
ABSTRACT
Introduction The rising prevalence of multi-resistant organisms threatens the efficacy of current antimicrobial treatments. Antibiotic stewardship is a key factor in slowing the development of resistance and must become part of a clinician’s regular practice. National guidance unanimously emphasises the importance of a 48-hour review of antimicrobial prescriptions. We assessed the compliance of antibiotic reviews across two sites in Wales.
Method Two cycles of data were retrospectively collected across two teaching hospitals in Wales prior and following introduction of an antimicrobial alert sticker. A univariate odds ratio for 48-hour referral stratified by C-reactive protein (CRP) was calculated in a logistic regression model for the cycle one data.
Results One-hundred and thirty-nine patients were included in the cycle 1 data across both sites. We identified that patients with a CRP ≤100 mg/L (a marker of less severe infection) were less likely to have their antibiotic prescription reviewed by 48 hours.
Discussion Patients with CRP ≤100 mg/L were less likely to receive a 48-hour review of their antimicrobial prescription. Compliance with review improved following introduction of a simple alert measure.
Introduction
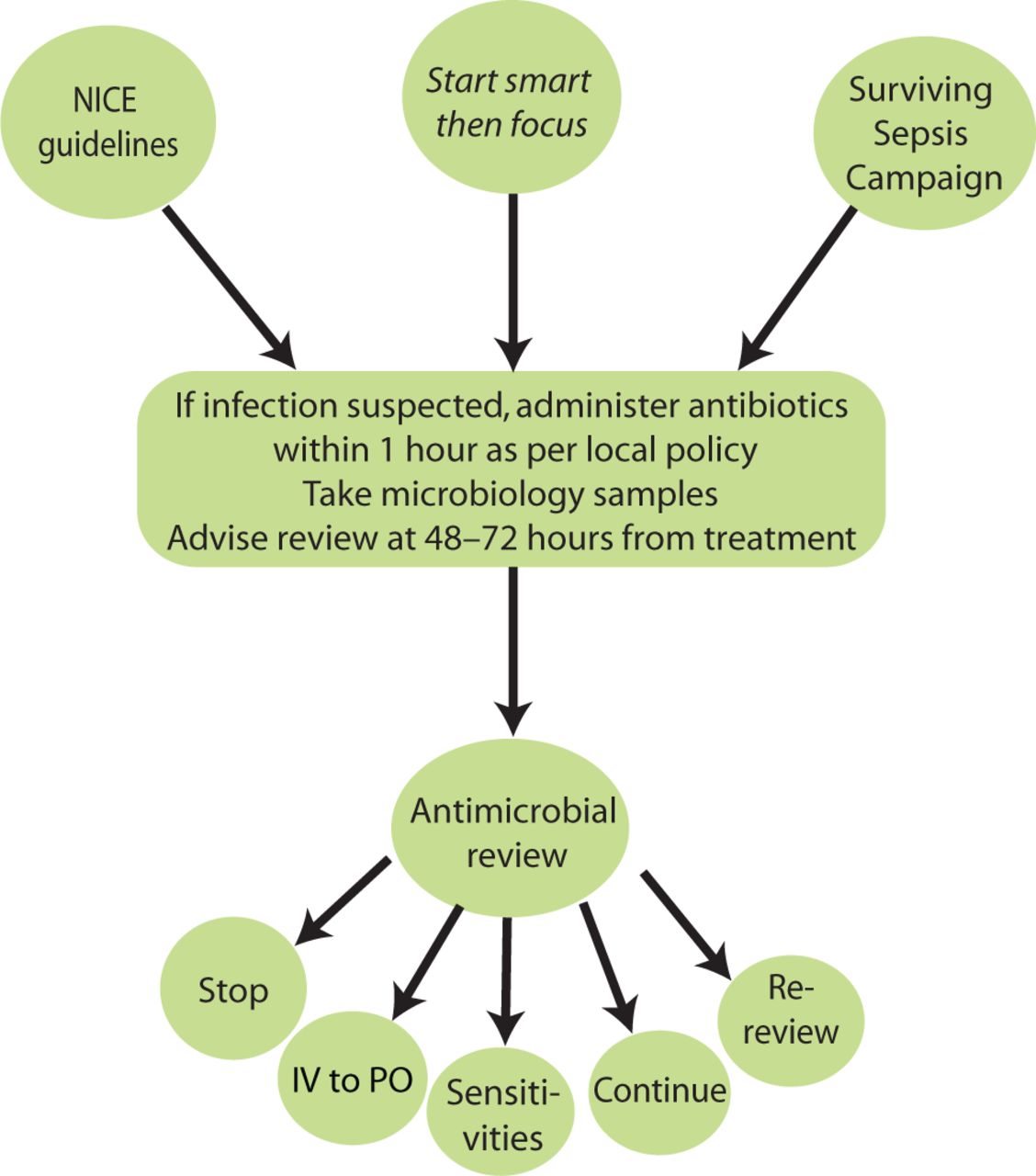
Antimicrobial resistance is ‘one of the biggest threats to global health, and is recognised as a ‘worldwide crisis’.1,2 National Institute for Health and Care Excellence (NICE) guidance, Start smart then focus and UK Surviving Sepsis Campaign all recommend re-assessment of antimicrobial prescriptions at 48 hours to support their rationale for use (Fig 1).3–5

Guidance on antimicrobial use as recommended by NICE,3 Start smart then focus4 and Surviving Sepsis UK.5 IV - = intravenous; NICE = National Institute for Health and Care Excellence; PO = per oral.
The UK Surviving Sepsis Campaign recommends administration of broad-spectrum empiric IV antimicrobials within an hour following the recognition of sepsis and septic shock.5 Importantly, they also recommend daily assessment for de-escalation of antimicrobial therapy.5
Unfortunately, there is some suggestion that the international sepsis campaign has increased inappropriate antimicrobial use in the emergency department setting.6 Bacterial disease was suspected or confirmed in only 71% of patients treated for suspected sepsis (2008 definition) in one emergency department in the Netherlands.6 Despite absence of bacterial disease in 29% of the patients after rigorous diagnostics, median duration of antibiotic treatment in this group was still 7 days (interquartile range 4–10).6 The reasons for this are complicated and multi-factorial but likely to include lack of senior decision makers, time pressures and uncertainty surrounding the diagnosis during the acute phase.
It is unlikely that bacterial infection will ever be perfectly diagnosed at the point of admission, and so regular review of antibiotic prescriptions with the view to de-escalating or switching to oral agents (if appropriate) or stopping (if not indicated) is crucial. The 48–72-hour antibiotic review is frequently used as a prompt, a ‘soft stop’ (supplementary material S1) and surrogate marker for this practice.7
We report findings from the antibiotic prescription audit that may help teams to develop targeted interventions to improve compliance with antimicrobial review. We followed this up with a non-randomised quality improvement project independently at site 1 and in collaboration with the pharmacy department at site 2 with the aim of improving compliance with 48-hour review using a sticker prompt.
Objective
We sought to measure clinical review post-antimicrobial prescription within unscheduled care settings in two acute hospitals in Wales. We carried out an antibiotic prescription audit that addressed two questions.
Is a 48-hour review readily undertaken following the initiation of antibiotics?
Does the likelihood of clinical review vary depending on the C-reactive protein (CRP) level on admission?
Rationale for use of CRP as a surrogate marker of severity of infection
An observational study in 2005 identified that CRP was superior as a marker of infection when compared with white cell count and temperature alone.8 The combination of CRP and a temperature (>38.2°C) produced 100% specificity for infection. There is no absolute cut off for CRP and the trend of a CRP is often more useful than a single result. However, in general, the higher the CRP, the more significant the inflammation and, correspondingly, the more significant the infection. In this study, CRP was used as a surrogate marker for severity of infection and patients were categorised according to CRP levels using arbitrary cut offs. Although these cut off points are not recognised or defined nationally, they are frequently used in clinical practice.
Methods
Initial audit
An audit across two hospital sites in South Wales assessing compliance of antimicrobial review as recommended by NICE guidelines and Start smart then focus.3,4
Site 1: This is a tertiary teaching hospital. Patients on the medical admissions unit who had been prescribed antibiotics between Monday and Friday over a 3-week period were included. Data were collected on the presence of an antibiotic review at 48 hours, either from the plan in the medical case notes or from a change on the medication chart. Patients’ CRP results from the first 48 hours of admission were also recorded.
Site 2: This is a district general hospital. Data were collected across 10 medical and surgical wards within the hospital on a single day. All patients who had received antibiotics during their current admission were included. Data were collected from medical case notes and electronic records and included the presence or absence of the 48-hour review and CRP results during this time.
To test the association between the CRP result when antibiotics were started with the occurrence of a documented 48-hour review, we pooled pre-intervention data from both hospitals. For analysis, CRP levels were categorised into no CRP measure taken; low CRP (≤20 mg/L); CRP 21–100 mg/L; and CRP >100 mg/L. These categories were chosen as a surrogate marker for severity of infection at the point of prescribing. Univariate odds ratios for 48-hour referral stratified by CRP test results (excluding patients with no CRP test) were calculated in a logistic regression model using the high CRP group as the referent. Analysis was carried out in STATA v14.
Interventions
Two key interventions were introduced at each site and the audit repeated. Education on the current best practice was circulated to prescribers and the introduction of an antibiotic alert measure (a sticker to be placed with the patient’s medical notes) to assist and prompt a 48-hour antibiotic review.
Site 1: Data from the medical assessment unit were collected over a 2-week period using the same criteria for inclusion. Patients who had received antibiotics for longer than 48 hours at the time of review were excluded as they had passed the intervention measure point. An antimicrobial alert in the form of a sticker was placed in the notes to prompt a review (Fig 2a).

48-hour review antibiotic stickers. a) Site 1. b) Site 2.
Site 2: In collaboration with the pharmacy department a 48-hour antibiotic review sticker (Fig 2b) was designed and piloted on one medical ward. Data were collected on patients prescribed antibiotics during their admission over a 3-week period. One patient was excluded as the antibiotics were started pre-admission.
Results
One-hundred and thirty-nine patients were included in the pre-intervention audit from both sites. Twenty-eight patients were excluded due to either a lack of data, being lost to follow up or where patient notes were unavailable. Antibiotic review occurred in 53% (74/139) of patients at 48 hours. Among 131 patients for whom a CRP test was recorded, the mean CRP was 76 in patients whose antibiotics were not reviewed and 121 in those who were.
Antibiotics were reviewed at 48 hours in 12.5% of patients with no CRP result (8 patients), 50% with ‘low’ CRP (≤20 mg/L; 26 patients), 44% with CRP 21–100 mg/L (52 patients) and 70% of patients with CRP >100 mg/L (53 patients). Logistic regression analysis using the highest CRP group (CRP >100 mg/L) as referent showed that the likelihood of a 48 hour review was lower in patients with lower CRP test results, or no CRP test, than those with a CRP >100 mg/L (Table 1).
Logistic regression univariate analysis of the likelihood of 48-hour review depending on category of C-reactive protein test result
Site 1: There was a 30% increase in the number of antimicrobial reviews performed during the post-intervention period. Of the 26 patients audited post-intervention, 21 (81%) had clear, documented antimicrobial reviews carried out during the first 48–72 hours. Ten reviews occurred prior to receipt of the sticker intervention and 11 following the sticker prompt. Four patients (15%) had no signs suggestive of sepsis on admission or during the first 48 hours. Of the patients with no signs of sepsis, 75% had clear, documented antimicrobial reviews, following which, the antibiotics were stopped at 48 hours.
Site 2: There was a 20% increase in the number of antimicrobial reviews performed during the post-intervention period. Of the 20 patients audited post-intervention, 15 (75%) had clear, documented antimicrobial reviews carried out during the first 48–72 hours. Ten reviews occurred prior to receipt of the sticker intervention and five following the sticker prompt. Four patients continued broad-spectrum antibiotic treatment with no clear justification.
Discussion
Antimicrobial prescribing audits from two hospitals have shown that patients with no CRP result or a low CRP are less likely to have their antimicrobial treatment reviewed in the first 48 hours of admission in comparison to those with a high CRP (Table 2). In the context of antimicrobial stewardship, this is a great concern as the de-escalation or cessation of antibiotics is most likely to be appropriate in this cohort of patients. Many health boards have already recognised the need to encourage prescribers to review antibiotics at 48 hours by including a prescriber ‘review section’ on medication charts (supplementary material S1).7 Our baseline data suggest that this measure isn’t sufficient to generate the significant culture change required.
Comparison of C-reactive protein value against a 48 hour antibiotic review at sites 1 and 2 pre- and post-intervention
The results of two pilot quality improvement projects (uncontrolled and non-randomised interventions) suggest that simple interventions designed to prompt antibiotic review have the potential to improve review compliance particularly among patients with less severe infection (as measured by CRP response). Reviews were increased by 20–30% and use of broad-spectrum antibiotics reduced in patients with low CRP (≤20 mg/L) at both sites. Four patients with a CRP ≤100 mg/L at site 2 remained on broad-spectrum antibiotics over a weekend, when the sticker prompt was not in operation, further demonstrating the effectiveness of this strategy.
There are a number of limitations with this cross-site study. Site 1 only collected data between Monday and Friday. The out-of-hours antibiotic review data are therefore not captured and may give a positive skew of results in light of the limited workforce on weekends. At site 2, the second cycle of data was collected on a medical ward where the project lead was based, introducing a level of bias.
While the likelihood of performance bias by the care provider is recognised in the post-intervention groups, the pre-intervention baseline data across both sites demonstrate clear shortcomings in the standards of antibiotic stewardship across different specialties and multiple sites. Despite slight variations in the methodology pre- and post-intervention at sites 1 and 2, one of the strengths of the study is that similar results were produced by both site teams demonstrating that the findings are generalisable. Additionally, it is indicative of a more systemic issue, suggesting our notion of ‘A lower CRP in the context of infection, is less likely to lead to antimicrobial review,’ is a wide-spread problem requiring improved antibiotic stewardship compliance.
Because of the limitations of the study, the following conclusions can only be considered exploratory and need to be investigated further. They have been shared so that they can be considered in future studies and when individuals are designing interventions to improve antimicrobial prescribing.
We believe that clinical teams working in an acute setting are generally performing under pressure and so principally focus their attention on patients who are more unwell. As a result, we suggest that ‘sicker’ patients tend to have their antimicrobial treatments reviewed and amended. We believe that patients that have less severe infection or limited/no evidence of infection at the time of admission (ie a CRP ≤100 mg/L) will be stable at the point of review and, as such, are less likely to have their antibiotics reviewed and de-escalated. Unfortunately, we did not collect information on National Early Warning Score (NEWS) at site 1 to allow for further comparison and analysis. This may have provided further evidence to support this assumption. We plan to repeat the audit, collecting information on patients’ temperature and NEWS to see if the findings are reproducible and if these findings support our initial assumption.
We also believe that a positive effect of antibiotic therapy can be falsely attributed to patients who are stable at the time of review, creating a reluctance to change therapy (an ‘if it’s not broken, don’t fix it’ mentality). Clinical teams, therefore, need to be educated and encouraged to critically review previous decisions in light of new information. In a previous audit in 2007 (personal communication) we identified five patients with a documented diagnosis of respiratory tract infection who were prescribed antibiotics. All patients had no objective evidence of bacterial infection (CRP <5 mg/L; apyrexial; normal white cell counts; normal chest X-rays). Three of these patients received extended courses of antibiotics (8, 10 and 12 days). We believe that these extended courses of antibiotics could be related to similar issues as identified earlier (ie lack of review in stable patients).
We propose that a change in culture is required in order to ensure appropriate antimicrobial review for patients who are started on antibiotics at the point of admission when subsequent data suggest that either infection is not present or is mild. We suggest that medical teams need to be educated to specifically look out for patients who are stable or who have limited evidence of infection, so that those patients can be reviewed more carefully and antibiotics de-escalated or stopped as appropriate. Using ‘low’ CRP results as a prompt is one way to achieve this.
We believe a culture change to promote antibiotic review and instil confidence in a clinician’s ability to stop antibiotics when not indicated is of particular importance. There should be an additional focus on clear documentation from prescribers and clinical teams, highlighting the reasons behind the decision for initiating antibiotics and additionally identifying parameters for de-escalation. Clear documentation and handover are essential to ensure antimicrobial stewardship success.
In summary we have identified that patients with low CRP, CRP 21–100 mg/L or no CRP on admission are less likely to have their antimicrobial prescriptions reviewed when compared with patients with high CRP (>100 mg/L). We believe that antimicrobial stewardship teams should target this group of individuals and that a change in culture among clinical teams is required to achieve this.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj:
S1 – Medication chart used across Wales with ‘soft stop’ antibiotic review.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.