
ABSTRACT
Despite huge advances in vaccines, testing and treatments for COVID-19, there is negligible evidence on the perceptions of people hospitalised with COVID-19 about the care they received.
To address this, we developed a satisfaction survey for people with COVID-19 admitted to our hospital during the first COVID-19 wave in Liverpool. Of those invited, 98/160 (61%) responded, of whom 94/98 (96%) completed the survey. Respondents rated overall care highly (mean 4.7/5) and 89/94 (95%) reported that they would recommend the hospital to friends and/or family. Most respondents felt safe on the ward (94%), with privacy maintained (93%) and pain well managed (90%). Fewer than two-thirds (63%) of respondents considered themselves adequately consulted regarding medications and side effects. Sleep and food/drink quality were also highlighted as areas for improvement.
To overcome the issues raised, we generated a ‘COVID-19 practice pointers’ poster within an integrated educational bundle on COVID-19 wards.
The impact of the bundle on perceptions of people hospitalised with COVID-19 will be evaluated in people hospitalised with COVID-19 in Liverpool in 2021. Whether hospitalised for COVID-19 or other conditions, our survey results are a timely reminder of the importance of involving patients in shaping the care that they receive.
Introduction
Approximately 15% of people with COVID-19, the disease caused by SARS-CoV-2, require hospital care.1 In the UK, more than 408,000 people with COVID-19 have been hospitalised.2
Despite huge advances in the understanding of COVID-19,3 the perspectives of people hospitalised with COVID-19 have received scant attention.4 This is concerning given limited NHS capacity, restrictions on hospital visiting and associated in-hospital morbidity and mortality.
We conducted a quality improvement project (QIP) involving a satisfaction survey of people hospitalised with COVID-19 in Liverpool. Here, we describe the implementation methods used so that they could be replicated by other units or hospitals, review the survey responses, and recommend interventions to enhance patient-centred care.
Methods
Design
A cross-sectional survey.
Inclusion criteria
People admitted to Liverpool University Hospitals NHS Foundation Trust (LUHFT) with virologically confirmed and/or clinically suspected COVID-19 (eg consistent radiological findings) were eligible to participate. Virological confirmation was by PCR on upper (eg nasopharyngeal swab) and/or lower (eg sputum) respiratory tract samples.
Exclusion criteria
People with COVID-19 who were receiving non-invasive or mechanical ventilation at the time of enrolment, lacked capacity, or did not give verbal consent to participate were excluded.
Survey
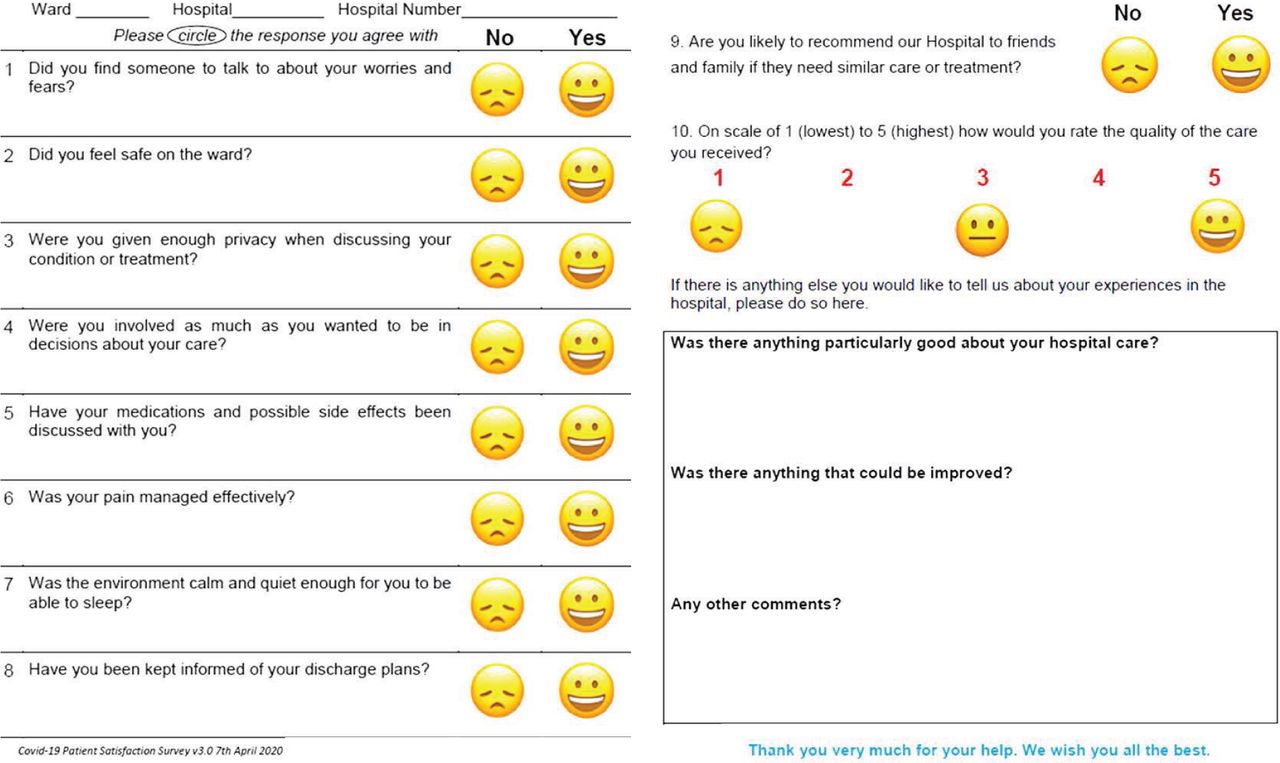
A pre-existing satisfaction survey was combined with a ‘friends and family’ question to form an adapted COVID-19 patient satisfaction survey (Fig 1). The survey questions covered topics including safety, privacy, medications (including analgesia), sleep and communication. There were also free-text questions about positive experiences and areas for improvement.
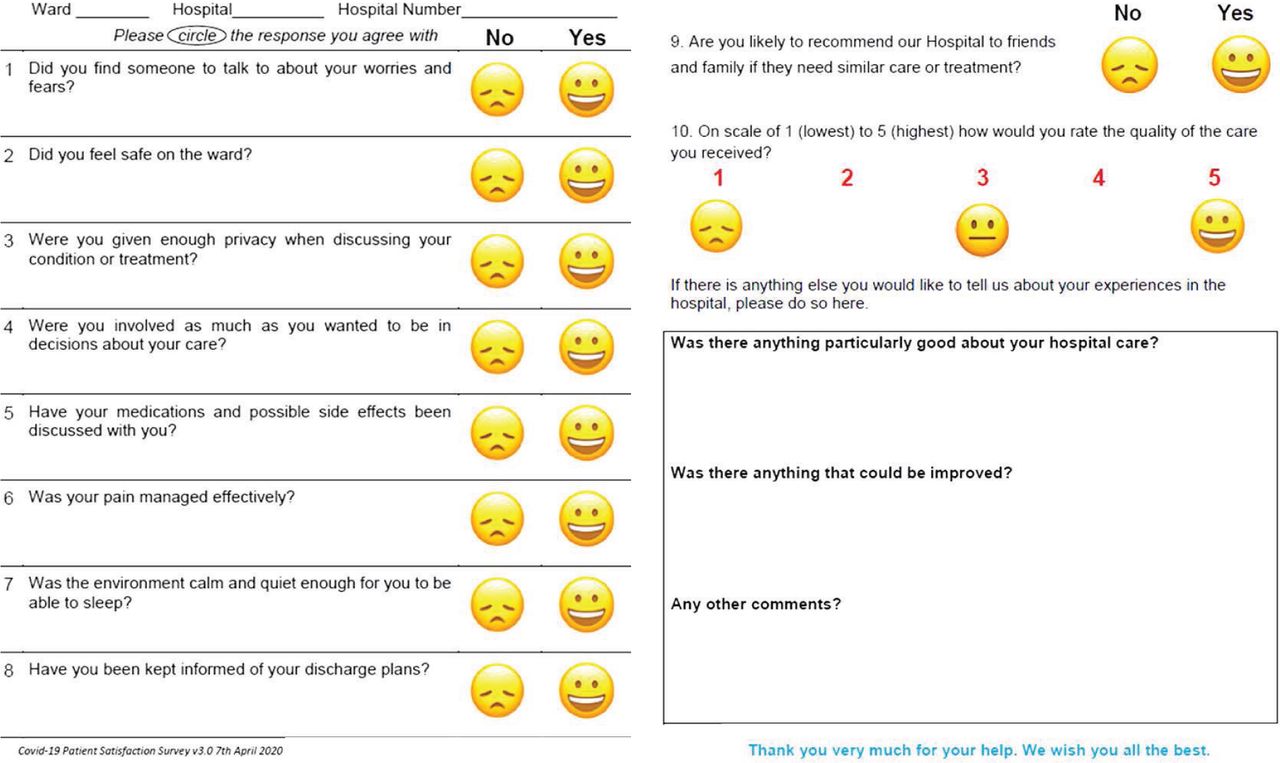
COVID-19 satisfaction survey.
The survey was reviewed by the ‘patient and family experience’ and ‘communications’ departments at LUHFT, and certified as learning disability friendly. A patient survey app facilitated tablet-based data collection, favoured for infection prevention and control (IPC), but a paper survey was offered as an alternative. A standard operating procedure (SOP) was created that gave implementation details in keeping with infection prevention principles (see supplementary material S1).
Recruitment
Recruitment was intended to be systematic with surveys conducted pre-discharge. However, due to heavy clinical commitments and rapid turnover, some participants completed surveys post-discharge. Potential participants were approached by trained students and doctors pre-discharge or contacted by letter or telephone post-discharge. Families, carers and ward staff were permitted to assist completion where required, including by phone or video call.
Approvals
The QIP was first reviewed by the infectious diseases multidisciplinary team and subsequently approved by the local clinical effectiveness department.
Period of implementation
15 March – 15 June 2020.
Analysis
Anonymised responses were transcribed to a password-protected server. Quantitative analyses summarised mean feedback scores and qualitative analysis categorised free-text responses in each domain of care identified by respondents, including safety, wellbeing, food/drink, personal hygiene and communication. This was an opportunistic QIP and no specific sample size was required.
Results
A total of 98/160 (61%) responses were received, of which 72/98 (77%) were completed post-discharge. The sociodemographic and clinical characteristics of 94/98 (96%) of respondents who provided complete survey responses are shown in Table 1.
Sociodemographic and clinical details of people hospitalised with COVID-19
COVID-19 was confirmed in 87/94 (93%) by positive viral PCR and the remainder met clinical criteria for suspected COVID-19 Median respondent age was 59 years and 49/94 (52%) were male. One-third (31/94, 33%) were ex-smokers or smokers. Over one-third (32/84, 38%) of participants were obese and 10/94 (11%) were black, Asian and minority ethnic (BAME). Most participants (73/94, 78%) had one or more comorbidities, with chronic lung disease (38%), hypertension (31%), diabetes (19%) and vasculopathy (16%) predominating.
The average rating of the quality of care received was 4.7/5 and the majority of respondents (89/94, 95%) reported that they would recommend LUHFT to their friends or family (Fig 2). More than 4 in 5 respondents reported that they felt safe during their stay, they were kept informed of discharge plans, they were involved in decision making relating to their care, their privacy was maintained and their pain was managed appropriately. Being able to share worries and fears (78%), sleep quality (77%) and information about medications and side effects (63%) received lower satisfaction scores (Fig 2).
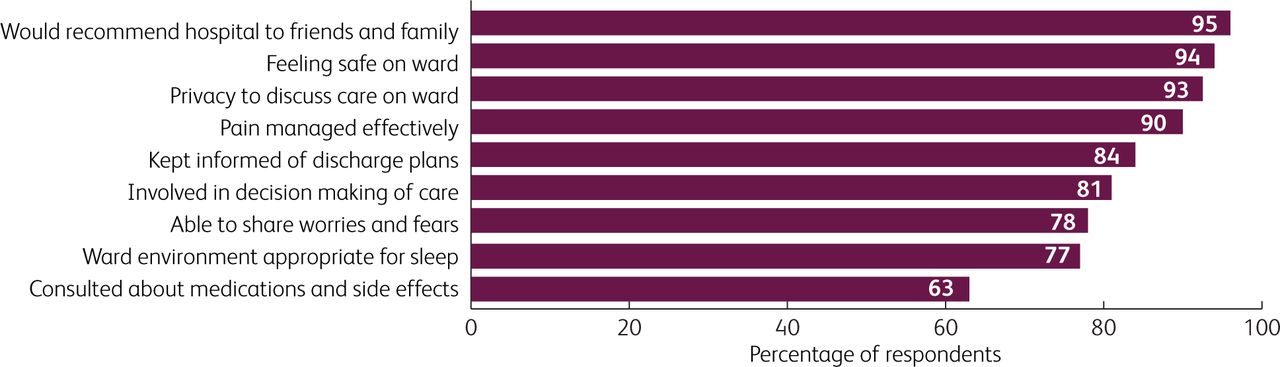
Quantitative feedback from people hospitalised with COVID-19 about their care (n=94).
Free-text responses suggested that medical and nursing care was highly praised, whereas quality of food and drink, and sleep environment were areas for improvement (Table 2). Bilateral communication issues were raised, with one hearing-impaired respondent reporting struggles to communicate when face masks were worn. Other respondents mentioned inadequate or inappropriately timed communication relating to their care (Table 2).
Free-text responses of people with COVID-19 (n=94) on aspects of care that were positive and those that could be improved
Discussion
The COVID-19 pandemic has distorted the healthcare system and eroded processes aimed at improving patient care. Scant attention has been paid to patient involvement in shaping services and holistic healthcare provision, including suspension of routine patient feedback surveys and engagement activities.4,5,6
To our knowledge, this is the first peer-reviewed report of the perceptions of people hospitalised with COVID-19 on the care they received in a UK hospital. The QIP methods we describe, including details of the SOP and survey itself, are low-cost, pragmatic and open access so that they can be replicated by other units or hospitals.
Our survey showed that people with COVID-19 rated the quality of care they received highly, particularly from medical and nursing staff. The majority of respondents reported that they would recommend LUHFT to friends and family. These results are in line with other settings7 and are encouraging, given COVID-19 pressures on the NHS. The results are also in keeping with previous evidence that positive patient experiences are strongly influenced by confidence in care providers.5 The key area for improvement recommended by respondents was communication, especially related to medications and their side effects.
Regular, open, bilateral communication about medications and side effects – including novel therapeutics being evaluated by ongoing randomised controlled trials – is highly relevant to all patients in hospital, especially underserved groups, and not only those with COVID-19. Importantly, the survey revealed that communication issues were further compounded by mask-wearing.
Universal mask-wearing among healthcare workers has positive impacts on reducing nosocomial SARS-CoV-2 transmission in both staff and patients.8 However, there are negative effects of personal protective equipment (PPE), including depersonalisation and fear.9 Older patients in particular may experience heightened anxiety or low mood in COVID-19 wards due to isolation, suboptimal communication or direct COVID-19 neurological effects.10
Patients have been shown to perceive that doctors with face masks have a lower degree of empathy than those without.10 Moreover, people hospitalised with COVID-19, especially if hearing impaired, may have difficulties understanding healthcare workers and communicating their own needs. This should be taken into consideration and mask-windowing adaptations, increased speaking volume and visual aids should be used when needed. This is vitally important, especially for vulnerable patients, and pertinent given ongoing recruitment into studies trialling novel therapeutic agents.
Other key areas for improvement identified by respondents were poor food, drink and sleep quality – areas highly relevant to all hospitalised people, regardless of illness.
Respondents were generally complementary about domestic and cooking staff. However, locally, kitchen staff were also affected by sickness and understaffing, and supply chain issues meant that, at some times, menu choice was more constricted than normal.
Overnight noise levels mean that poor sleep quality is a persistent issue in hospital. Being admitted with COVID-19 is stressful, especially given media coverage and hospital closure to visitors. Sleep is vital for good health and wellbeing, and good sleep quality can contribute to reducing anxiety.11 Potential solutions to poor sleep quality identified include noise monitoring, staff reminders to reduce noise during ‘protected sleeping time’ and single-occupancy rooms. However, these solutions may be hard to achieve when hospitals are working at or over capacity.
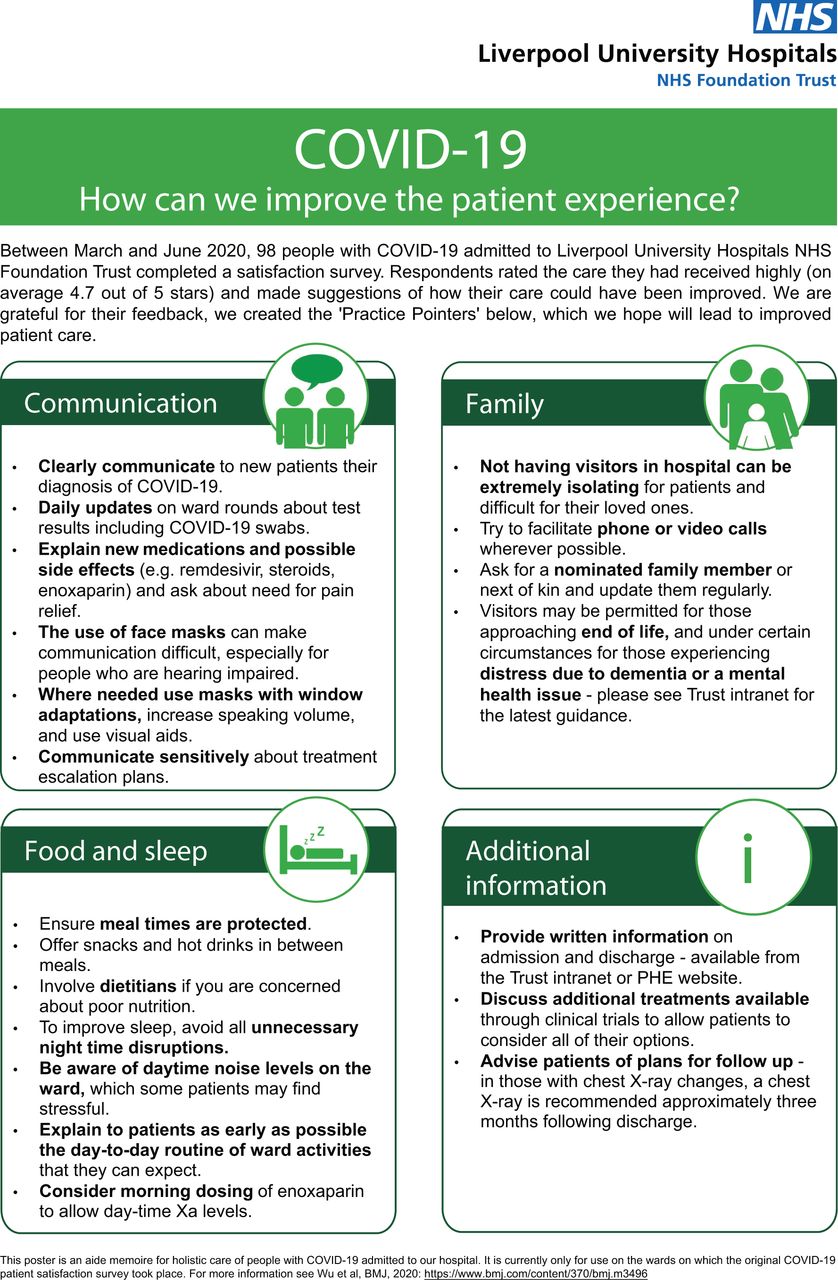
In response to the feedback findings, we generated a poster of ‘COVID-19 practice pointers’ on COVID-19 wards (Fig 3). The posters, which are A2 size with an easy-to-read font size, have been placed in visible locations on COVID-19 wards during the second wave of COVID-19 in Liverpool. The poster can also be used as a hospital-wide screen saver to increase staff awareness.

Pilot version of poster detailing holistic COVID-19 practice pointers.
The posters are part of an integrated bundle and complementary QIP for multidisciplinary teams caring for people with COVID-19. The complementary QIP has been to implement and assess feedback from the multidisciplinary team on use of a checklist based on the mnemonic ‘OSCAR’. This includes key elements of COVID care: Oxygen, Steroids, Coagulation, Antibiotics/antivirals, and Research treatments. It is designed to improve documentation and prescribing, and prompts explanation of components of COVID-19 care to the patient. Overall, the bundle consists of COVID ward induction sessions including introduction of the OSCAR checklist, lanyards and posters with the checklist, the COVID-19 practice pointer poster and a patient information leaflet.
This QIP has several limitations. It was pragmatic, non-randomised and had multiple potential sources of bias. These included lack of sequential participant recruitment, ad hoc survey implementation, variable times of survey completion (eg pre- and post-discharge) and exclusion criteria that may have led to under-representation of underserved groups or those most severely affected by COVID-19. We overcame some of these issues by supporting participants to complete the survey and involving carers and/or family where possible. However, this may have led to further bias. Moreover, survey respondents’ ability to recall their experiences when severely ill may have been impaired (even if they made a good recovery) and gratitude towards staff for care received may have influenced their response. We partially addressed these limitations by allowing sufficient time to complete the survey with appropriate support and clearly explaining that the aim of the survey was to elucidate both the successes and shortcomings of patient care in order to improve our service in the future. Our participants’ social and clinical demographics appear similar to other published cohorts from the UK,12 but it should be noted that, likely due to Liverpool’s background ethnodemography, only 11% of participants were BAME in our cohort. Future analysis of COVID-19 feedback survey data will aim to evaluate equity of healthcare provision by comparing responses of BAME patients with other patient groups.
Conclusion
Our survey of people hospitalised with COVID-19 showed that care quality during admission was rated and recommended highly. However, the survey also revealed areas for improvement in holistic healthcare provision including communication, especially with relation to medications and discharge planning, and sleep and food quality. To improve care in 2021, we are implementing the ‘COVID-19 practice pointers’ poster within an integrated educational bundle on COVID-19 wards within LUHFT. We hope to be able to scale up this bundle for future evaluation of its impact on the care of people hospitalised with COVID-19 at LUHFT and, potentially, beyond.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/FHJ:
S1 – COVID-19 inpatient satisfaction survey SOP.
S2 – Full sociodemographic and clinical details of people hospitalised with COVID-19 (n=94).
Acknowledgements
We thank all the respondents who kindly gave their consent and participated in this study and the multidisciplinary teams on wards 3X, 3Y, 9X and 9Y for supporting this project. We are grateful to Kathryn Barnes and the reprographics team at LUHFT. We also thank Claire Duffy and Andrea Kearley for support with data collection and the departments of respiratory medicine (especially Dr Ayesha Kumar and Dr Fred Frost), clinical effectiveness (especially Helen Vormawah), patient and family experience, and communications of LUHFT for their invaluable support and collaboration.
Funding
TW is supported by grants from the Wellcome Trust, UK (209075/Z/17/Z); the Medical Research Council, Department for International Development, and Wellcome Trust (Joint Global Health Trials, MR/V004832/1), the Academy of Medical Sciences, UK; and the Swedish Health Research Council, Sweden.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.