
Introduction
Our integrated sexual health service (ISHS) does not have electronic requesting for sexual health samples. In mid-2019, healthcare assistants (HCAs) reported an increased workload in completing declaration forms, to support the processing of mislabelled samples by the laboratory. If they were unable to be completed, time was spent recalling patients to repeat their sexual health samples, resulting in repeat attendance and patient inconvenience.
Our electronic pathology reporting system confirmed 600 samples were not processed between January and June 2019, affecting 500 patients: approximately 2.5% of all new and re-registered patients.
Upon further analysis, an estimated one-third of non-processed samples resulted in a missed opportunity to test, due to patients not being informed, or not attending repeat appointments. This is a concerning statistic in a city where rates of gonorrhoea and syphilis continue to climb, recognising that delays in diagnosis and treatment can increase the pool of infection within the community.
Our aim was to reduce the number of non-processed samples from our ISHS by 80% within 4 months.
Materials and methods
Pareto analysis of 600 non-processed samples highlighted that >80% were due to labelling error or leaking in transit (Fig 1).

Pareto analysis of reasons why samples were not processed.
Using the Pareto principle, by addressing labelling error and reasons for leaking, we would achieve our biggest improvements. Plan, do, study, act (PDSA) cycle 1 entailed engaging HCAs for improvement ideas regarding labelling, ensuring frontline staff felt supported. We agreed the HCAs would implement a second check of all patient identifiers on samples and request forms. These would then be stamped and initialled by HCAs, prior to transport.
Background data were presented to our ISHS prior to this PDSA, with clinicians being asked to ensure patients screwed sample lids on tightly to reduce the chance of leaking. A standard operating procedure was created.
Results and discussion
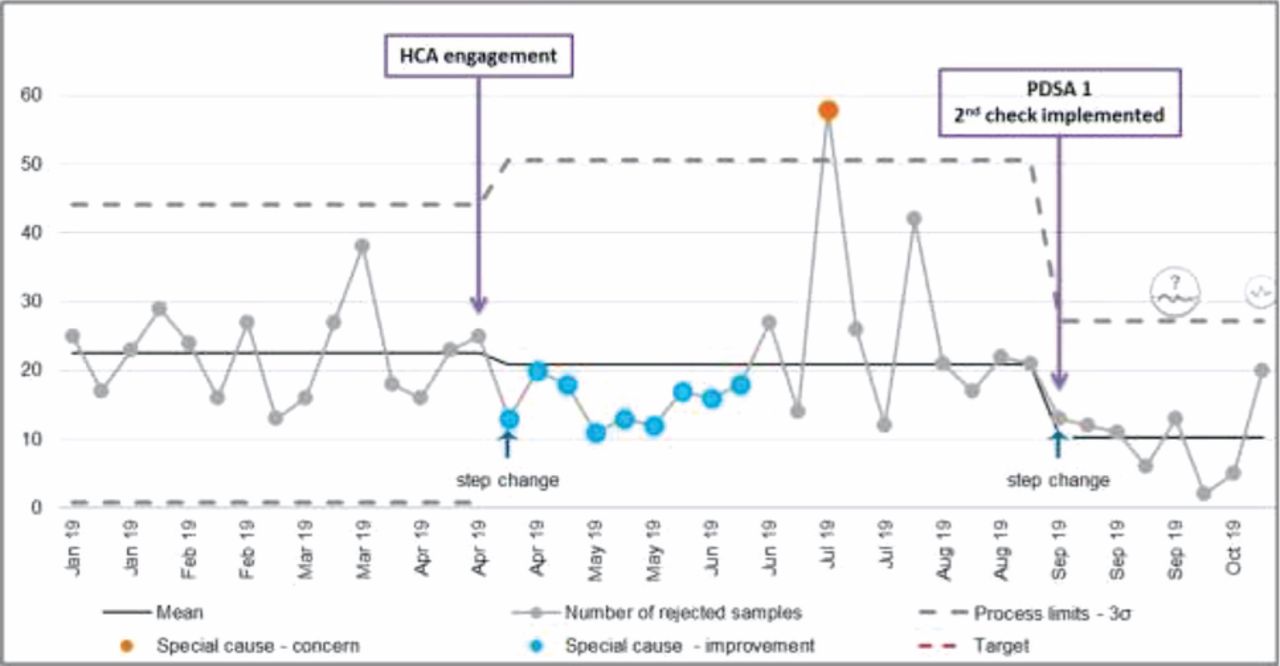
The weekly number of non-processed samples from January 2019 was plotted on a statistical process control (SPC) chart. The mean weekly number of non-processed samples from January to mid-April (baseline period) was 22.5. While highlighting the issue, and engaging staff within the planning stage, there was a significant step reduction in mean from 22.5 to 20.9 (Fig 2).
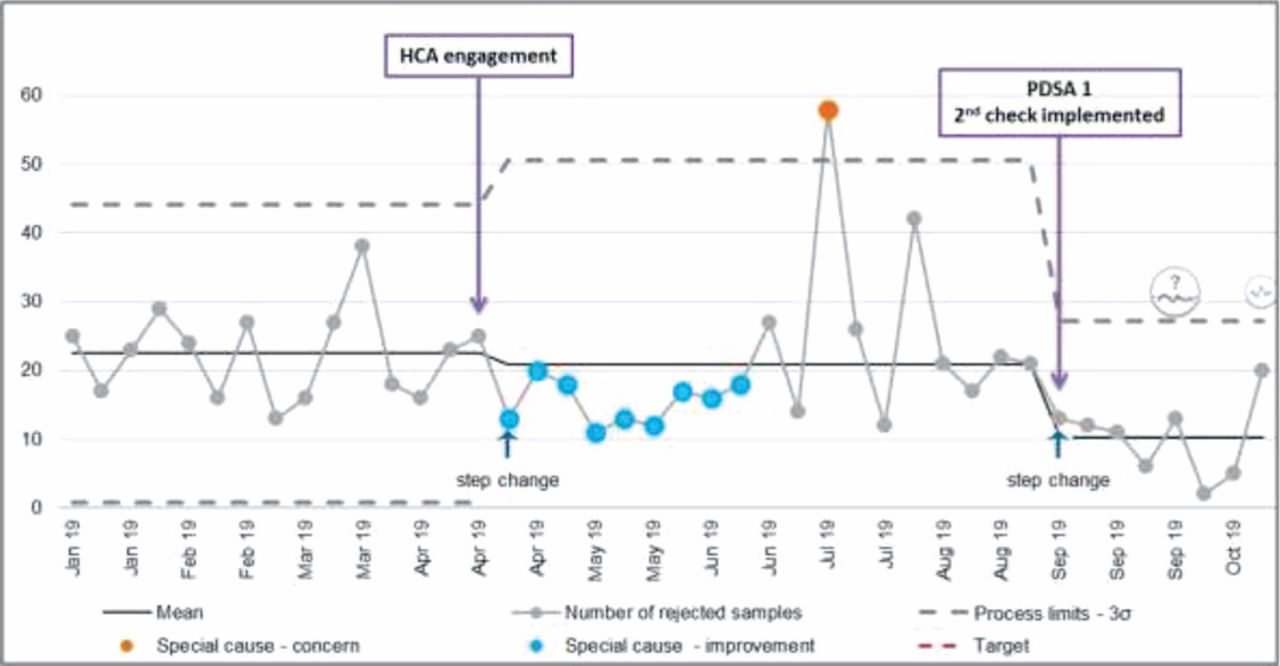
Statistical process chart showing weekly number of non-processed samples.
Upon implementation of the second check on 02 September, we had >7 successive weeks of improvement, creating a step-change and a statistically significant new weekly mean of 10.2. There was a >50% reduction of non-processed within the first two months.
Conclusion
This project shows that engagement of frontline staff enables people to feel empowered to second-check specimens, and be a part of improvement science, enhancing the culture of patient safety within our ISHS.
Further work is ongoing to reach our aim of 80% improvement within 4 months. PDSA cycle 2 includes upscaling the second-check process to five spoke clinics, and quality-assuring leaked samples with the laboratory.
Weekly feedback of data continues to drive improvement. Staff enjoy seeing how small interventions, through PDSA cycles, can improve patient outcomes. They are envisioning how improvement science may be applied to other workstreams within our ISHS.
Conflicts of interest
None declared.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.