
Antimicrobial resistance (AMR) is a critical and worsening public health threat driven by high volumes of use and inappropriate clinical targeting. Ecological studies show an association between antibiotic use and resistance rates. Moderation of antibiotic prescribing requires a deeper understanding of differences in local prescribing behaviours. The purpose of this study was to understand the factors in antibiotic prescribing determined by discretionary choice behaviour that may provide insights into enhanced methods to modify antibiotic usage and control AMR.
Oral antibiotic prescribing information extracted from general practitioner (GP) prescribing data were aggregated by applying WHO Anatomical Therapeutic Chemical Classification (ATC) defined daily doses (DDD). Average annual antibiotic daily prescribing rate (AAADPR) was the sum of DDD of all oral antibiotics in each practice divided by practice population and 365 (days). AAADPR in each GP practice with >2,000 people in England in 2017–18 were linked by regression to other publicly available factors including demographics, geography, medical comorbidities, clinical performance, patient satisfaction, prescribing selection and medical workforce characteristics. Regression coefficients for those modifiable prescribing selection factors were applied to the difference between values for median and top decile practices to establish the overall reduction opportunities through changing prescribing behaviour.
We studied 5,889 practices supporting 49.8 million patients to identify 25 factors accounting for 58% of AAADPR variation between practices (Figs 1 and 2). Factors non-modifiable by the local practice that are linked to increased AAADPR: more northerly location, higher prevalence of diabetes, chronic obstructive pulmonary disease (COPD), coronary heart disease (CHD) and asthma; higher white ethnicity; higher patient satisfaction; and lower population density. However, 11% of the variation in AAADPR can be linked through prescribing behaviour modifiable by the local practice to increased AAADPR, these include wider range of antibiotics prescribed, higher proportion taken as liquids, higher doses in each prescription, lower National Institute for Health and Care Excellence guidelines compliance, lower use of targeted antibiotics, lower spend/dose and less seasonal variation.

2017–18 cross-sectional regression analysis (factors on the left side of the graph relate to less prescribing).
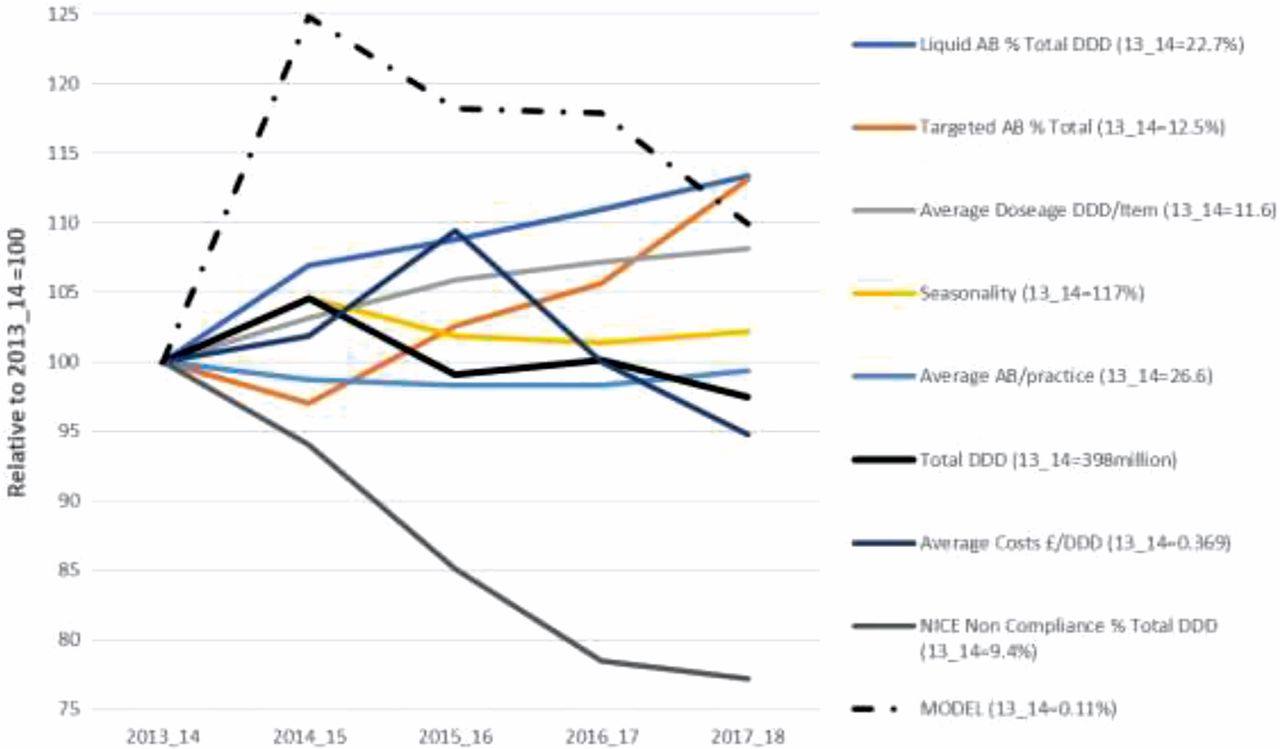
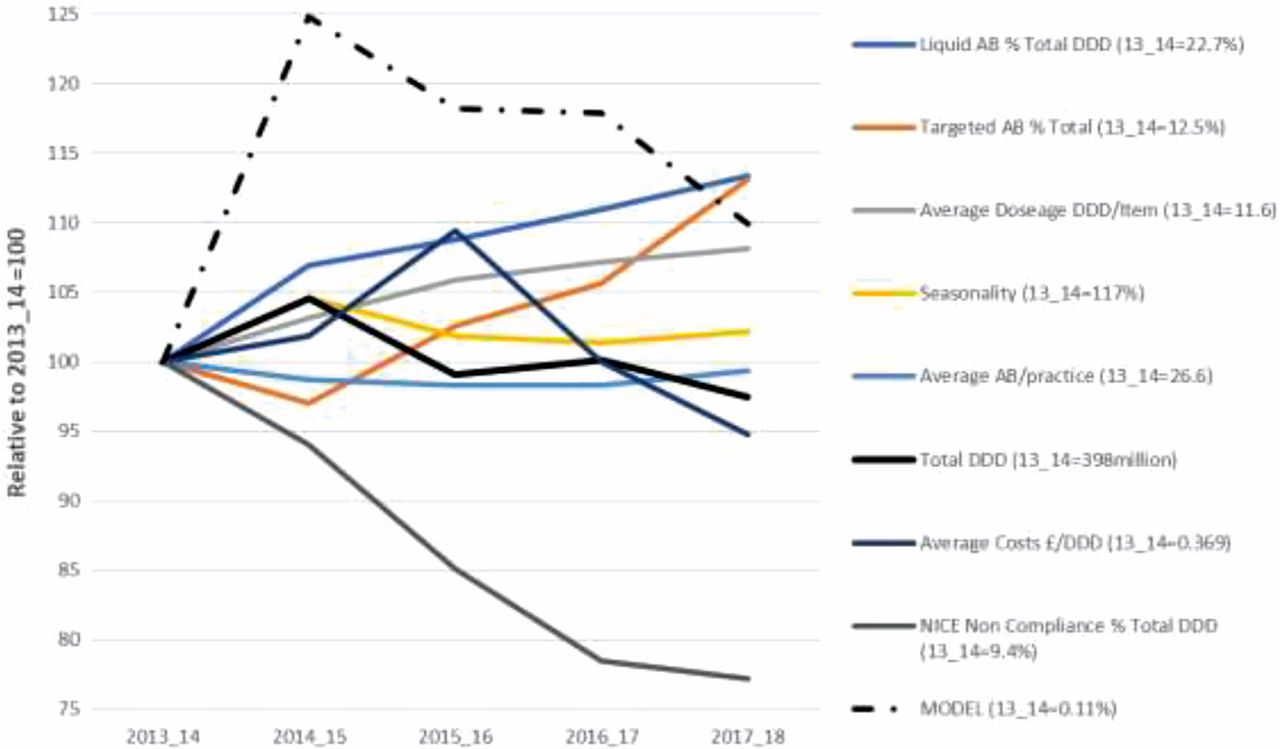
Trend in prescribing factors over last 5 years linked to model regression.
Applying the model to the last 5 years shows that since 14–15 changes in prescribing factors have been reflected in reduction in the overall prescribing. The model also suggests that if all practices achieved the level of prescribing modifiable factors of the top decile practices, the statistical model suggests that overall AAADPR would be reduced by up to a further 31%.
We acknowledge that such analysis cannot infer causation and is ultimately associative in its nature. Demographics, location and medical condition of the population are major drivers in antibiotic prescribing in general practice. However prescribing selection plays a significant role and results from this analysis can provide benchmarks for both the non-modifiable and modifiable factors against which practices could evaluate their opportunities to reduce their antibiotic prescribing.
Conflicts of interest
None declared.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.