant changes in staff expertise.
Cardiac procedures
Cardiac procedures are classified into the following groups: CABG only; isolated valve replacement/repair only; other (including aortic root surgery); CABG and valve replacement/repair; CABG and other; CABG and valve replacement/repair and other; and valve and other.
The NICOR database classifies the type of surgeries into four groups according to their urgency: elective, urgent, emergency and salvage surgeries.
Statistical analysis
Continuous data are presented as median with interquartile range (IQR) and categorical data as frequencies and percentages. Comparisons between the two periods are made using Mann–Whitney U test for continuous variables and χ2 or Fisher’s exact test for categorical data. Unadjusted and adjusted odds ratios (ORs) were obtained using logistic regression modelling. A Firth logistic model was used for the adjusted model due to small numbers in some categories. An interaction term was fitted to assess whether the changes differed between elective and non-elective surgical procedures. The significance level used was p<0.05 (two-sided test) for the primary comparison of any transfusion until discharge and p<0.004 for other components and time points after Bonferroni correction. Wastage was assessed as the number of units wasted relative to the total number of transfusions, with differences tested and incidence rate ratios (IRR) obtained using Poisson models. Analysis of interoperator variability was performed using random effects modelling. One surgeon who only performed two operations was excluded from the analysis. A two-level random intercept model was used to account for any correlation among patients operated on by the same surgeon. Operator performance was plotted using the standardised level 2 residual from the random effects model.
Results
Over the two time periods, a total of 3,647 cardiac surgeries were performed (1,930 in 2014 and 1,717 procedures in 2016, with 19 and 10 patients having more than one procedure, respectively; Table 1). CABG alone, followed by CABG and valve, were the most frequent procedures. There was no significant difference in the type of surgeries, EuroSCORE (European System for Cardiac Operative Risk Evaluation) and preoperative haemoglobin values of patients between the two periods. Following merger, the number of patients undergoing at least one preoperative haematinic test (ie iron/ferritin/B12/folate) increased from 93/1,930 (4.8%) to 168/1,717 (9.8%), p<0.001.
Patient characteristics pre- and post merger
Transfusion rates pre- and post merger are shown in Table 2. The incidence of ‘any’ transfusion (defined as receiving any of RBC, FFP, cryoprecipitate or platelets) at 24 hours, 72 hours and until hospital discharge had overall reduced significantly (OR 0.84; 95% confidence interval (CI) 0.73–0.97; p=0.02) following merger (Table 3), although the reduction lost significance after adjusting for age, gender, procedure type, haemoglobin level and urgency of procedure (OR 0.86; 95% CI 0.73–1.01; p=0.06). Overall, the reduction in RBC transfusion after the merger remained significant at all time points (p≤0.002) after adjusting for all above variables (until discharge OR 0.77; 95% CI 0.66–0.90; p=0.001). There was no significant difference in the RBC reduction effect between elective vs non-elective procedures.
Transfusion rates pre- and post merger
Odds ratios for ‘RBC’ and ‘Any’ transfusion for pre- versus post merger
The overall use of cryoprecipitate transfusion increased after the merger at all time periods, at 24 hours (OR 1.49; 95% CI 1.20–1.86; p=0.0002), at 72 hours (OR 1.41; 95% CI 1.13–1.74; p=0.001) and at discharge (OR 1.37; 95% CI 1.11–1.70; p=0.003). FFP and platelet usage had remained the same. The median (IQR) number of RBC, FFP, platelet and cryoprecipitate units/pools for those that were transfused were 3 (2–5), 3 (2–4), 1 (1–2) and 2 (1–2), respectively, with no significant difference between the pre- and post merger periods.
In total 607/10,074 (6.0%) units were wasted pre-merger compared to 3.7% (328/8,769) post merger (IRR 0.62; 95% CI 0.57–0.67; p≤0.001; Table 4). Merger resulted in 23 fewer units per 1,000 units being wasted. Overall the wastage for FFP (IRR 0.57; 95% CI 0.48–0.67; p<0.001) and platelets (IRR 0.33; 95% CI 0.17–0.63; p=0.001) had reduced significantly after merger, while wastage for RBC (IRR 1.15; 95% CI 0.87–1.54; p=0.33) and cryoprecipitate (IRR 0.89; 95% CI 0.53–1.49; p=0.65) did not change. In total, wastage was lower for non-elective surgery compared to elective (IRR 0.84; 95% CI 0.72–0.97; p=0.018), but there was no difference in the post-merger effect between elective and non-elective surgery (interaction p=0.97).
Blood component wastage for pre- and post merger periods per site
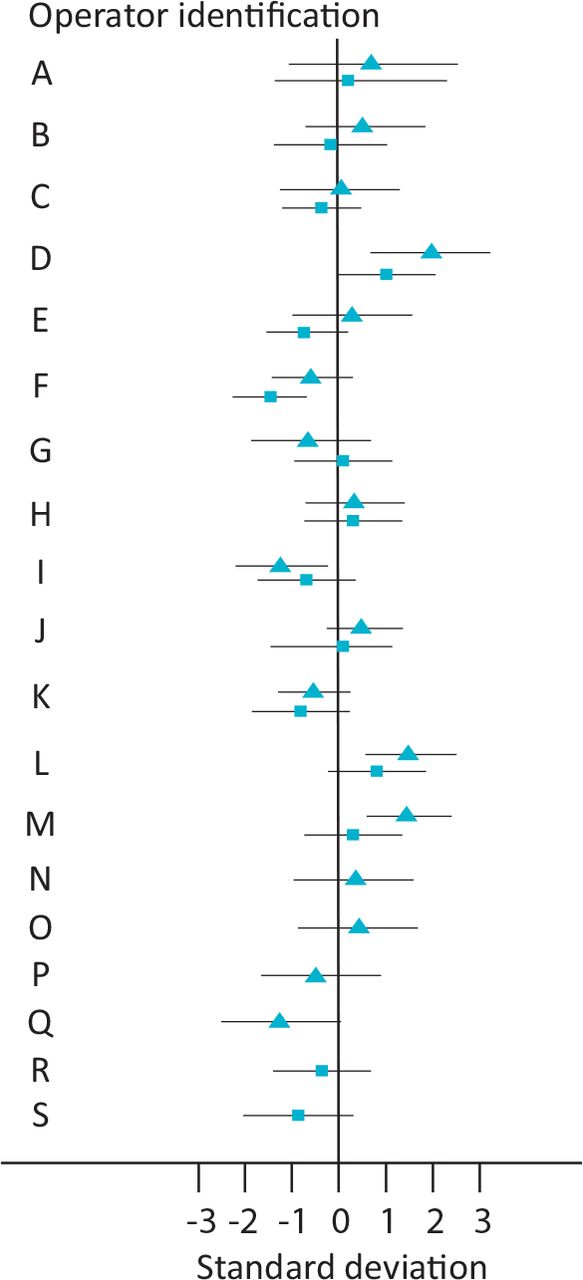
Analysis of interoperator variability (unadjusted) in 2014 showed an overall transfusion rate of 71.2%, with significant variability between operators (SD 0.325; SE 0.087; p<0.001; Fig 1). Transfusion rates between consultants ranged from 52.1% to 85.9%, with 95% of consultants expected to have values between 56.4% and 82.6%. EuroSCORE adjusted analysis of interoperator variability in 2014 showed an overall transfusion rate of 74.1% and significant variability between operators (SD 0.394; SE 0.096; p<0.001), with 95% of consultants expected to have values between 56.5% and 86.3%. In 2014 three operators transfused significantly more than average, and two operators had significantly lower transfusion rates. No operator lay more than two SDs from the mean, so these would not be defined as outliers (Fig 1).

European System for Cardiac Operative Risk Evaluation adjusted consultant outcome by year. Triangle = 2014; square = 2016. The boxes represent the proportion of operations transfused for each surgeon as estimated by the level 2 residual from the random effects model. The horizontal lines show 95% confidence intervals. A value of zero as shown by the vertical line represents the mean transfusion rate over all surgeons and time-points. A value of 1 would indicate that a surgeon’s rate lies one standard deviation above the overall rate and −1 would indicate a value one standard deviation below the average rate.
In 2016, the unadjusted overall transfusion rate was lower than 2014 (67.5%), however the variability between operators still remained significant (SD 0.181; SE 0.079; p=0.04), with transfusion rates per consultants ranging from 53% to 78.8%, and 95% of consultants having values between 59.1% and 74.9%. In 2016, the EuroSCORE adjusted variability between operators dropped after merger (SD 0.269; SE 0.082; p=0.001), and furthermore only one operator has a significantly higher transfusion rate above average, compared with three in 2014.
Discussion
After the merger, we found that the overall use of RBC transfusion has reduced significantly at 24 and 72 hours after surgery, and up to hospital discharge; cryoprecipitate use has increased at all time points (24 hours, 72 hours and up to discharge); platelet and FFP wastage have reduced significantly; and the variability in transfusion practice between consultants reduced significantly.
Our results on blood usage mirror the UK blood usage data, showing that the demand for RBC components has reduced by approximately 7% over the recent years, while the use of cryoprecipitate has increased.7,8 Preoperative practices to optimise haemoglobin (eg treatment of iron deficiency anaemia) have also changed nationally and internationally. The almost doubling in testing of preoperative haematinics could explain the reduction in RBC usage in our cohort after the merger.
The overall use of cryoprecipitate transfusion increased after the merger at all time periods but this did not lead to increase in wastage. Our results confirm the findings of two national audits performed in England and Canada, which showed a rise in cryoprecipitate use, with the commonest indication being cardiac surgery followed by trauma.9,10 The move throughout the international community towards targeting higher fibrinogen levels could explain this trend.
Another interesting finding is the significant reduction in blood component wastage from 6.0% to 3.7% after the merger (p≤0.001), being primarily due to reduced FFP and platelet wastage. This reduction translates to an absolute cost savings of ∼£8,200 per annum (pa) for FFP (unit cost £32) and ∼£5,225 pa for platelets (unit cost £209). Unlike RBC that can be stored in blood fridges near clinical areas, support for FFP and platelets still relies on transfusion laboratories being available to replete stocks. In 2014, both FFP and platelets were pre-emptively ordered in anticipation of requirement and to minimise a potentially harmful delay in the case of major bleeding. If not required, these were often wasted. This changed in 2016, with the introduction of a 24 hours a day, 7 days a week, onsite laboratory, reducing unnecessary ordering and wastage, with cost savings for the institution. Interestingly, UK laboratory services are currently undergoing significant changes as part of the Pathology Modernisation Programme.11 Models to centralise the service are being considered, where laboratories are asked to network with one another to build lager pathology systems that have the capacity to deal with rising demand and technological developments. This modernisation programme will result in sharing services, whereby one organisation is responsible for the blood transfusion services of multiple hospitals, improving quality, efficiency and cost effectiveness but also risking the return of pre-emptive ordering and stockpiling – as described for our 2014 cohort.
The difference in transfusion practice between consultants is one of the most interesting findings of the study. There were three significant outliers in terms of liberal transfusion practice who, although reduced following merger, remained significant in spite of national and local guideline recommendations. The variability between operators reduced, likely an effect of the sharing of best practice in a larger volume department, but consultants identified as being at the upper end of transfusion practice remained so despite correction for EuroSCORE. There is potential for hidden confounding variables in this data, such as subtle case-mix factors not listed in the EuroSCORE which could affect transfusion rates but real-world experience would suggest that there may be a genuine individual operator effect on blood transfusion practice.
This study has a range of limitations, such as its observational nature. Also, the data focused only on the impact of the merger on the overall transfusion practice at BHC, and it does not explain if the reduction in blood usage was appropriate or inappropriate, nor does it include details of how these changes impacted on patients’ short- and long-term outcomes. However, considering that clinical staff and surgical treatment of different cardiac procedures remained unchanged during the study period, it is very likely that the reduction in RBC use is appropriate.
A key strength of this study is the use of the purpose built NICOR database and the hospital transfusion electronic system, rather than databases designed for other purposes. This has ensured a high degree of fidelity and has minimised the extent of recall bias. Second, by including all patients who had undergone cardiac surgical procedures in three large hospitals in London, we have avoided introducing selection bias. Thirdly, by comparing different infrastructure transfusion support services on a background of improving clinical practice, we have been able to demonstrate that change in transfusion infrastructure can alter resources (ie blood usage and wastage). Therefore, for policy makers and other institutions in the NHS and worldwide, our results might be of interest. This may be also be useful in the merger of other clinical services
In summary, our findings have identified a range of clinical and organisational factors that have led to improvement in transfusion service impacting a regional specialised service. However, future research and any other clinical improvement projects should focus on reducing variability in transfusion practice between users, as well as testing whether novel strategies and new initiatives such as patient blood management (including, for example, preoperative identification of anaemia and iron supplementation, intraoperative cell salvage and antifibrinolytic use, postoperative point-of-care testing of clotting function and changes in transfusion trigger) can reduce mortality, morbidity and length of stay for cardiac surgery patients. This work highlights the potential for stepwise change and a ‘once in a generation opportunity’ offered by large hospital mergers as well as the importance of capturing complete and quality data sets, prior to and continuously following these events, to ensure demonstrative cost effectiveness and value.
Conflicts of interest
Marie Scully has received grants from Baxter, Baxalta, SHIRE, Alexion, Ablynx and Novartis outside of the submitted work.
Acknowledgment
We would like to acknowledge Ms Christ Doughty for assistance with data collection.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.