
ABSTRACT
Background The Baveno VI consensus identifies patients with compensated advanced chronic liver disease (cACLD) who can safely avoid screening endoscopy. However, concordance in clinical practice with this guidance is unknown. We audited clinical practice and the provision of transient elastography (TE) aiming to identify potential cost savings and benefits.
Methods Retrospective data collection from 12 sites across London over 6 months by reviewing oesophagogastroduodenoscopy (OGD) reports, platelet count and TE results as well as information on site-specific provision of TE.
Results Three-hundred and fifty-one screening procedures were identified; 177 (50.43%) had a TE test performed within the preceding 12 months; 142 (80.23%) patients with a recent TE test did not meet criteria for screening OGD. TE provision varied widely between sites.
Conclusion Improving concordance with the Baveno criteria through improved provision of TE would have benefits for patients, healthcare systems and the environment and would help to address the challenges of moving on from the COVID-19 pandemic.
Introduction
Acute variceal haemorrhage is a catastrophic complication of cirrhosis and associated with a mortality of 14%–22% at 6 weeks.1 Historically, all patients with cirrhosis would undergo variceal screening at diagnosis, and regularly thereafter, in order to facilitate the prompt initiation of primary prevention measures to minimise bleeding risk.2,3 It is now recognised that patients with compensated advanced chronic liver disease (cACLD) can have their bleeding risk stratified using non-invasive techniques, reducing the burden of invasive procedures on patients with a low pre-test probability of bleeding.1
The Baveno VI consensus identified that patients with cACLD who have a liver stiffness measurement (LSM) of <20 kPa and a platelet count of >150,000 cells/μL are at low risk for clinically significant portal hypertension (CSPH) and varices needing treatment (VNT), defined as ≥grade 2 or those with high-risk stigmata.3,4 It was, therefore, proposed that these patients can safely avoid screening endoscopy and should instead have annual monitoring of LSM and platelet count. These criteria have since been validated in international cohorts, with one study demonstrating a negative predictive value (NPV) of between 0.92 and 1.00.5 Previous studies suggest that between 25%–50% of screening endoscopies can be safely avoided through the use of these non-invasive markers, with significant financial and patient benefit.6,7 Despite the significant body of evidence supporting these recommendations, it remains unclear how rigorously these guidelines are followed in clinical practice.
The current COVID-19 pandemic has further brought this into focus as endoscopy services across the country now face significant strain through an unprecedented backlog of requests and reduced capacity due to stringent infection control protocols.8 Identifying patients who could have screening endoscopies safely deferred could help endoscopy services free capacity and reduce unnecessary invasive procedures and potential exposure to COVID-19 in a vulnerable population.
We therefore audited clinical practice across 12 London hospitals to assess compliance with Baveno VI guidelines and calculated the potential benefits that could be achieved through improved adherence to the guidelines.
Methods
The Gastro London Investigative Network for Trainees (GLINT) is a collaborative group of trainees based at hospitals across London.9 Participation in the trainee network is voluntary and individuals collected data from each hospital site using an agreed pro forma (supplementary material S1).
All sites registered the project through their local audit department where local procedures were followed.
Retrospective data were obtained from electronic endoscopy records at 12 London hospitals. Of the 12 hospitals:
six were tier 1 centres that provide minimal hepatology services such as clinics
four were tier 2 centres that accept hepatology referrals short of transplantation
two were tier 3 (tertiary) liver transplant centres.
Inclusion and exclusion criteria are outlined in Table 1.
Inclusion and exclusion criteria
For each patient who underwent a screening oesophagoga-stroduodenoscopy (OGD) within the study period, LSM (measured in kPa) assessed using transient elastography (TE) and platelet count from the preceding 12 months were recorded from the patients’ medical notes. In those with more than one platelet count result, we used the result closest in time to the TE. We then used these data to calculate how many patients were outside the Baveno VI criteria for the presence of varices needing treatment (VNT) and could therefore safely avoid screening endoscopy. Only those patients with both LSM of <20 kPa and a platelet count of >150,000 cells/μL were considered to fulfil the criteria. As earlier, VNT was defined as ≥grade 2 or those with high-risk stigmata.3
Using national tariff data, the total potential cost saving was then calculated. Follow-up data were collected up to June 2020 to calculate the rate of variceal bleeding.
Data were also collected from the contributing centres regarding the availability of TE. Contributors provided data on the type of requesting system (eg electronic or paper form), the healthcare professional performing the investigation, the average time taken to get a result following the request and the physical location where TE is performed.
Analysis
Secondary points of analysis were calculating the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for VNT. Fisher's exact test was used to compare data between tertiary and non-tertiary centres. Statistical analysis was performed using Graphpad Prism v9.
Results
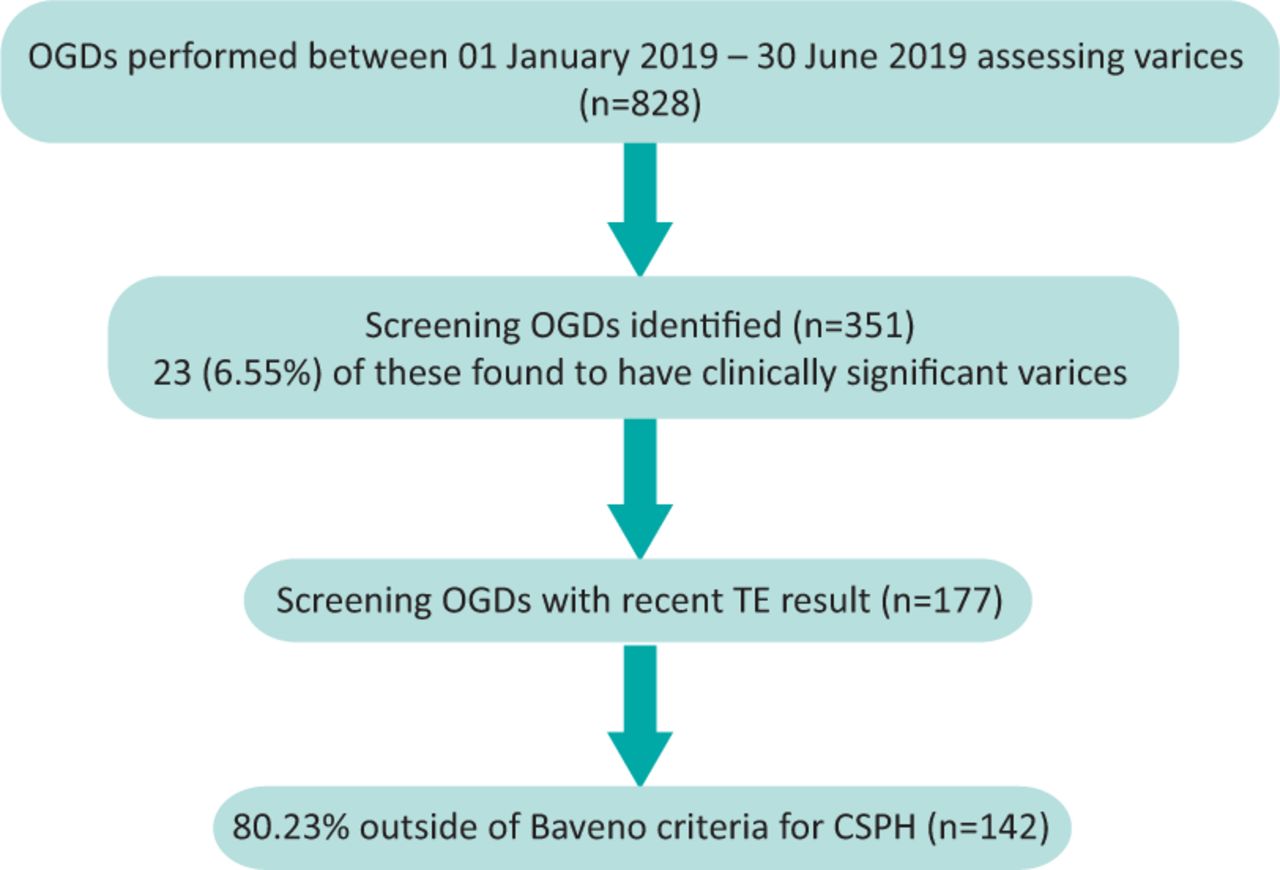
In total, data for 828 OGDs were collected across 12 London hospitals over a 6-month period from 01 January 2019 to 30 June 2019. Twenty-four were excluded due to incomplete data, 173 due to decompensation at the time of endoscopy and 280 that were performed as variceal surveillance, and thus not screening, OGDs. Three-hundred and fifty-one were performed as screening procedures for oesophageal varices and it is these that are analysed herein. The data analysis is summarised in Fig 1.

Endoscopic data analysis. CSPH = clinically significant portal hypertension; OGD = oesophagogastroduodenoscopy; TE = transient elastography.
One-hundred and forty-two (80.23%) of the patients with a TE result (n=177) within the past 12 months did not meet the Baveno VI criteria for screening endoscopy, and 9/142 (6.34%) of these patients were found to have VNT at endoscopy.
Thirty-five (19.77%) patients met the Baveno VI criteria for the presence of VNT necessitating screening OGD and, of these, 9/35 (25.71%) were found to have VNT at endoscopy.
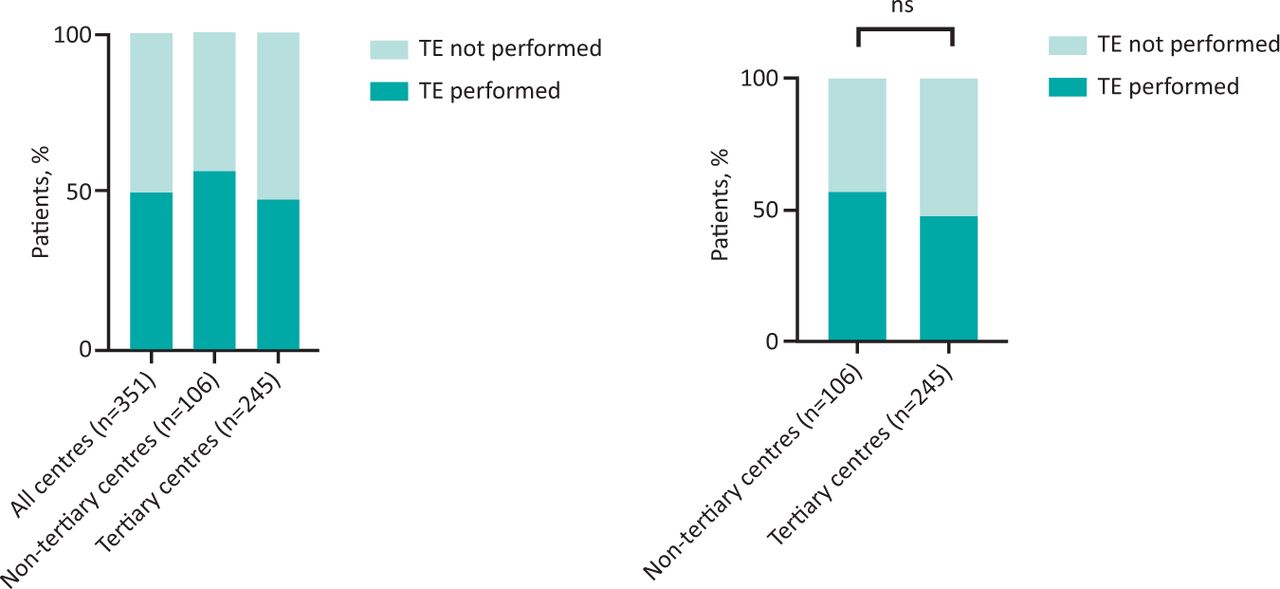
Of the 351 screening endoscopies examined, 177 (50.43%) of these patients had a TE result from within the past 12 months (Fig 2a). One-hundred and seventeen of 245 (47.76%) patients managed at tertiary hospitals had a recent TE result compared with 60/106 (56.60%) patients from non-tertiary hospitals (Fig 2b). The difference between tertiary and non-tertiary centres was not statistically significant (p=0.13). The highest percentage was from a non-tertiary centre with 71.43% compared with the highest performing tertiary centre with 49.18%.
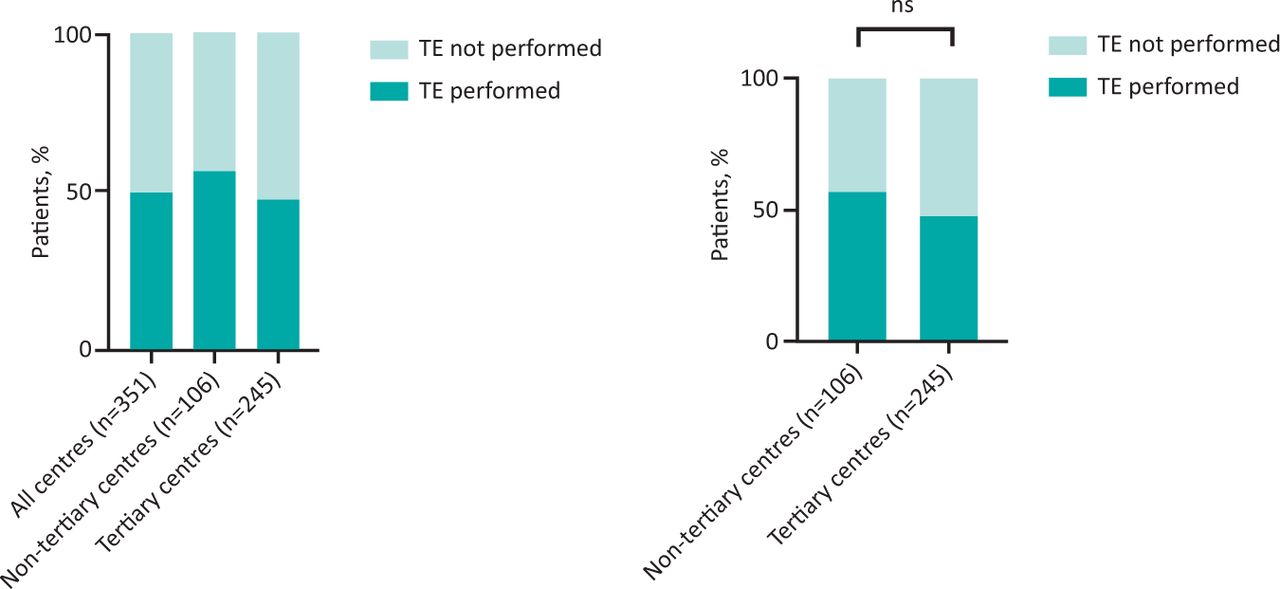
a) Analysis of patients who underwent a screening oesophagogastroduodenoscopy (OGD) showing those who did and did not have a transient elastography (TE) result available from the preceding 12 months. b) Comparison between tertiary and non-tertiary centres regarding the availability of a recent TE result. Statistical significance was assessed using Fisher's exact test.
Using the proposed 2020/2021 national tariff system information, which pays £349 per diagnostic OGD and £41 for a TE exam, this represents a potential saving of £43,736 from this cohort had a TE been performed and Baveno guidance followed.10
Of the 351 screening endoscopies, 23 (6.55%) patients had VNT, while 328 (93.45%) did not. Four (1.14%) patients undergoing screening endoscopy subsequently suffered from a variceal bleed and none of these had an available TE result but all of them had platelet counts below 150,000 cells/μL.
In this cohort, the sensitivity of the Baveno VI criteria for detecting patients with VNT was 50%, while specificity was 83.65%. PPV was 25.71% and NPV 93.66%.
Eight of the 12 centres provided data regarding the nature of the provision of TE. These results are summarised in Table 2. The time taken from request of TE to result ranged from 48 hours to 3 months.
Details of provision of transient elastography at the individual centres that contributed to data collection
Discussion
Our audit has demonstrated that the use of TE and adherence to Baveno VI guidance in current clinical practice across London is poor. Our real-world data showed that 49.57% of patients who underwent screening OGD had not undergone a TE test in the preceding 12 months. We also found that, when examining screening endoscopies, 80.23% of these could have been avoided had the Baveno VI guidance been followed.
The reason for this poor adherence to the Baveno VI criteria may be due to a lack of awareness regarding the guidance, as identified in previous studies.11 Other likely contributing factors include the variation in provision of TE across different sites, as well as possible scepticism from clinicians regarding stopping OGDs in this patient cohort.
Survey data from the sites in our study found large differences in estimated turnaround times after the test was requested, ranging from 48 hours to 3 months, as well as differences in the nature of provision of TE testing. The best performing centres, from both tertiary and non-tertiary cohorts, all performed TE at the time of outpatient appointment in a so called ‘one-stop’ service, whereas the worst performing centres required patients to travel to an alternative site. This suggests that easy-to-access testing may remove a barrier to the use of TE that could potentially improve adherence to the Baveno VI guidance.
This variable provision of TE and poor adherence represents an opportunity to reduce the number of endoscopies performed, which would have multiple benefits for patients, the environment and healthcare systems.
Through establishing a one-stop clinic where patients would be seen by their physician and have TE and phlebotomy performed, they would be required to attend hospital less frequently and would undergo less invasive procedures in the form of endoscopy. This reduction in the number of procedures required to be performed by endoscopy departments would be particularly appealing given the backlog of cases that has developed due to the COVID-19 pandemic.12 Managing this backlog, in the context of the climate crisis, has led to discussions regarding environmentally sustainable healthcare provision.13 Establishing one-stop clinics would offer a low carbon alternative to endoscopy with reduced hospital attendances as well as less medical waste.
There would also be cost savings to healthcare systems. Our data, even in a relatively small audit, identified a potential cost saving of over £43,000 had the Baveno criteria been fully adhered to. While there would be some initial capital cost (such as purchasing of machinery and training of staff), the low cost of each scan (£41) means that initial outlays would be recovered by healthcare systems quickly.10
In our study, the Baveno VI criteria performed worse in terms of VNT missed compared with other studies: 6.4% compared with 2% in a study by Augustin et al.14 The reason for this higher miss rate is unclear and we did not collect specific data on these patients, such as aetiology or comorbidities, which may have helped to explain our findings or potentially prompted the performance of an endoscopy for these patients. However, our study was not designed to robustly validate these criteria, and no patients outside the criteria for VNT went on to suffer from a variceal bleed in the follow-up period. Moreover, not only has the safety of the criteria been repeatedly validated in larger studies, there have even been suggestions that the Baveno VI criteria may still be too conservative and lower cut-offs could be utilised without compromising patient safety.5–7,14
While we believe our audit has raised important points regarding the benefits of following Baveno recommendations, there are limitations in our methodology. While we did not assess the number of screening OGDs that were avoided after patients were assessed using TE, we did demonstrate significant underutilisation of the Baveno VI guidance in clinical practice. We assumed that sites followed recommended guidelines in performing TE on fasted patients and did not explicitly confirm this.
All centres in our study had access to TE, albeit in varying capacity, suggesting that there are additional contributing factors for the poor adherence to the Baveno VI guidance. Future areas of research include a multi-centre assessment of the barriers to its implementation, which could potentially be performed using quality improvement methodology and assessing the timing of surveillance endoscopy, which the Baveno VI consensus does give guidance on, as this could highlight further potential cost savings and benefits as described above.
Conclusion
Our real-world multi-centre study demonstrates that, when risk stratifying patients with cACLD for a screening OGD, adherence to the Baveno VI consensus criteria in clinical practice requires substantial improvement and that there is a wide variation in the provision of TE. Rectifying this represents an opportunity to streamline service provision in a manner that would benefit patients, the environment and healthcare systems.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj
S1 – Pro forma used for data collection.
Acknowledgements
This work was undertaken by the Gastro London Investigative Network for Trainees (GLINT) with data collection performed by Lalana Songra, Metin Yelcin, Khizar Rafique, Rajan Patel, Charlotte Skinner, Saniath Akbar, Jennifer Clough, Sean Carlson, Mohammed El-Naggar, Samuel Tribich, Ava Zamani, Emma Michael, Maria Bashyam, Khin Han, Alexandra Cheng and Alexander Cole.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.