
ABSTRACT
Within the last decade, clustering of comorbidities has become an increasing health problem on a global scale and will continue to challenge healthcare professionals in the coming years. People with multiple diseases find difficulties in managing their daily lives due to the implications each disease brings; attending and keeping up to date with hospital appointments, being prescribed and taking various medications, the effects of mental health and quality of life, and the impact it has on their families. Most research in clinical trials often exclude individuals with multimorbidity and observational studies mainly focus on single disease outcomes, therefore there is an opportunity to encourage future research in an area which could help prevent further cases and improve the lives of those already living with multimorbidity. This review aims to summarise the rising prevalence and most common clusters, highlight the challenges faced in healthcare, and explore ways to improve future research.
Introduction
Chronic conditions are the leading causes of death globally.1 The World Health Organization (WHO) predicted that 87% of deaths in high-income countries were attributable to chronic conditions, and the proportion of worldwide deaths caused by chronic conditions is expected to rise from 59% in 2002 to 69% in 2030.2 While many people are known to have at least one type of chronic condition (such as diabetes, heart failure, asthma, chronic kidney disease or depression), in more recent cases people are now living with multiple chronic conditions, known as comorbidities or multimorbidity. The terms comorbidity and multimorbidity are often used interchangeably to refer to co-occurring conditions, however they have an important distinction.3 Comorbidity refers to one or more additional conditions in reference to an index condition, in comparison, multimorbidity is clarified as no one condition being considered as the index.4–6 Multimorbidity is thus highly heterogeneous, and can be used to describe a wide array of chronic conditions. Furthermore, the concept of concordant and discordant clusters play an important role in healthcare, as some conditions may share similar pathophysiology and treatment known as concordant, while other conditions may have unrelated pathophysiology and have different or even contradictory treatment.7 Therefore, the complexities of multimorbidity has brought major challenges for the healthcare system, healthcare professionals and the person living with them.8
Here, we aim to summarise the rising prevalence of multimorbidity and the most common clusters, highlight the current challenges faced in healthcare and areas of future healthcare research.
Rising prevalence
The literature presents differing estimates of prevalence due to the various methodologies used to define multimorbidity including the number and type of conditions being studied.9,10 A systematic review found 132 definitions involving 1,631 different criteria.11 Previous systematic reviews also emphasised the heterogeneity of existing multimorbidity definitions.9,10 Some measures of multimorbidity are based on simple counts of chronic conditions from self-report or clinician assessment, while other measures were based on indices to assess the burden of mortality by using weights on the range of conditions, duration, severity and resource utilisation such as the Charlson Comorbidity Index or the Elixhauser Comorbidity Index, however, data on such indices are often limited.10–12 Furthermore, these measures were originally developed and validated among selected populations such as elderly patients or in-hospital settings.13 For this reason, in most studies multimorbidity is most commonly defined using a pragmatic approach of simply summing the number of coexisting chronic conditions, with the most common definition of two or more chronic conditions clustered together.8,12,14
The estimated prevalence of multimorbidity across existing studies range from 7% to 99%.4,12,15–34 Alongside the definition of multimorbidity, the setting and population of the study largely influence the estimates; for example, when considering the whole population a cross-sectional study in Scotland using primary care data found 23.2% of participants had multimorbidity, while in a study from the USA estimated the prevalence to be 22.6% and an Australian study based on national survey data showed 32.6%.16,35,36 The prevalence increases with age.4 When considering the older population from the study in Scotland, around 65% of those aged more than 65 years and almost 82% of those aged 85 years or more had multimorbidity, whereas a study from Spain found that for those over the age of 85 years the prevalence was as high as 95.1%.16 In non-western countries such as Iran, when considering adults aged 40 to 75 years, the prevalence of multimorbidity reached 19.4%, while in southern Brazil, a study in adults over the age of 20 years found 29.1%.37,38 Similarly, a cross sectional study in Bangladesh reported a prevalence of 54% in those over 60 years, and in Nigeria, 49% of elderly patients admitted in hospitals had multimorbidity.28,39
Despite the variability in definition and population, all studies have highlighted a high prevalence of multimorbidity. A recent longitudinal study using the English Longitudinal Study of Ageing (ELSA) data demonstrated that the prevalence of multimorbidity steadily increased over time, with prevalence increasing from 31.7% to 43.1% in 10 years, signifying an expected rise of multimorbidity in the coming years.40
Most common cluster
Understanding why certain diseases cluster together, the pathways through which they interact biologically and how social environment, economic or political factors contribute to disease clustering, has been recognised as the syndemic approach.41 Disease clusters have different levels of impact on the patient and the healthcare they receive, based on concordant and discordant clusters; for example, the Piette and Kerr's conceptual framework of concordance and discordance suggests that the comorbidities for diabetes can be either concordant (meaning the comorbidity will support diabetes management) or discordant (meaning the comorbidity would compete with the diabetes care).42 So, patients with a higher number of concordant comorbidity conditions will receive better diabetes care due to provider cueing and synergistic care, while patients with more discordant conditions will receive the worse diabetes care due to distraction and competition for limited resources.42 However, the research in this is still very limited.
Patterns of multimorbidity have mainly shown an increasing prevalence specifically in cardiometabolic conditions.43–47 A most recent cluster analysis based on data from the UK, showed that diabetes and cardiovascular diseases were the largest group of multimorbidity conditions.46 Similarly, a study investigating multimorbidity patterns in the elderly, ranked cardiovascular and metabolic disorders to be the first pattern among other disease patterns.43 In addition, the Emerging Risk Factor Collaboration estimated at the age of 60 years, people with cardiometabolic multimorbidity was associated with 12 years reduced life expectancy compared with those without cardiometabolic multimorbidity.44 The leading top 10 causes of mortality are cardiometabolic conditions, therefore cardiometabolic multimorbidity has been identified as one of the greatest clusters impacting patients.
Likewise, greater multimorbidity of physical conditions is linked to mental health conditions, such as depression.6 More than 300 million people worldwide are affected by depression, whose symptoms are continuous low mood, poor concentration, loss of interest, low self-esteem, feeling anxious or worried and, in the severe forms, self-harm or suicidal thoughts.48 People with multimorbidity have the highest prevalence of depression, but it is often overlooked, since single diseases are given more priority.16,49
Key healthcare challenges
One of the key challenges faced by individuals with multimorbidity and healthcare professionals is the fragmented clinical care since it creates miscommunication and may confer inconsistent healthcare messages. A qualitative review found that people with multimorbidity received services from multiple healthcare specialists who only focus on single conditions of their health, and do not see them as a whole person.50 In addition, it becomes burdensome and unsafe for the individual as it can become duplicative with differing messages, time-consuming and can lead to an increase in the prescription of multiple medications.16,35 Polypharmacy, defined as the simultaneous use of five or more chronic medications, is highly prevalent in older adults, especially for people with multimorbidity.51 Polypharmacy increases the potential risk of adverse drug reactions and side effects. A study reporting expert opinions expressed that nearly 50% of older adults take one or more medications that are not medically necessary, as a result of difficulties in assessing whether new symptoms are part of previously known conditions or the medication for it or if it's a new clinical condition.52,53 Furthermore, a recent study in older adults from England found almost one-third of the total population using five or more drugs was significantly associated with a 21% increased rate of falls over a 2-year period, which potentially increases the risk of injury-related hospital admissions.54
People with multimorbidity are frequent users of hospital services, including regular hospital appointments, readmission, emergency admissions and the use of outpatient services.55,56 A large study of patients registered in general practices in Scotland showed that participants with multimorbidity (≥4 vs 0 conditions) were six times more likely to experience unplanned hospital admissions and 14 times more likely to have potentially preventable unplanned hospitalisations.57 The English Hospital Episode Statistics (HES) demonstrated that people older than 65 years comprise 60% of admissions to hospitals, 65% of occupied-bed days, 90% of delayed transfers and 65% of emergency readmissions.58 Previous studies report substantial increases in healthcare costs and resource utilisation when additional chronic comorbidities are present.59 A recent primary care study demonstrated the mean annual cost for face-to-face consultations was £412.70 per patient without comorbidities, £516.80 for one comorbidity, £620.75 for two comorbidities and £778.83 for three or more comorbidities.3 Moreover, a systematic review identified 35 studies, of which, almost all demonstrated a positive relationship between multimorbidity and healthcare utilisations outcomes (physician visits, hospital use and medication use) and healthcare costs outcomes (medication costs, out-of-pocket costs and total healthcare costs).60 Although people with multimorbidity consume a greater proportion of healthcare resources and might benefit from disease-specific programmes, for most people with multimorbidity, there is a need to maximise efficiency of outpatient services across multiple chronic conditions.61
Another key healthcare challenge is that people with multimorbidity are more likely to have a lower quality of life, as the number and severity of chronic conditions increases, this impacts peoples physical functioning, emotional well-being and social interactions.48,62 Also, those with multimorbidity have a much lower life expectancy compared with those without multimorbidity. A study in the UK using 36 chronic conditions found that at the age of 45 years, participants with multimorbidity lost 5.15 more years of life (95% confidence interval (CI) 4.78–5.14) than participants without multimorbidity; the corresponding figure at the age of 65 years was 4.54 years (95% CI 4.21–4.87).63 When accounting for the severity of the conditions, at 45 years, participants with poor health and multimorbidity had 9.00 years of life lost (95% CI 8.47–9.53) compared with those with good health without multimorbidity, while participants with top 10 comorbidities had 6.53 years (95% CI 6.01–7.05) lower life expectancy compared with those without the top 10 comorbidities.63,64 Lastly, although the prevalence of multimorbidity has shown to be high in older adults, multimorbidity is becoming more prevalent in younger age groups. A study from Scotland found that the onset of multimorbidity occurred 10–15 years earlier in people living in the most deprived areas compared with the most affluent.16
Multimorbidity is already burdensome and has many healthcare challenges as described, yet the SARS-CoV-2 (COVID-19) pandemic has placed greater risks on people with multimorbidity. A recent international survey evaluated the impact of COVID-19 on routine care for chronic diseases during 31 March 2020 to 23 April 2020 and found that most healthcare professionals (67%) identified moderate or severe effects on their patients due to changes in healthcare services since the outbreak; and 80% reported the mental health of their patients worsened during COVID-19.65 Furthermore, many low- and middle-income countries have overstretched healthcare systems and the pandemic has further overwhelmed them. Current research has demonstrated that people with pre-existing comorbidities and multimorbidity are strongly associated with the risk of severe COVID-19 infection resulting in hospitalisation which leads to a cascade of further complications due to multi-organ failure or result in mortality.66–68
Encouraging future research
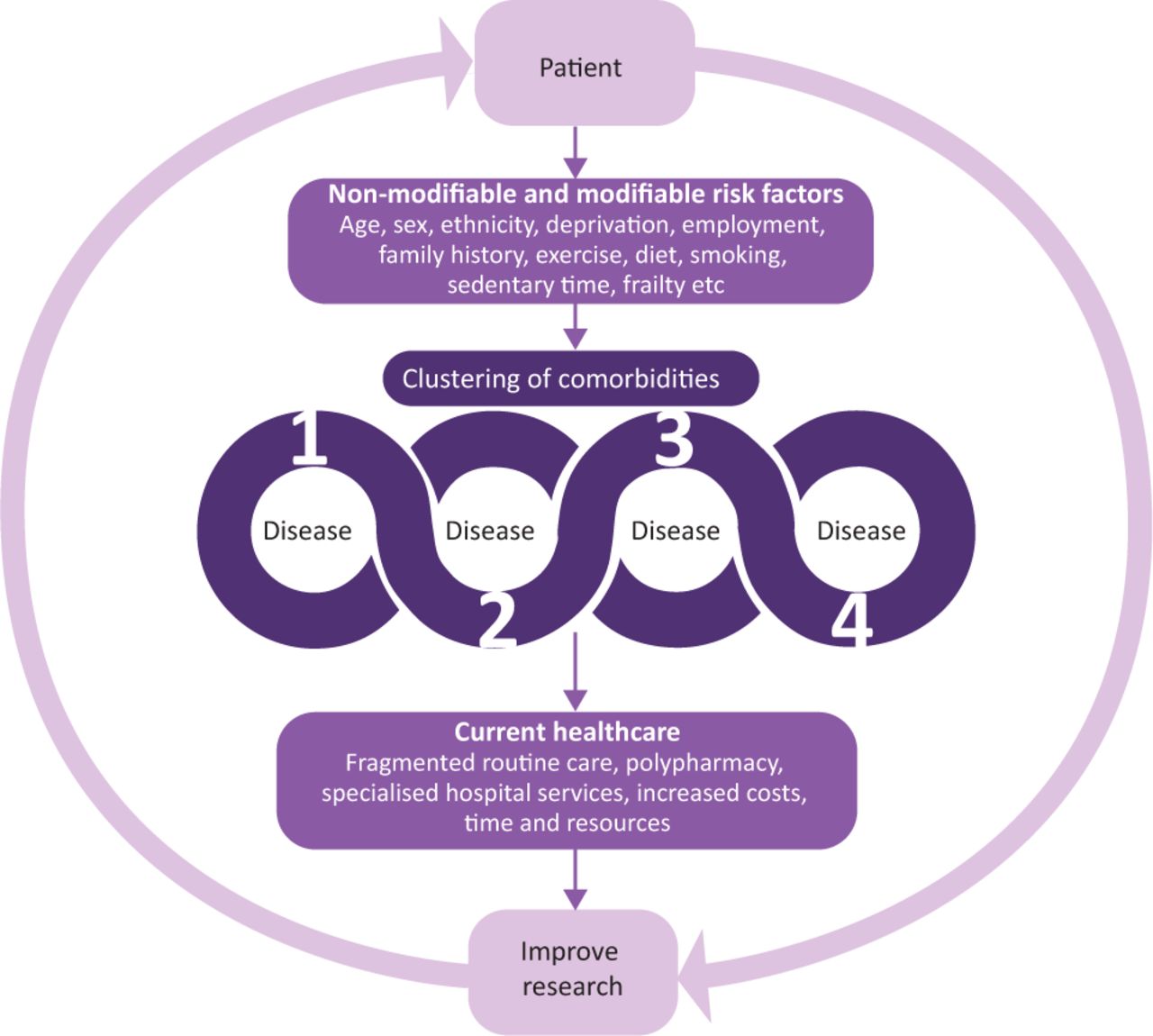
The healthcare challenges reflect the fact multimorbidity is a complex process (Fig 1) and has become an emerging priority worldwide.8 Understanding why certain diseases cluster together and the pathways of developing multiple diseases is key to preventing further cases. The evidence highlights the need for updated standard guidelines for research purposes and for potential health benefits in people with multimorbidity.9,10,17 Healthcare models are currently disease-orientated, meaning that the management of chronic conditions apply to the single condition and may not be relevant to those with multimorbidity.69 This is partly due to the fact these models were based on evidence which often excluded individuals with other morbidities, or have been disease specific.69 Healthcare systems across the globe use different approaches to tackle the problems caused by multimorbidity.70 In the UK, the National Institute for Health and Care Excellence (NICE) has published guidelines for the assessment and management of people with multimorbidity.14 The key message from this guideline was that care should be individualised for each person.14 Therefore, healthcare professionals are recommended to use a tailored approach of care involving personalised assessment and developing individualised management plans.14 However, the evidence on the update of these guidelines is still limited. Furthermore, while a tailored approach in clinics mainly focus on medication management and pharmacological interventions, there is an increasing recognition for effective interventions to counterbalance the effects of lifestyle behaviours and self-management.71

Clustering of comorbidities and future research. Adapted with permission from the authors.
The most recently published report Multimorbidity: a priority for global health research by The Academy of Medical Sciences (2018) highlights the fact that the increased prevalence of chronic conditions are not only due to an ageing population but also due to a shift to unhealthy lifestyle behaviours in recent decades.8 The main modifiable healthy lifestyle behaviours (including physical activity, healthy diet or smoking cessation) have been shown to be effective in the management of several chronic conditions as well as some comorbid conditions. A recent study in the UK found that, regardless of the presence of multimorbidity, engaging in a healthier lifestyle was associated with up to 6.3 years longer life for men and 7.6 years for women.72 The study also highlighted that not all lifestyle risk factors equally correlated with life expectancy, with smoking being significantly worse than others.72 When it is proven difficult to reduce all risk factors, healthcare professionals may focus on stronger determinants of life expectancy, thus individualising the care of patients with multimorbidity in line with NICE guidance.72
Lifestyle behaviours are based on individual choices, therefore self-management interventions were introduced with the aim to improve the way individuals self-manage chronic conditions and to optimise their health. Self-management interventions have been widely implemented within primary care following NICE guidance for many disease management pathways; for example, the Diabetes Education and Self-Management for Ongoing and Newly Diagnosed (DESMOND) structured education self-management programme in those with type 2 diabetes has shown to reduce cardiovascular disease risk, reduce depression and promote healthy behaviour change, such as increased physical activity and weight loss, while being a cost-effective intervention.73,74 However, there is limited evidence of interventional research conducted for the effective management of people with multimorbidity.75 A Cochrane review of interventions found only three studies which involved health-related behaviours where the results were mixed.75 Currently, the ongoing Movement through Active Personalised engagement (MAP) study aims to assess the effectiveness of a structured self-management education programme with the primary goal of increasing daily physical activity in patients with multimorbidity.76 Although, the follow-up for the study is short (12 months), which will not allow the evaluation of long-term mortality benefits. Therefore, further interventional research in this area is also required.
In view of the rapidly increasing prevalence of COVID-19 infection across the globe, further research is needed to understand the biological mechanisms involved between multimorbidity and the increased risk of severe COVID-19 infection. A study from Charité University Hospital in Berlin reported the findings on causes of death and comorbidities from 26 decedents with severe COVID-19, indicating that immediate causes of death were due to septic shock and multi-organ failure which was directly linked to lung damage initiated by COVID-19 and not related to pre-existing health conditions in most cases.77 Future research on a larger scale is much needed as most studies have focused on small sample sizes, in order to understand why those with multimorbidity suffer with the worse outcomes. Finally, consider the longer-term effects such as changes in lifestyle behaviours due to the lockdown, development of further physical and mental health conditions, uptake of vaccines and the outcomes of those patients with previous multimorbidity who have survived COVID-19.
Conclusion
In summary, the literature presents considerable evidence on the increased prevalence and the negative impact that multimorbidity has on patients, healthcare professionals and the healthcare system. Yet, there is still limited research on understanding the reality of the uptake of national guidelines for the management of multimorbidity, approaches to managing multimorbidity, identifying clusters of multimorbidity and, lastly, the initial and longer-term effects of COVID-19. Now, more than ever, we need to prioritise multimorbidity research using high-quality real-world primary care data and future interventional studies to gain a better insight into the complexities of multimorbidity.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.