
ABSTRACT
Introduction Effective leadership is vital for high-quality healthcare. Despite progress in leadership development for junior doctors, studies reflect perceptions that junior doctors feel underprepared for leadership. This study aims to understand medical students’ perceptions about barriers to effective leadership training and how to mitigate these.
Methods This was a mixed-methods study utilising focus group interviews structured using four trigger questions. Qualitative narrative responses underwent quantitative inductive coding applied by two independent coders. Commonly occurring codes underwent thematic analysis to understand underpinning themes.
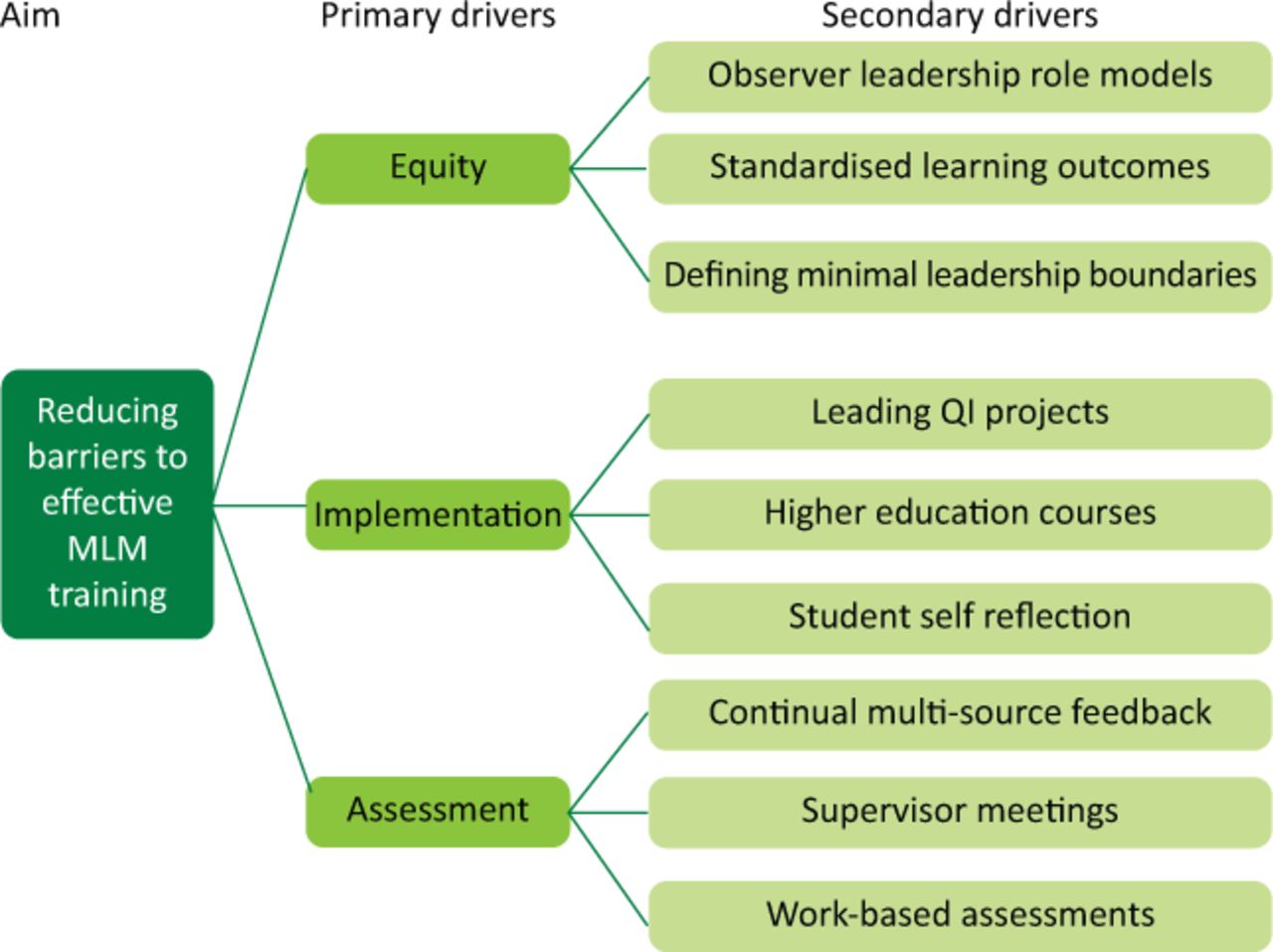
Results Thirty-one students were interviewed from King's College London (n=24) and St George's, University of London (n=7). Cohen's kappa statistic of inter-rater reliability was 0.73. The priority areas were the equity of teaching, implemented approaches and methods of assessing competency. The study presents a driver diagram summarising findings.
Conclusion This study presents medical students’ perceptions about barriers to effective leadership training in current undergraduate curriculum and interventions to mitigate these.
Introduction
To deliver high-quality and safe healthcare, it is pivotal that healthcare organisations ensure effective leadership.1 In a global climate with increasing expectations of stretched healthcare systems, it is becoming increasingly important that doctors working within these systems are able to manage not only clinical but also organisational demands.2 When effective, leadership is shown to improve function at all levels of the healthcare system and it is imperative, irrespective of discipline, for doctors to invest in developing leadership skills.3,4 A growing body of international research further demonstrates that clinician involvement, specifically, in executive decision-making promotes change that is both resource friendly and beneficial for patient care.5
Acknowledging these calls, the Faculty of Medical Leadership and Management (FMLM) have defined guidelines entitled the ‘Medical Leadership Competency Framework’ (MLCF), that all qualified medical professionals must follow. This is well established in postgraduate training where doctors are expected to demonstrate competency in the MLCF domains for career progression.6
However, despite similar efforts being made in leadership development for junior doctors, progress remains slow.7,8 A recent survey of over 1,500 doctors in training found 91% had improvement ideas, but only 11% were able to implement these.9,10 Though multifactorial, this discrepancy reflects a lack of experience in seeing a change through to completion, contributed to by a lack of leadership knowledge and skills.11 To be sure that the doctors of tomorrow are ready to be leaders and enablers of change, educators must train the medical students of today better.
Medical schools are heeding these calls and, to reflect this growing need, are adapting to include teaching of medical leadership skills within their curricula.2 There are formal efforts by the FMLM to introduce standardised curricula with early leadership exposure and structured workplace experiences.12–14 However, at present, there remains no consensus on the optimal methods to implement this teaching with some criticising current teaching as merely ‘tick-box’ exercises that neglects wider cognitive skills required in leadership.15,16
The ultimate goal is to implement a detailed and effective leadership teaching programme that complements existing medical school curricula. This study aims to understand medical students’ perceptions about the barriers to effective leadership training in their current undergraduate curriculum and how they propose that educators can mitigate these.
Method
This mixed-methods study utilised focus group interviews. The qualitative data were coded using a quantitative framework which informed a thematic analysis. This study was completed in a district general hospital in the UK in October 2019.
Focus group interviews
A convenience sample of final-year medical students from St George's, University of London (SGUL) and King's College London (KCL) on clinical placement were invited to attend. Students who attended were informed of the study and signed a register that constituted informed consent. At present, neither school have formal leadership curricula, but KCL are piloting a leadership lecture series set up by a student-run leadership society.
The group interviews were conducted by authors of the study. In order to ensure consistency of discussion between groups, a set of trigger questions were asked to provide a framework for the group interviews.
What barriers prevent you from developing leadership skills?
How is medical leadership taught to you?
How do you think exposure to medical leadership could be improved?
How do you think leadership could be assessed in a medical curriculum?
These questions were constructed in the absence of other validated tools.17 The questions were developed through preliminary pilot testing which showed the questions were reliable, and had face validity in identifying the desired construct within the generated discussion.
Data analysis
Interviews were recorded and transcribed verbatim while maintaining anonymity. Data were then input to NVivo, version 9, (QSR International, Melbourne, Australia). Thereafter three stages of analysis were undertaken.
Familiarisation and coding
Reviewers orientated themselves to content by reading the transcripts and applying codes to the text in an iterative process. The coding framework was orientated around the trigger interview questions.
To ensure validity and reliability of coding, 20% of transcripts were independently coded and inter-coder reliability checks undertaken.18 Kappa statistics were calculated with a value of >0.7 sought for a randomly identified sample. This is consistent with previous studies applying similar methods.19,20 Discrepancies were discussed and when these were not resolved by discussion, third-person arbitration was done by supervisors.
Generation of descriptive summaries
The nature of our inquiry was inductive, therefore exploratory data analysis techniques were applied. The data were described and summarised to inform subsequent hypothesis formation.
Interpretation of themes and learning
The purpose was to deepen the analysis and interpretation gained in stages 1 and 2. Re-examination of these collections of codes provided opportunity to identify overarching themes and context within the data.21 This was continued until thematic saturation was achieved and agreed.
Ethical approval
Ethical approval was not required as this did not divulge patient information nor utilise NHS resources.
Results
A total of 31 students were interviewed from KCL (n=24) and SGUL (n=7) over three 1-hour focus-group sessions. Cohen's kappa statistic of inter-rater (coding) reliability was high, k=0.73 (95% confidence interval (CI) 0.42–0.89). Table 1 describes baseline demographic data of the cohort and Table 2 highlights the most commonly occurring codes that students mentioned for each of the four trigger questions.
Baseline characteristics
Codes applied for responses to each trigger question
What barriers prevent you from developing leadership skills?
A number of perceived barriers were identified which were split into clinical barriers and educational barriers. Concerns around clinical barriers were the discrepancies between teams and sites with regards to student involvement. The degree of support provided to students on placement influenced how readily the students were able to engage and act independently as a team member, and subsequently a leader (n=27). Student F3:
Support is an issue, I don't think in busy hospitals you often have support to practise leadership. So, having a good support structure is important.
If a student encountered a placement where they were given an appropriate level of responsibility and felt actively involved, they perceived to develop skills more rapidly than compared with clinical placements where they were an observer. Student F17:
In medical school you're quite often a passive observer and I think that's where the biggest gap is in stepping up to workplace leadership.
Students reported educational barriers relating to the often overwhelming number of competencies they need to accomplish to progress through the undergraduate curriculum (n=22). The schedule leaves little time in which they can pursue skills like leadership and even less incentive to do so (n=11). Student F4:
Time is stretched for us already with the different things we have to get done. I think there are so many pressures through medical school.
Another perceived educational barrier to medical leadership was a lack of awareness of the topic. Consequently, they did not pursue development as leaders because they did not appreciate a need or use. Their attention was taken by other pressures of medical school which were more apparent in daily study – a factor students felt represented a dearth of leadership teaching in medical curricula. Student M8:
It's really about being aware of it. Even before this session I googled ‘What is medical leadership’.
How is medical leadership taught to you?
The main method by which students received leadership teaching, or rather a teaching experience involving leadership, was through simulations of acute clinical scenarios. This was a commonly stated setting where students perceived gathering leadership experience through leading emergency teams (n=25). However, the absence of formal feedback or assessment on their capabilities specifically as leaders limited this approach. Student F30:
[Leadership is taught] indirectly through simulation because although you get different experiences with simulation, I think we've all had one where you have to take charge ... but then there wasn't specific teaching on leadership itself.
At KCL, students were able to get leadership teaching through a student society (n=10). This was student run and was beneficial for those who were prepared to get this experience in their own time. The society provided teaching and opportunities to practice leadership and management, quality improvement skills, public speaking and to network. Students who had particular interest in leadership would seek teaching externally, but this was a minority (n=5) and, overall, there was perceived a lack of adequate leadership teaching. Student F13:
There are societies like ‘Beyond Med School’. Following the principles form the national healthcare leadership academy programme, they do teaching on practical skills for leadership ... so it's a more all-encompassing programme.
How do you think exposure to medical leadership could be improved?
Some felt it pertinent to incorporate leadership training into current teaching practices, such as simulation by the addition of learning outcomes in leadership domains. However, it was also acknowledged that leadership needs to be valued independently and incorporating it into existing teaching risks diluting the training. Students propose that it would be beneficial for dedicated leadership teaching that is continuous and progressive throughout the year (n=25). Student F1:
It would be good to have a session fortnightly and make it relevant to that clinical stage the students are at. But I think it would be good to have it set aside, rather than mixed with something else.
Another way that students suggest curricula can improve exposure is to introduce leadership-based projects and student-selected components (n=16). Allowing students to undertake a body of work in the field offers potential extra-curricular benefits. As with other projects that students complete (such that result in posters, presentations or publications), leadership projects must offer the same incentives. Student M26:
We already spend time doing quality improvement projects, why couldn't we do a leadership project. I think having a formal project that is recognised by the school would make you stand out and develop personally.
Another recurrent theme for improving their leadership training was defining the boundaries of responsibility on placement for final-year students (n=16). Uncertainty around their limitations as students, when it came to taking opportunities to lead, subsequently meant they often did not feel empowered to take leadership opportunities. Student F29:
I am often unsure when the right time is to develop leadership skills, for example, knowing when to speak up and take charge. Because ultimately you're only a student and you're unsure what is appropriate to actually do.
Students highlighted the importance of final placements as being a crucial time to get real-time feedback so they can learn and amend practice before they qualify. Students who commonly view themselves as passive observers stated that the merits of being empowered to take active roles in managing patients and leadership in general; under suitable guidance, it helps to bridge the gap they currently envisage between being a student and a practicing doctor and further down the line, a leader. Student M6:
If you give more responsibility to medical students in their final year, that would give the people supervising the students a duty to give constructive feedback on what the students did well or not.
How do you think leadership could be assessed in a medical curriculum?
The value of leadership specific assessment was widely agreed (n=30). The general consensus was that written exams are less useful in assessing leadership skills, as there were concerns over the translation from theory to practice. Incorporating leadership as a separate domain in simulation training with constructive feedback after the scenarios was an actionable suggestion for a method in which leadership could be assessed. Student M6:
If it was integrated to clinical teaching, then I think it's important that you get feedback. Because you rarely hear about how you function as a leader it is important to have specific leadership-related feedback.
While this represents specific feedback on singular learning events, a more comprehensive method of assessment can be multi-source feedback (n=20). This can be guided by a clinical supervisor with overview who can discuss development over the course of a placement utilising peer assessment. The concept of multi-source feedback collates multiple sources of constructive feedback over a period of time that can demonstrate a well-rounded valuation of a student's leadership abilities. Student F15:
Supervisors often don't see us every day and rely on team feedback to make sure we are sound, clinically. I don't see why they can't do the same for leadership?
Alongside external assessment, students saw value in self-reported questionnaires on personal development of leadership qualities (n=17). This was suggested as a method by which students could be encouraged to reflect and assessed before and after a time period, such as a clinical placement. Student F18:
Questionnaires measuring confidence in being a leader before and after sessions and with specifically targeted questions would be good. This means, even if we don't get much supervisor guidance we have our own measuring stick of sorts.
Discussion
Studies from over a decade ago suggest faculty and students believed that experiential training was the most effective for teaching leadership skills and that future studies should address optimal methods of teaching and assessing leadership skills among medical students.22 This study builds on this by providing an insight into the barriers that medical students perceived about leadership training, primarily around the equity of teaching, approaches being implemented; and methods of assessing competency. Methodological rigor was ensured by double-coding a random 20% sample of transcripts.18,21 The methodology has also been applied to qualitative data in patient safety research.19,20 We accept that limitations of the sample size and cohort make it difficult to draw widely generalisable conclusions and also, given the absence of similar literature, the trigger questions used are not externally validated. However, the novel methodology of this study provides an insight that can guide further research to test the conclusions drawn. These results demonstrate priority areas that are amenable to improvement through proposed recommendations identified from the literature (Fig 1). To the our knowledge, this is the first study exploring medical student views on barriers to effective leadership education in undergraduate curricula.
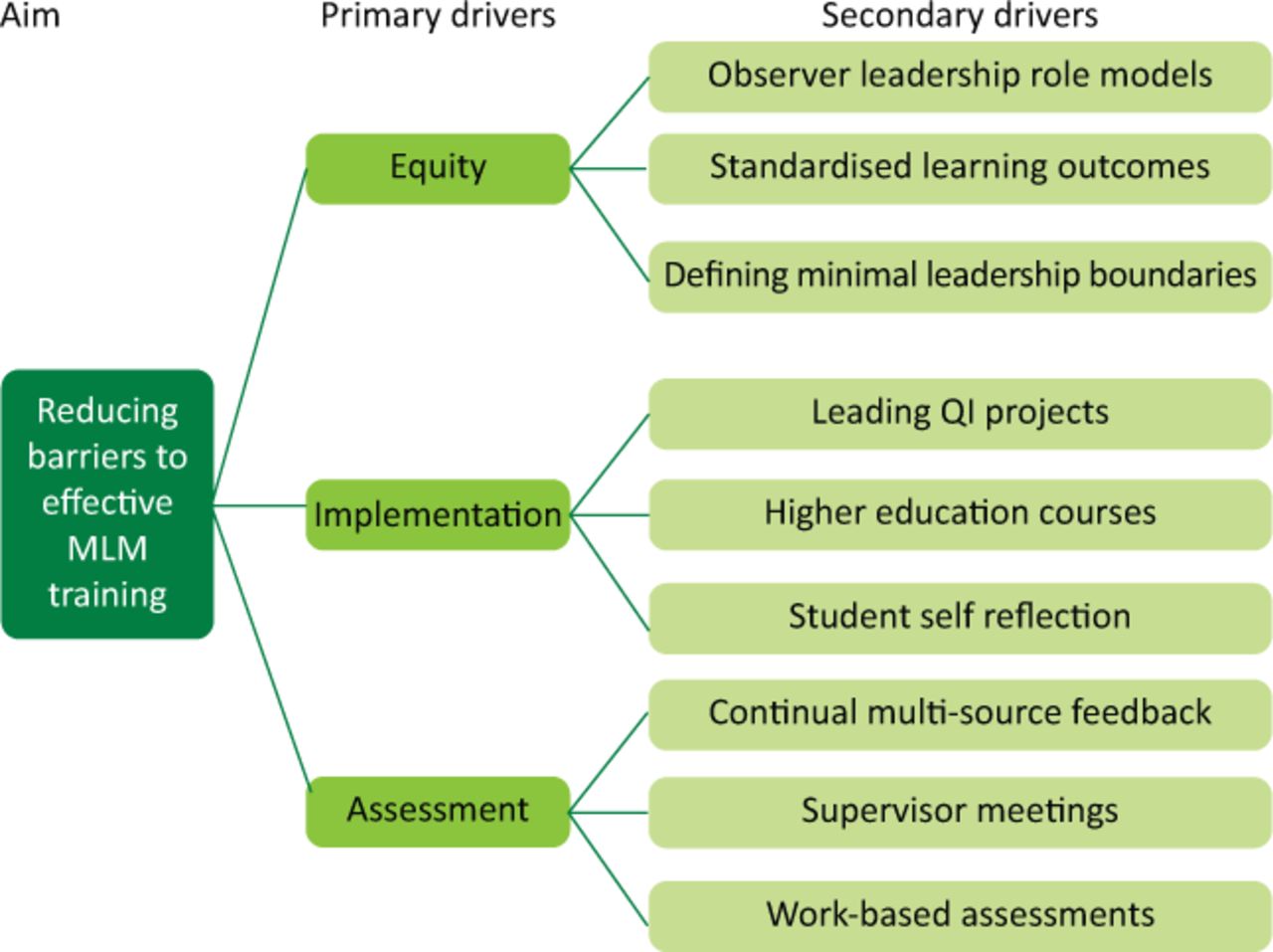
Driver diagram for reducing barriers to medical leadership and management training. MLM = medical leadership and management; QI = quality improvement.
Relation to the literature
Equity
Recent reviews of UK medical schools report that most medical schools teach leadership within the core curriculum but felt they were unable to increase the volume of leadership teaching due to curricular constraints.23 To ensure equity of leadership teaching there must be defined minimal teaching provided for all students. Many schools introduce shadowing periods during clinical placements where students assist the junior doctor whose role they will fill after graduation. The increasing levels of practical experience are important to prepare them for independent practice.24 Applying similar principles, students should have the option to shadow other more senior healthcare leaders such as medical directors or clinical leads.25
These can be implemented within clinical placements when student timetables are often less prescriptive to allow self-directed learning.26 Defining these as a requirement within a placement block will ensure supervising teams are aware of the student's requirements to fulfil this and ensure they are afforded the autonomy and opportunity to undertake this leadership training. Furthermore, following clinical exposure, formal feedback and follow up from trainees, educational/clinical supervisors or personal tutors will reinforce learning but also provide a framework with which students can develop their skills.27–29
At present, few studies have examined the effect of defining a role for medical students but, worldwide, institutions vary in their approach. Some opt for short leadership programmes for senior staff while others incorporate leadership training in their regular curriculum.30 If these could be uniformly implemented early in training, they can begin to develop a pathway for future healthcare leaders.
Implementation
Several systematic reviews have been undertaken in recent times exploring leadership development programmes and the aspects that predict successes.31–33 However, these all arrive at similar conclusions, that training is heterogeneous, and though individual programmes are associated with varying levels of increased self-efficacy, the outcomes on wider system levels remain unclear. This study chooses to discuss interventions to address the areas that the students identified as amenable to improvements for leadership training, namely defined roles, quality improvement (QI) projects and extracurricular study.
In addressing equity of leadership training, defining a role or boundary will facilitate this. It is accepted that the level of skill or competence that final-year students possess will limit the scope of leadership they can safely practice. However, understanding and defining the areas of clinical practice in which they are deemed competent after completing medical school will allow them to begin to lead on aspects of clinical care. Taking lead on tasks such as handing over of patients to the multidisciplinary team, raising patient safety concerns or documenting in medical notes would give students greater ownership of patient care.
An alternative way to ensure competency, other than prescribing a list of tasks to complete, is to set learning outcomes that they can achieve through structured learning and thereafter reflection, supported by an informed supervising team. A review of postgraduate training programmes suggested three key domains to incorporate into clinical placement learning outcomes. These focus on acquisition of skills, such as giving feedback and conflict resolution; technical knowledge; and personal growth and self-awareness.13
QI is defined as ‘better patient experience and outcomes achieved through changing provider behaviour and organisation’.34 Leading QI requires junior doctors to behave as leaders to foster and achieve change.35,36 By giving students skills but also the empowerment to implement improvements to systems improves care while teaching many of skills the MLCF define as important for leadership such as improving services and setting direction. Actively being encouraged to lead change also counteracts a ‘learned helplessness’, which left unchecked causes future disengagement with management.36
For those who wish to develop further, some institutes offer student selected components, intercalated BScs, Masters and PhDs on medical leadership and management. Though higher-level qualifications are offered in only a few institutions, the FMLM are working to establish guidance to enable wider implementation. Other options are national or international leadership fellowship programmes, which in the UK in recent years have grown in popularity.37
The ultimate goal for any leadership training is to ensure patient safety, so that once students are deemed competent, they should be trusted and adequately supervised to take ownership of their clinical roles. The training should also instil a holistic view with the understanding that not all leadership involves widescale organisational change, but rather that students be comfortable and able to lead in the regular and common aspects of clinical care, including workplace structure, functionality and staff wellbeing. Communication, direction setting, reflection, self-awareness etc are such implicit aspects that will continue to be utilised and developed long after students qualify.
Assessment
As with any behavioural capability, there is difficulty in assessing the knowledge-based components. As mentioned, QI, audits and projects lend themselves to experiential practice of skills, but also result in reports or presentations which can be used to assess the learning achieved throughout the programme of work. This potential for academic output is also a motivational factor that can attract students to leadership training.7,38
Peer-feedback or multi-source feedback is a valuable measurement against which students can assess practice. Embedding this early in training teaches them to receive feedback from peers, but also how to give constructive feedback. Alongside this, there must be continual self-reflection that not only guides discussion with tutors but also allows the student to examine and consolidate their own practice. This is a practice that can be encouraged for any clinical situation they encounter and is useful preparation for continued reflection throughout future training.
While continual self- and peer-summative assessments have value, there must be formative assessments of students’ development – to assess progression of attaining competencies over time. It can be difficult to assess leadership skills objectively, but assessors can remedy this by continual summative assessments of competencies through work-based assessments. Another way this can be achieved is through timely appraisals or interviews with senior supervisors.39
Conclusion
Effective leadership is vital to ensure the delivery of safe and high-quality healthcare and this study presents medical students’ perceptions about the barriers to effective leadership training in current undergraduate curriculum and literature proposing how educators can mitigate these. The priority areas focus on the equity of teaching, approaches being implemented and the methods of assessing competency. We hope this work will generate hypotheses which further collaborative study can utilise in development of undergraduate leadership curricula.
Acknowledgements
Thanks to Dr Zainali Panjwani who acted as the second independent coder.
- © Royal College of Physicians 2020. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.