
ABSTRACT
The stellar gains in life expectancy and health over the past century have been accompanied by an increase in societal and health inequalities. This health gap between the most and least fortunate in our society is widening, driven by complex social determinants of health, as well as healthcare systems themselves. Physicians are not just well-qualified and well-placed to act as advocates for change, but have a moral duty to do so: to stand by silently is to be complicit.
Following a workshop on health inequalities and medical training at the Royal College of Physicians Trainees Committee, we sought to examine how health inequalities could be addressed through changes to the medical education system. We discuss the arguments for reform in recruitment to medicine, and changes to undergraduate, postgraduate and continuing medical education in order to equip the profession to deliver meaningful improvements in health inequalities. We propose a population health credential as a mechanism by which specialists can gain additional skills to take on leadership roles addressing health inequalities, allowing them to support colleagues in public health and bring in specialty-specific knowledge and experience.
Introduction
The 20th century saw enormous improvements in prosperity, life expectancy and quality of life: the ‘great escape’ from poverty and disease.1 These health benefits have arisen from improved nutrition, water, housing and sanitation, as well as the rapid development of scientific medicine, which has provided us with modern miracles (such as vaccines, antibiotics and insulin). However, health inequalities (HI) within society have increased in parallel. These inequalities do real harm; the World Health Organization (WHO) Commission on Social Determinants of Health (SDH) was not restrained when it declared ‘Social injustice is killing people on a grand scale.’2 The death toll from HI is not limited to poorer nations: inequalities contribute to every major health concern, from diabetes to airways disease, communicable and non-communicable disease, regardless of geography or government.
In the UK, improvements in life expectancy have now plateaued. Social and economic inequalities along with child poverty, both relative and absolute, have increased, with apparent substantial inequalities in life expectancy. Life expectancy is no longer improving for those in our most deprived communities, arguably linked to recent policies of austerity, where the impact was felt hardest in the most deprived communities.3 The economic interests of business sectors (tobacco, alcohol, food and drink, and manufacturing) can come into direct conflict with the priorities for public health, with these commercial determinants of health further exacerbating inequalities.4–5 The COVID-19 pandemic has aggravated financial inequalities, while high levels of deprivation almost double the risk of death from COVID-19.6,7
The case for physicians to address health inequalities
The NHS offers universal healthcare, free at the point of access, and is ranked as highly equitable and accessible in international comparisons.8 Despite this, many of the achievements in disease prevention that have improved life expectancy show marked disparities within our society. Tobacco smoking, alcohol consumption, drug use, vaccination and cancer screening uptake all show variation based on measures of social deprivation.9–13 This demonstrates the continuing effects of the inverse care law, described nearly 50 years ago, which states that: ‘The availability of good medical care tends to vary inversely with the need for it in the population served.’14
As physicians, we accept that our profession has a role in disease prevention, with ‘lifestyle’ modifications, education campaigns, screening and vaccination programmes being our responsibility. Yet, disease is often the manifestation of wider societal issues, and our impact will be diluted without consideration of such factors.
While treatment without prejudice is written into the General Medical Council's (GMC) Good medical practice and the ‘modern Hippocratic Oath’ (Declaration of Geneva), both documents state no obligation to address inequalities in health, or the social determinants that underpin them.15,16 The widening health inequalities in our society, despite the many successes in modern medicine, is justification that this bystander approach is inadequate. It abdicates responsibility for the ‘causes of the causes’ of disease to others. As Don Berwick has written: ‘To try to avoid the political fray through silence is impossible, because silence is now political. Either engage or assist the harm. There is no third choice.’17
Even if we should, can we, as physicians, effect meaningful change in this arena? We strongly believe so, and that the benefits of such an approach would be felt widely. As Rudolf Virchow stated in 1848: ‘Medicine is a social science, and politics nothing but medicine at a larger scale.’18
Physicians as advocates
Doctors are well-placed to be powerful and influential advocates for change in healthcare and wider society, to become Virchow's ‘natural attorneys of the poor’.18 We are highly trusted by the public, possess relevant expertise, and physicians are increasingly interested and engaged in civic and political matters.19,20 Royal colleges and other professional bodies have increasing political influence, whether they seek or use that influence or not. In addition, we have seen the increasing role of physician-activists, such as the ‘#ThisIsOurLane’ movement addressing gun control in the USA.21 The importance of robust physician advocacy within wider society has been brought home in the COVID-19 pandemic, where key voices in healthcare have shaped the societal narrative of the pandemic, and sought to address common misunderstandings of the public.
Altruism and social justice are the motivations that attract many to the profession, but while the vast majority of doctors believe activism on health-related issues is important, most do not participate.22 Whether familiarity and exposure to the consequences of health inequalities normalises them to some physicians, or whether a lack of skills and opportunity limit their ability to remain advocates for societal change, is unclear.23 However, the sense of powerlessness to address causes of ill-health beyond the clinic is a driver for moral injury and physician burnout.24,25 The case for greater physician involvement in tackling HI and their underlying social determinants is clear. How then, do we equip the profession with the skills and attributes required to achieve this?
Medical student selection: doctors should represent the society in which they work
For medical professionals to represent the diverse communities they serve, individuals should be drawn from them. Currently, medical students do not fully represent the wider society from which they are recruited. Students from Black heritage are underrepresented compared with the wider population, as are those from the most deprived communities, and the state education system.26,27 This inequity raises a wider question of how to ‘level’ the playing field, without reducing the standards expected of successful applicants.
There are barriers to medical school entry for those from particular backgrounds, related to socioeconomic status, ethnicity and region. Medical school entry is competitive, and rightly so; those who join the medical profession need the ability and vocation for what is a long and hard career. However, stringent exam selection criteria can become barriers in themselves, and are problematic when viewed though a lens of social mobility and addressing SDH/HI. Recent research has proposed reducing academic entry criteria from candidates from poorly-performing secondary schools by one to two A-level grades.28 Requirements for work experience placements and medical school selection criteria based on extra-curricular activities can favour applicants from higher-performing schools, particularly those with ample opportunities in sport, music and drama, or applicants from families that benefit from contacts and networks. Widening access to medical school (WAMS) initiatives at medical schools (including summer schools, work experience, differential entry criteria and extended foundation courses) can help tackle these barriers to medical school entry (see examples in Table 1). Beyond admission, students require ongoing support to address potential attainment gaps during medical school. Research experiences, publications and positions of responsibility (the criteria upon which postgraduate selection hang) are more challenging to achieve for those whose financial position precludes an intercalated degree or requires additional employment.41
Reforms to medical education and training to address health inequalities and the social determinants of health
Doctors are not equally distributed throughout the UK, with some regions ‘under-doctored’ per head of population. Unfortunately, the distribution of medical schools and doctors in training mirrors this disparity, further entrenching these regional inequalities.42 Indeed, the NHS as a whole is under-doctored, and regional and socioeconomic disparities should be a key determinant in where additional medical school places, and new medical schools, are created, as was the case in the last expansion in medical schools in 2018.43–45
The undergraduate curriculum: health inequalities as a lens, not a module
The GMC states that: ‘Newly qualified doctors must be able to apply social science principles, methods and knowledge to medical practice and integrate these into patient care.’46 Some medical schools include specific modules on this topic, an approach espoused by the Working for health equity report, and consensus core learning outcomes has been developed with medical schools and royal colleges.47,48 However, social determinants of health and health inequalities should not be a bolt-on module to add to a curriculum, but a lens through which medicine is viewed.
Indeed, when isolated from the rest of medical training, its theoretical framework can be dry and feel remote; a problem too large and nebulous to tackle. Learning about health inequalities and SDH should be a continuous vertical strand in undergraduate medical education, involving both theoretical and experiential learning.
Theoretical training will raise an awareness of HI issues, but students may need to witness and experience HI in the real world to truly appreciate its impact. Many entering medical school have limited experience of how those from different backgrounds live their lives, and what constrains their ability to access healthcare or make healthy lifestyle choices. Expanding the horizons of medical students through exposure to those in such situations is best achieved through hearing and seeing the lived experiences of our patients; for instance, why a patient with occupational asthma would not attend mid-week appointments due to threat of unemployment, or not change jobs as poor literacy limits their employment opportunities. Many described models of teaching SDH/HI include experiential learning as an instructional strategy.49 Opportunities for this learning do exist in secondary care and SDH/HI learning should be integrated throughout subject- and specialty-specific modules. In addition, primary care, as well as in allied services, provides excellent opportunities for students to gain a window into the lives of others and insight into their experiences.
Previous reports have argued that learning for SDH/HI should be formally assessed, however, such topics create a challenge for assessment, and are often unexamined.49,50 Assessment drives learning, and avoiding any assessment in SDH/HI inadvertently sends a message to students that such content is of lesser importance. Conversely, by protecting learners from assessment, exploration of the topics driven by interest and curiosity of learners may be encouraged. Learning may be best assessed through reflective practice, essays and narratives, rather than multiple-choice questions; while the latter has allowed for standardisation of examinations, it contributes to a narrowing of educational focus from the complexities of the art of medicine inherent in this area.
There is also a wider, more nebulous curriculum that perhaps medical schools should seek to touch upon. The principles of addressing SDH and HI are fundamentally philosophical, ethical and political; for they are predicated on the judgements about what we value, both as a profession and as a society. Perhaps aspects of ethics, history, politics, advocacy and humanities, often side-lined to special study modules in the increasingly hectic medical curriculum, need to become a greater focus. Health inequalities associated with ethnicity and race, associated with profound mistrust of healthcare systems within some communities, can only be understood through acknowledgement of the impact of colonialism, historical abuses (eg Tuskegee, Sims and Lacks), and ongoing racism in our society.51 Medical humanities, including fiction reading and writing, can develop cultural competence, and insight into patient experience.52,53
Medical schools are constantly required to ‘modernise’ and expand an ever-congested curriculum, while protecting the teaching of traditional core clinical skills and knowledge required for the safe practice of new doctors. Some call for the undergraduate medical curriculum to remain focused solely on knowledge-based teaching, and that extraneous elements detract from training safe doctors.54 This presumes that medical school training is a zero-sum game; that a day spent learning about SDH/HI means a day less training in electrocardiography interpretation or prescribing. Knowledge and skill are not independent and, indeed, additional perspectives aid learning. Some dispute the assertion that SDH/HI is the responsibility of a doctor (as outlined previously). Finally, the purpose of undergraduate medical training is not just to train a competent foundation year-1 doctor, but to establish the foundations from which an individual's personal development and professional career may flourish. In essence, SDH/HI is a cornerstone of that foundational learning.
The postgraduate curriculum and career trajectories
While undergraduate medical education aims to equip students for a career as a doctor, postgraduate (PG) education trains doctors for work in particular specialties and must be grounded in action. Therefore, PG curricula in SDH/HI must be framed within the context of an individual doctor's career intentions and their chosen specialty; it is disingenuous to suggest that SDH/HI training for a doctor in respiratory medicine will be the same as for a histopathologist, a hand surgeon or an intensive care physician. Creating ‘one size fits all’ courses is likely to have a deleterious effect, consigning SDH/HI to the list of mandated courses of limited practical significance.
Indeed, there is a risk that knowledge of SDH/HI is considered to be everyone's and, therefore, no one's responsibility, a nebulous challenge too large for any individual physician to tackle. To mitigate against this risk, SDH/HI learning at the postgraduate level must be woven into the precise needs of each specialty and sub-specialty if it is to have a meaningful impact. It is, therefore, worthwhile to step back and consider what roles and responsibility that a consultant physician might have, and consider the skills and attributes related to SDH/HI that the consultant would need to develop.
Five domains of responsibility have previously been conceptualised as domains of obligation and aspiration concerning healthcare.22 These move from an individual focus on safe care for the single patient, to responsibilities to address socioeconomic drivers of health inequality, and global health. We have applied this model to UK practice, and considered the responsibilities and obligations of physicians and the systems in which they work for these. In this model, physicians have varied roles within the healthcare structure, with differing educational needs to support this (Fig 1).22 These responsibilities shift from individual clinicians to services, healthcare organisations, national healthcare systems and government. Physicians have roles at several levels, with most clinicians focusing on direct patient care and the development of services. Local service leaders have responsibilities to ensure equitable access and attempt to address some direct SDH. Population health leads would have population health responsibilities in their specialty, ensuring fair and equitable distribution of resources, including to interventions targeting broader SDH.
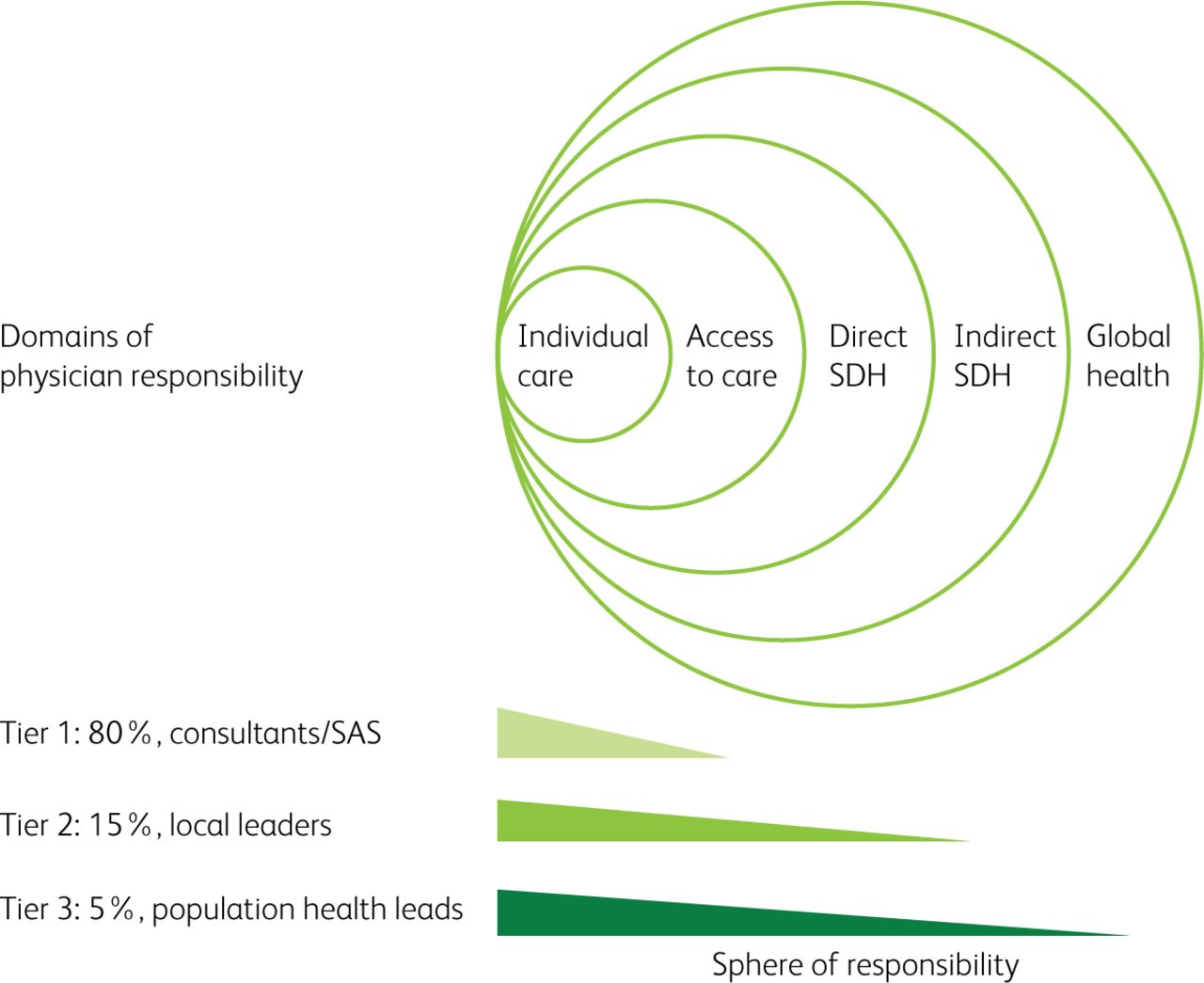
A model of physician responsibilities for domains of the influences on health and inequalities. SAS = specialty, associate specialist and staff grade doctors; SDH = social determinants of health.
For most practicing physicians (tier 1 in our model), their daily responsibilities focus on the patient in front of them and the design and delivery of the services in which they work. They should be skilled in advanced consultation skills to aid behaviour change and should understand the local services available to help their patients address their personal social determinants of health.
For those in leadership positions (managing services and overseeing departments), additional responsibilities for health inequalities rest on their shoulders (tier 2). The structures of healthcare services may inadvertently discriminate against those from more deprived communities, such as through language exclusion in written information or consultations, or digital exclusion through the rollout of telemedicine services. Departmental and service leaders have a responsibility to collect data on health inequalities affecting their patient population and lead quality improvement to address these. They also will have responsibilities to ensure their service integrates into the wider landscape of health services, particularly services which have shared priorities in preventative interventions (such as smoking cessation or reduction in alcohol harm). Physicians with tier 2 responsibilities have additional learning needs related to SDH/HI. Again, as for postgraduate education, such learning should be targeted to the practicalities of the relevant specialty, and may be best led by specialist societies, supported by royal colleges.
Responsibilities for regional and population level health outcomes, and the inequalities therein, are split between organisations and specialties. Indeed, the very structure of medicine, where care and responsibility are fractured between primary and secondary care and public health, seems almost perfectly designed to prevent joined up population health. However, the drive towards integrated care systems, where a single organisation is responsible for primary and secondary care and public health, offers a realistic opportunity to achieve a population health perspective that ensures value and equity. In such a system, each specialty will need to ensure fair distribution of resources within their sphere and be responsible for identifying and addressing inequalities.
This approach will need physicians with a specialist interest in population health approaches and health inequality (tier 3). It is disingenuous to assume that public health physicians have either the capacity, or the specialty-specific knowledge, to address these issues at the specialty and regional level. Specialty physicians with a particular interest in population health and inequalities will be required; such an interest should be an attractive, planned and supported career trajectory, much like leadership, teaching or research. Given the cross-specialty nature of such roles, innovative training approaches are needed, and a ‘credential’ qualification in population health and inequalities could be an approach to formalise this. Such work may also involve public bodies outside of healthcare, which, under the Well-being of Future Generations (Wales) Act 2015 and similar legislation under consideration in parliament, have responsibilities to societal well-being, inequalities and sustainable development.55
Cautions and caveats
The proposals outlined above are not without risk. The evidence for interventions targeting SDH/HI are materially different from those used for many therapeutic strategies in medicine, without randomised controlled trials to highlight the way. It is, then, unsurprising that there is disagreement on whether addressing SDH and HI is an obligation of the medical profession, or an aspiration. Many will, with some justification, argue that we should focus solely on clinical excellence in the care of the individual patient, rather than addressing society's ills, particularly in training. These opinions may differ between some practising physicians and those who engage in medical representation, politics and activism, potentially driving discord between physicians and those who represent them.56
Improving the capability of the profession to address issues of population health and health inequalities will only bear fruit if those physicians work within a system that allows them to use their skills. Breaking down barriers between the silos of primary and secondary care, and leveraging integrated care systems as a tool to ensure accountability for equity and fairness in healthcare resource allocation, will be of prime importance. These changes to healthcare systems and training require funding, support and action; we cannot repeat the cycle of report after report and expect change.57
Conclusion
Physicians have a duty to tackle the widening health inequalities in our society. The profession should resemble the populations that it serves, and we must address the barriers to medical school entry that prevent this at present. Health inequalities need to be a core, vertical thread in medical school curricula, with theoretical and experiential learning assessed and given equal priority to other components. In postgraduate education, learning about SDH/HI must be integrated into individual specialty curricula, and must be focused on practical skills for consultancy. Formalised career paths for those with an interest in health inequalities and population health should be developed, which could be supported by a credential in population health and inequalities. In combination with structural changes in healthcare systems in order to break down professional silos and ensure clear lines of responsibility for inequalities, we may be able to live up to Virchow's cri de guerre.
Acknowledgements
The concept for this work, and many of the ideas and themes within it, came from a workshop held by the Royal College of Physicians Trainees’ Committee. We thank the members of the committee for their contribution. We thank the reviewers for their perceptive and constructive comments on the manuscript.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
Jump to section
- Article
- ABSTRACT
- Introduction
- The case for physicians to address health inequalities
- Physicians as advocates
- Medical student selection: doctors should represent the society in which they work
- The undergraduate curriculum: health inequalities as a lens, not a module
- The postgraduate curriculum and career trajectories
- Cautions and caveats
- Conclusion
- Acknowledgements
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.