
Introduction
Foundation year 1 doctors (F1s) are expected to prescribe from their first day in clinical practice. Prescribing involves a complex series of steps involving integration of theoretical and experiential knowledge, patient information, communication skills, mathematics and awareness of human factors that undermine safe prescribing. It has been suggested that prescribing should routinely be viewed and treated as a high-risk procedural skill.
The majority of prescriptions within secondary care are written by foundation doctors (FDs).1,2 FDs also make the most prescribing errors.2,3 An important part of the transition to prescriber is F1 induction. Since 2012, trusts and health boards must provide an induction and at least 4 days’ shadowing experience to new F1 cohorts before they begin their first post.4 However, there is no standardised F1 induction curriculum and research shows that content, including prescribing-related topics, and format can vary widely.5,6 FDs have themselves highlighted that they find transitioning to practical prescribing challenging and they often feel unprepared.7,8
This study aimed to address a critical knowledge gap: how can we use feedback from FDs to enable the F1 induction period and available resources to support prescribing competency during the first months of practice?
Materials and methods
A survey was designed to obtain information about F1 and F2 doctors’ experiences of preparedness to prescribe following medical school; experiences of prescribing teaching and support during F1 induction; the tools, resources and sources of feedback available to them during their first placement; and views about prescribing error feedback. FD members of the RCP were invited to participate over a 2-month period, with 229 FDs doing so.
Results and discussion
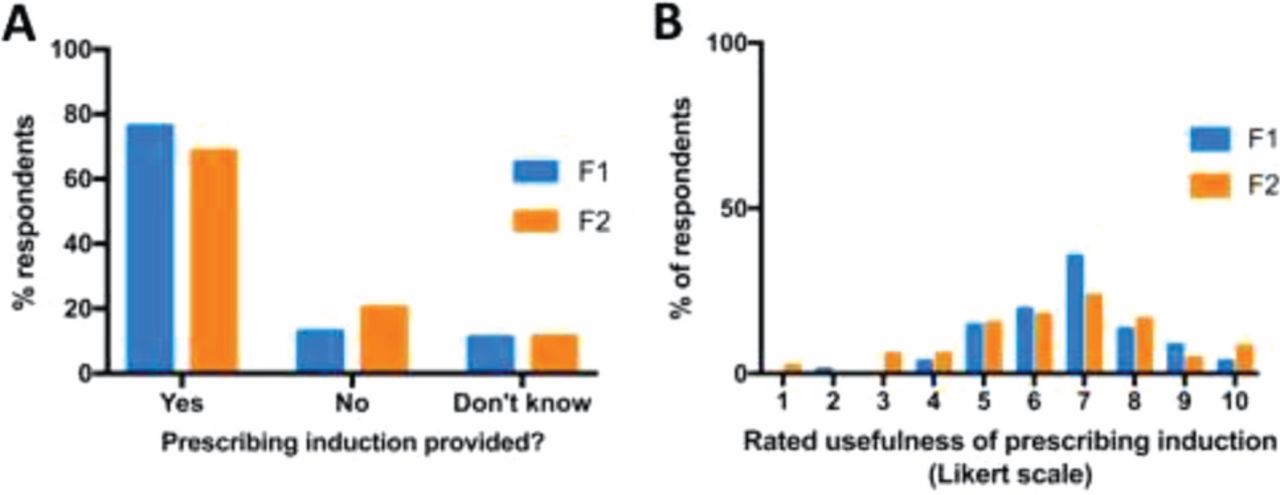
FDs felt moderately prepared for prescribing by medical school. 72% of FDs had received a F1 prescribing induction and had found this moderately useful, although less helpful if delivered several weeks after the start of F1 (Fig 1).
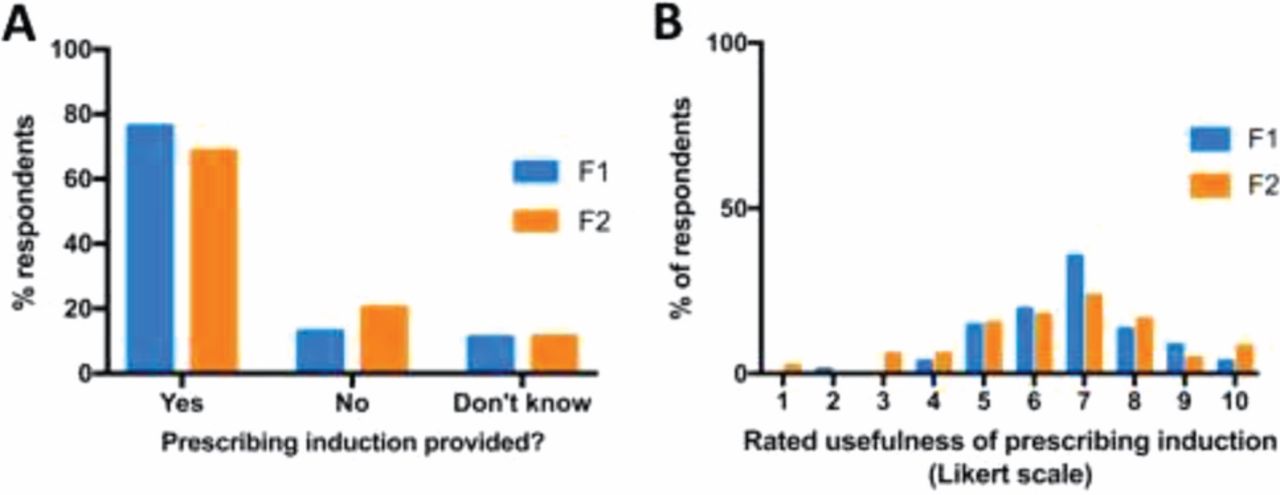
Provision and usefulness of prescribing induction.
FDs overwhelmingly expressed a preference for a neutral tone, and interactive and practical sessions. FDs strongly preferred prescribing induction topics based on common prescribing situations and errors, commonly prescribed drugs and local guidelines (Fig 2). They wished to avoid repetition of concepts covered in medical school.

Foundation doctors’ perceived most useful content to include in a prescribing induction.
FDs found the most useful and accessible prescribing resource was the ward pharmacist (94%), followed by intranet-based prescribing guidelines (82%) and apps (65%). Current prescribing teaching sessions (27%), electronic prescribing safety messages (28%) and prescribing checklists (11%) were deemed less helpful. FDs gave clear reasons for the sources they valued most and least and highlighted unmet needs.
Almost all FDs (97%) found feedback after prescribing errors to be a useful prescribing development tool. The majority of FDs had received feedback, most frequently from a pharmacist.
Conclusion
This study provides insight into how FDs feel the mandatory F1 induction period, support systems and resources could be used more effectively to promote the transition from student observer to prescriber. In particular, they favoured an emphasis on a suite of highly interactive, multimodal development opportunities with close involvement of pharmacists. Using FD feedback to direct refinements of induction-based prescribing teaching and development strategies could provide a mechanism to improve capability, competency and confidence during the new prescriber period.
Conflicts of interest
None declared.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.