
Introduction
On 23 March 2020, in response to the COVID-19 outbreak, the UK government announced a lockdown to slow the spread of the virus and protect NHS capacity. It had immediate effects on cardiology services in Nevill Hall Hospital (NHH). NNH provides an acute cardiology service using six coronary care unit (CCU) and 16 ward beds, non-invasive investigations and clinics. Routine angiography and pacing are undertaken at another hospital in the same health board while interventions for acute coronary syndrome (ACS) are carried out at the local tertiary centre on a treat and repatriate basis.
Methods
Data were collected on inpatient occupied bed numbers, number of coronary angiographies for ACS, inpatient and outpatient echocardiographies (ECHOs) and elective direct current cardioversions (DCCV). These data were compared over the same period (March to July) in 2019 and 2020.
Results
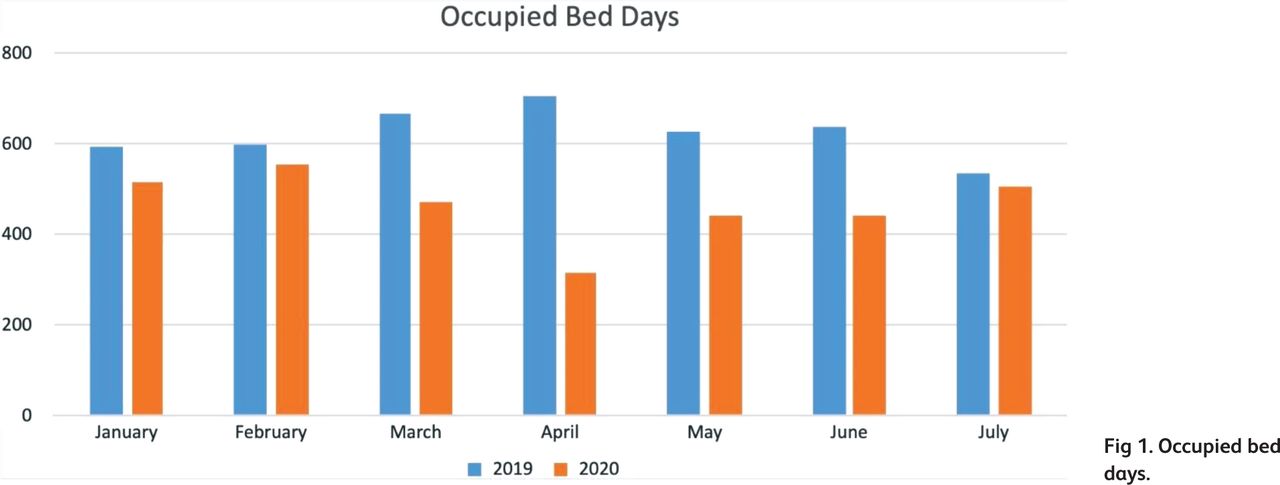
Average inpatient numbers fell from 21 to 8 from March to April, and have gradually increased to match 2019 numbers in July (Fig 1), with a fall in all non-COVID presentations, as reported in the UK.1
The numbers of inpatient ECHOs performed during March to April dropped from 144 (2019) to 38 (2020) while outpatient ECHOs dropped from 233 (2019) to 9 (2020). Inpatient ECHOs then increased to 121 between April and May and 107 between May and June while outpatient ECHOs remained essentially suspended.
Elective DCCV lists, which had eight patients every month in 2019, remained suspended from 23 March to 22 May 2020. Up until 22 July only three patients have managed to be on two DCCV lists.
Inpatient angiography/percutaneous coronary intervention (PCI) undertaken for ACS have fallen drastically (Fig 2).
Outpatient activity has been switched predominantly to telephone consultations.

Occupied bed days.

IP coronary angiography referrals (ACS + complex).
Discussion
These figures starkly demonstrate the effect on a single hospital unit raising concerns that potentially serious conditions go untreated. They build on a worrying trend of reduced cardiac presentations worldwide.
The fall in non-COVID presentations was evident in comprehensive data from Spain which showed a marked reduction in interventional cardiology activity during this pandemic.2 Historically, during the 2003 severe acute respiratory syndrome (SARS) outbreak in Taiwan, fear of catching the virus in hospital had a major impact on visits.3
Overall, the NHS has coped remarkably well. The message that ‘the NHS remains open for business’ must continue to address reluctancy to come to hospital.
There are major long-term challenges in terms of dealing with the backlog of clinics, investigations, procedures and adapting new working patterns and practices. While telephone clinics have proven popular with patients, many need to be seen face to face. Current clinic models could not cope with the same numbers when all interactions take longer. It is imperative that we consider a variety of alternatives as well as better vetting and triage of patients.
Conclusion
Against this background, the current referral to treatment times are unrealistic and careful evidence-based planning should be implemented to minimise disruption to patient care.
Conflicts of interest
None declared.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.