
ABSTRACT
Patient safety events are common in healthcare. We can learn from other safety-critical industries that further incidents are most likely to be prevented where lessons are learned at the system level rather than looking to attribute blame for errors to individuals. Progress has been made over the last 20 years and relies on a positive safety culture (or just culture) where staff trust organisations to investigate safety events for learning rather than blame. Systems-based investigation models, such as the Systems Engineering Initiative for Patient Safety (SEIPS), help investigators to consider the full range of contributory factors across a system and to identify important findings. Considering the hierarchy of controls, recommendations should be targeted at system changes which are more likely to produce sustained safety improvements, rather than at individual behaviours or training, which are less likely to influence future safety. Systems-based safety investigations can positively influence safety culture in organisations.
Key points
Systems-based investigations examine the system as a whole and look for flaws in the system supporting delivery of healthcare rather than in the individuals involved.
Systems-based patient safety investigation has been slow to become usual practice in healthcare, despite being acknowledged and recommended for the past 20 years.
The establishment of the Healthcare Safety Investigation Branch (HSIB) in the English National Health Service in 2017 was intended to promote systems-based patient safety investigations.
The Systems Engineering Initiative for Patient Safety (SEIPS) is an example of a systems-based model for incident investigation and is specifically designed for use in healthcare.
Recommendations to mitigate identified safety hazards should consider the hierarchy of controls to ensure recommendations are made at the most effective level.
Introduction
Safety incidents occur in all industries and are common in healthcare. According to the Health and Safety Executive, ‘an investigation can help you identify why the existing risk control measures failed and what improvements or additional measures are needed.’1
Most safety-critical industries, like aviation or the nuclear industry, take a systems-based approach to the investigation of safety incidents, rather than focusing on the actions of individuals. They recognise that few incidents can be attributed to individual actions; the vast majority relate to failures in the systems in which people work. Poor design and usability of equipment, inadequate testing of software programmes or confusing labelling of components all increase the risk of errors. Likewise, human performance is impaired by factors such as fatigue, inadequate nutrition and hydration, badly designed environments, external distractions and complex tasks. Investigations in other industries recognise that addressing such factors more effectively reduces long term risk than focusing on individuals’ actions.
In healthcare a systems-based approach to the investigation of patient safety incidents has been recommended for at least 20 years but has been slow to establish. In 2017 the Healthcare Safety Investigation Branch (HSIB) was founded to develop systems-based approaches to safety investigation in healthcare.2 The purpose of HSIB's investigations is prevention of future similar incidents rather than attribution of blame and liability to individuals.
A very brief recent history of incidents and investigation in healthcare
Recent interest in patient safety dates from 1999, when the United States Institute of Medicine published the report To err is human.3 This used retrospective case note review and concluded that between 44,000 and 98,000 people died in the US healthcare system each year because of medical errors. The report recognised that most cases of medical error were due to ‘faulty systems, processes and conditions that lead people to make mistakes or fail to prevent them’.3
These findings were echoed the following year by a UK report An organisation with a memory4 which estimated that about 10% of people admitted to hospital sustained harm because of medical care. This report acknowledged that, although human error may be a precipitant, ‘there are usually deeper, systemic factors at work which if addressed would have prevented the error or acted as a safety-net to mitigate its consequences’.4 It concluded that the NHS needed improvements in four areas:
Unified mechanisms for reporting incidents.
An open culture, in which incidents can be reported and discussed without fear of unjustified blame.
Mechanisms for ensuring that, where lessons are identified, changes are made.
Wider appreciation of the value of systems approaches in preventing, analysing, and learning from incidents.
Twenty years later there is still evidence that the English NHS is struggling to achieve these goals.
Incident reporting mechanisms are in place across the NHS. The National Reporting and Learning System (NRLS) was established in 2003 and the Serious Incident Framework in 2013. Further review as part of the NHS patient safety strategy5 has resulted in the ‘learn from patient safety events’ (LFPSE) system - previously called the ‘patient safety incident management system’ (PSIMS) while in development - which commenced in summer 2021. Incident reporting rates vary between organisations and are positively correlated with independently defined measures of safety culture.6
A just culture is a culture of trust, learning and accountability7 and is a prerequisite for confident reporting of errors and near misses. The autumn 2020 NHS Staff Survey had 600,000 respondents. 60.9% of staff involved in an incident felt they were treated fairly and 72.5% would feel secure about raising concerns.8 This suggests disappointing progress since the Francis Inquiry in 20139 and the Morecambe Bay Investigation in 2015.10
A safety culture concentrating on individuals can result in limited learning from incidents and in blame. Most recent healthcare safety investigations have used root cause analysis. Recommendations have often been person-centred, advocating improved adherence to rules and policies, further education and training and reminders to check more at the point of care.11,12 This tendency to concentrate on individual, linear contributory factors rather than the whole system limits the benefit of an investigation and can lead staff to feel that things never change. Patient safety incidents that have been managed in this way, including ‘never events’, have not been shown to decrease as a result of such interventions.13
In response, there have been significant developments in the English NHS, including the establishment of the Healthcare Safety Investigation Branch in 2017, the publication of the National Patient Safety Strategy in 2019,5 and the launch of the Patient Safety Incident Response Framework (PSIRF).14 These take a systems-based approach to patient safety investigation rather than focusing on individual staff fault. This moves away from blame and towards more effective safety recommendations. Such work is also supported by the Clinical Human Factors Group (https://chfg.org/), a charity set up in 2007 to put human factors at the heart of healthcare.
The Healthcare Safety Investigation Branch (HSIB)
HSIB was started in April 2017 to improve patient safety through effective independent investigations that do not apportion blame or liability. HSIB aims to carry out 25-30 national investigations each year. Potential investigations are assessed against four criteria:
Outcome impact - is this an important issue?
Systemic risk - is the incident systemic rather than local, based on a specific team or setting?
Learning potential - can HSIB make new recommendations to improve the system issues present?
Feasibility - can an effective investigation be executed?
Investigation reports are published and make recommendations across the system to national bodies. HSIB also undertakes maternity investigations according to the ‘Each baby counts’ criteria15 under a separate set of Ministerial Directions.16
HSIB drew on experience from other safety critical industries, particularly the Air Accidents Investigation Branch (AAIB). AAIB was established in 1915, 12 years after the Wright brothers’ first flight; it is central to the culture of UK aviation and has been copied internationally. Similar bodies were created for the marine industry in 1989 and the rail industry in 2005. These other safety-critical industries have benefited from systems-based investigations. However, healthcare is complex, and approaches used in other industries cannot always be easily transferred. Furthermore, the principles of incident investigation are culturally accepted, especially in aviation, and these industries also allocate considerable resources and dedicated staff to safety.17
HSIB has from its outset prioritised family engagement and staff support, and has published its experience.18,19 Family engagement in national investigations is 89%.
Systems-based investigations
Healthcare is a complex system made up of people, teams, environments, processes, equipment and technology. A systems-based investigation concerns the complex interactions within its delivery and avoids a linear approach (A causing B causing C). It regards incidents as faults in a system in which individuals are present (as patients or staff), rather than individual fault. A systems-based approach will occasionally identify individual accountability, but only when the system is not the major factor.
Over 100 systems-based investigation models are used in safety-critical industries.20 Examples include AcciMap, which uses a multi-layered diagram of contributory factors, and functional resonance analysis method (FRAM), which examines the variability in a range of the system's functions. These can be complex and require training, and their use depends on the incident's setting and the investigator's conceptual framework.
The Systems Engineering Initiative for Patient Safety (SEIPS) was described by Carayon21 as a framework for understanding the structures, processes and outcomes in healthcare and their relationships. It is a systems approach with embedded human factors principles and is designed specifically for use in healthcare. It has been used in many HSIB investigations including the national learning report on never events22 and will be supported by PSIRF,14 and will therefore be the method most commonly used and encountered by NHS professionals in England. Also specific to healthcare is the Yorkshire Contributory Factors Framework, which similarly takes a systems-based approach to the factors contributing to patient safety incidents in hospital.23,24
SEIPS
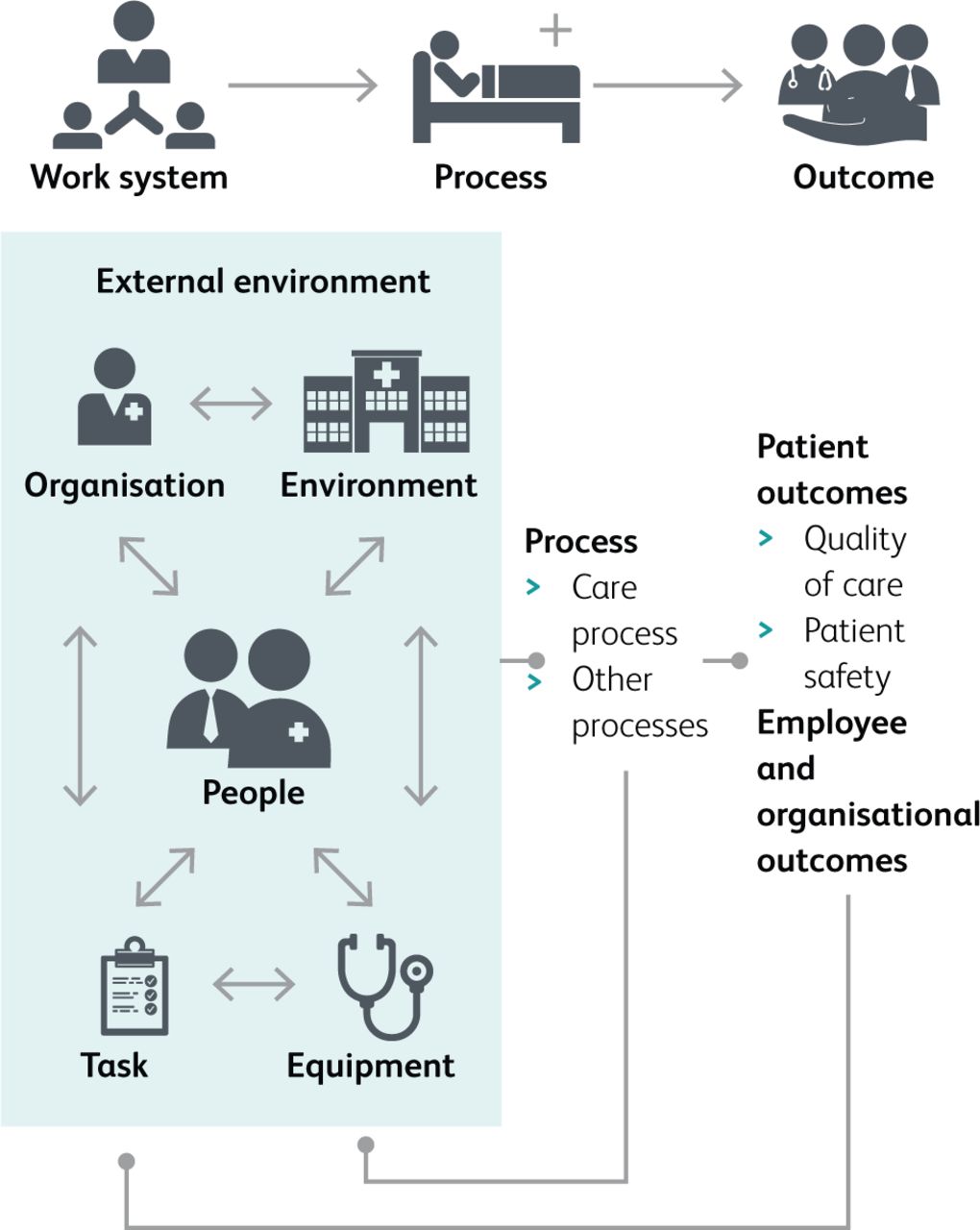
The SEIPS model is based on work systems which comprise interacting structural elements. SEIPS describes how system components result in work processes which may yield different outcomes including an unintended outcome. Work system factors include:21
person(s): the people working in the system and the patient
tasks: undertaken by the persons which may vary in complexity or variety
tools and technology: used to undertake the tasks which may vary in usability and functionality
internal environment: the space around the persons, e.g. layout, noise, temperature
organisation: conditions, resources, and activity within the organisation
external environment: factors outside healthcare institutions that might include policy, societal or economic factors.
Processes can be physical, cognitive, or behavioural and give outcomes for the patients, professionals, or healthcare institutions. The interactions between work system components lead to different outcomes, positive and negative. The framework includes feedback loops representing adjustments made by systems over time. Fig 1 shows the SEIPS model.

Components of the SEIPS model.
SEIPS has evolved since 2006. The most recent published iteration, SEIPS 101, is straightforward for those new to the model.25 It is a simplified, practice-oriented SEIPS model for easy use.
Training
The English national patient safety syllabus26 was produced by the Academy of Medical Royal Colleges and commissioned by Health Education England (HEE). It supports a systems-based approach to patient safety, and domain 2 concentrates on learning from incidents. In line with HSIB and PSIRF, it promotes patient and carer engagement and sets out to avoid blame. The supporting educational materials will be on HEE's e-learning platform during the second half of 2021. HSIB's ministerial directions require promotion of systems-based investigations in healthcare2 and an educational offer is being piloted during 2021 for roll out in 2022.
Effective recommendations from investigations
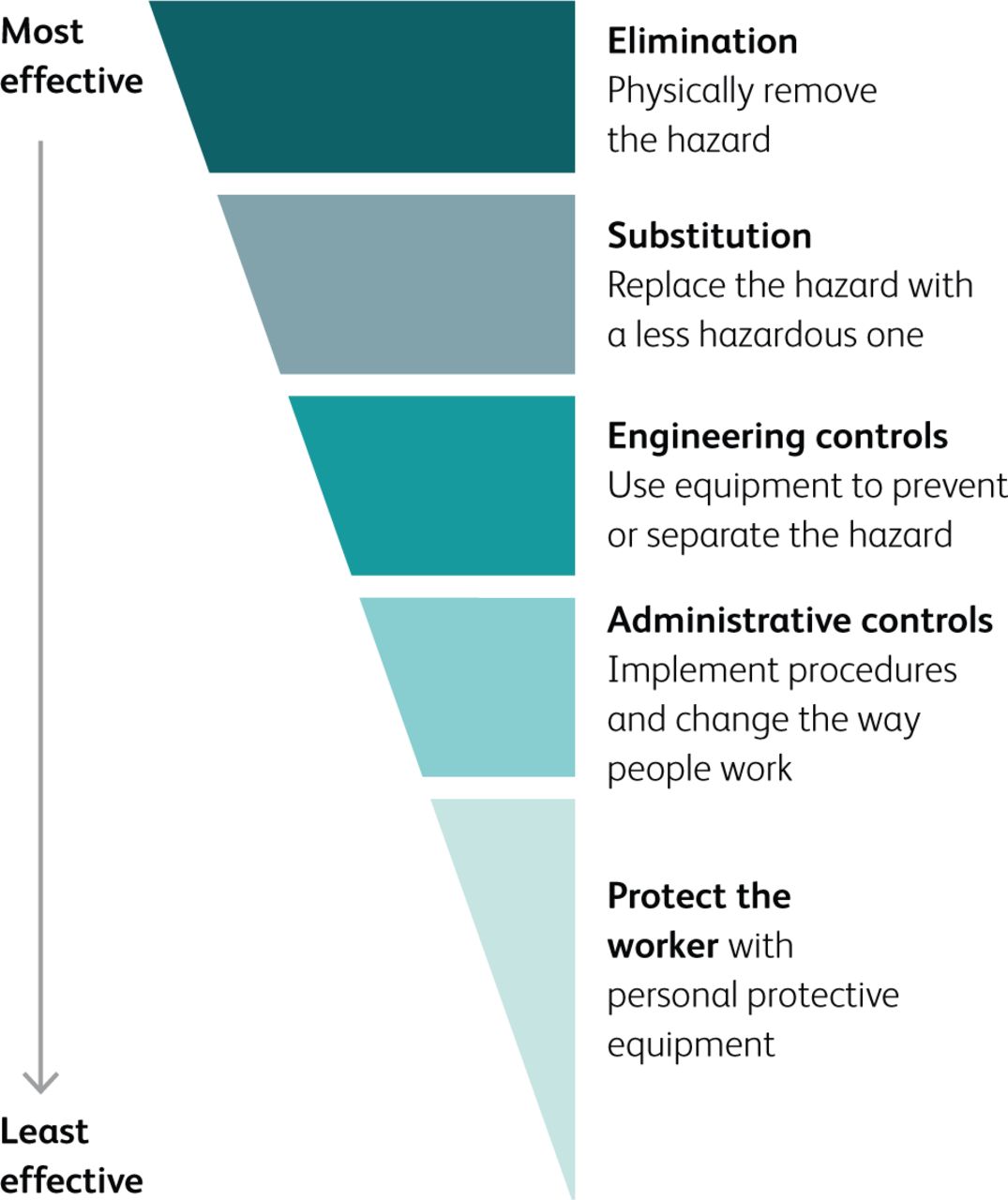
Any systems-based investigation needs effective recommendations to have potential to improve patient safety. A safety investigation may identify a contributory factor or a ‘hazard’ which can lead to a ‘safety risk’. A safety risk may have a number of ‘controls’ - measures expected to mitigate risk of incidents. Some controls may be robust enough to prevent the incident and these would be ‘barriers’. Other controls may not be robust and may be regarded as ‘safeguards’. This concept of some controls being stronger than others is represented in the hierarchy of controls (Fig 2).27 The stronger the controls that are recommended from a systems-based investigation, the more likely that there is a barrier to the event recurring. Education, adherence to policies or procedures, and checklists are relatively weak controls, therefore ‘safeguards’. Unfortunately, research shows that the significant majority of safety recommendations and implemented risk controls are administrative or weak controls.12,28
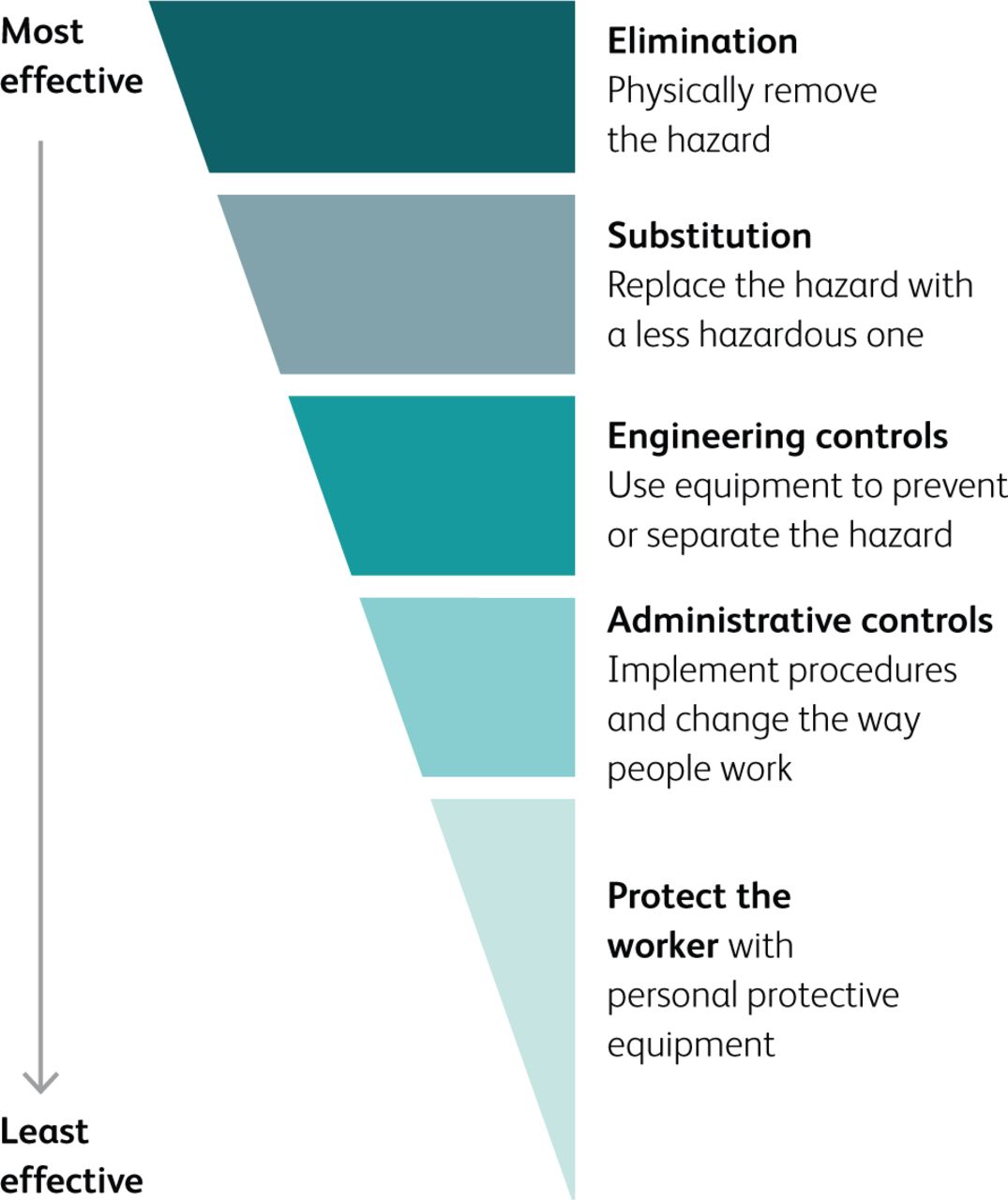
The hierarchy of controls.
When the hierarchy of controls was considered in HSIB's SEIPS-based analysis of NHS ‘never events’, it found that the never events that recurred did not have strong barriers to prevent their occurrence. The never event framework defined incidents as ‘having strong and systemic barriers’ to prevent them, so HSIB recommended that they did not fit the definition and that they should be removed from the never event framework. It recommended that stronger barriers were sought for these important safety incidents.22
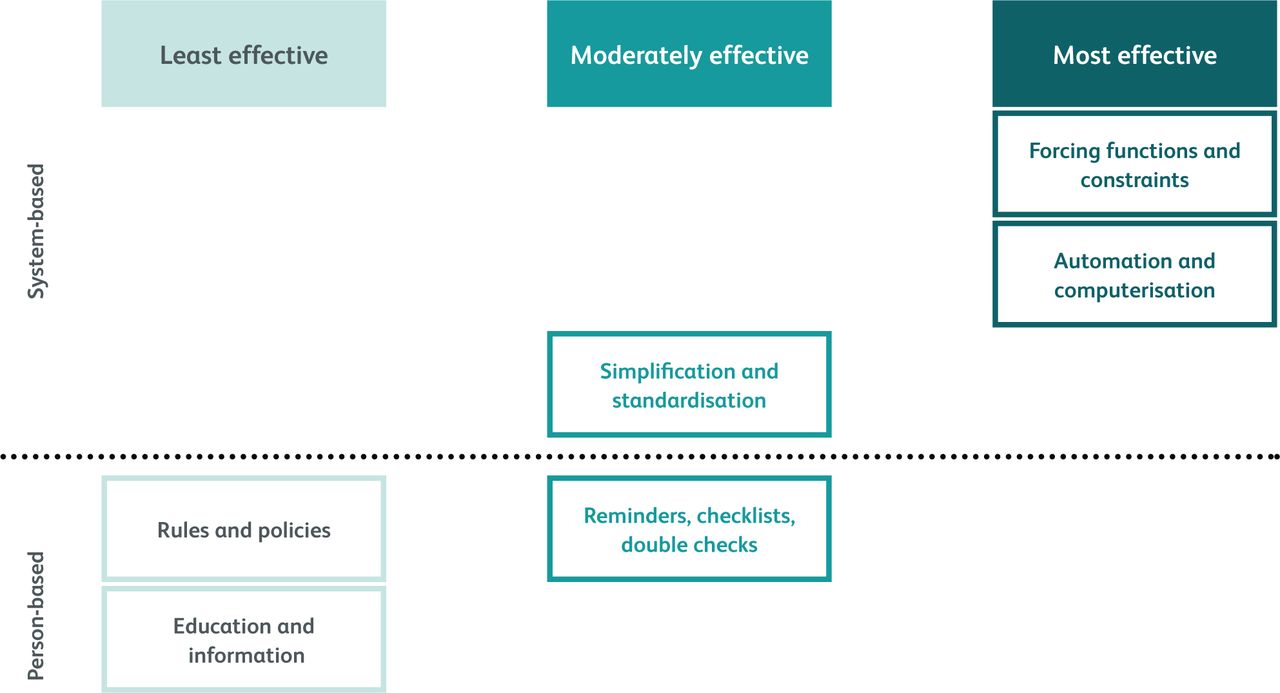
Considering this hierarchy of controls, recommendations from systems-based patient safety investigations are clearly most effective when they also take systems approaches rather than person-centred approaches. This was highlighted in work from Canada which uses a hierarchy of effectiveness of recommendations (Fig 3). This does represent a challenge in healthcare and the predominance of weak recommendations may not just be due to a lack of systems-based investigations but also to the difficulty of finding or implementing stronger controls or barriers. This may be due to the complexity of healthcare, a lesser prioritisation of making systemic changes for safety when compared to other safety critical industries, and a tolerance of weak controls by those working and involved in healthcare.

Hierarchy of effectiveness of interventions. Adapted with permission.29
HSIB is yet to fully prove its efficacy in this environment. It has been objectively successful at involving and engaging with patients and staff in systems-based patient safety investigations that do not apportion blame or liability. It is not a regulator and how its recommendations are implemented and reviewed needs further development. It is possible that a safety management system approach for healthcare may be beneficial on that front.29
Conclusion
Systems-based approaches to the investigation of patient safety incidents in healthcare are more likely to prevent future similar events than investigations which concentrate on individual errors and blame. Investigation models such as SEIPS can be used to explore the range of contributory factors and avoid inappropriate concentration on individual errors or simple linear causation. System-level recommendations are more likely to produce systemic change. Organisations which use systems-based investigations and recommendations when patient safety events occur are likely to improve their safety culture.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.