
ABSTRACT
The Getting It Right First Time (GIRFT) process is designed to improve the care of patients in the NHS in England through in-depth review of services, benchmarking and presenting a data-driven evidence base to support change. It started as a pilot project targeting unwarranted variation in elective orthopaedic surgery. It rapidly became apparent that the approach of clinically-led deep dives to review the activity in individual orthopaedic units was effective in improving standards of care but also resulted in substantial cost savings that could be reinvested in the clinical service. GIRFT has now expanded to encompass 40 clinical specialties and is funded by NHS England. We describe the ethos of networks and give examples of GIRFT specialty programmes that have made networks a key component of their recommendations.
What are networks?
Clinical networks should exist to enable patients, professionals and organisations to work together on large and lasting programmes of quality improvement. They should aim to deliver the best outcomes for populations now and for future generations, ensuring equity of access, quality and experience for patients, acknowledging workforce disparities and using innovative digital solutions. They do this by bringing the right people and expertise together with a shared vision to help drive improvements. Networks differ from systems in that they have a voluntary component using a collegiate approach to identify and implement a range of quality improvement strategies.
From the early 1990s, clinicians from different organisations, mostly hospital trusts, came together to discuss ways to improve care for specific conditions, particularly those that resulted in high mortality (heart disease, cancer and stroke). Eventually, these meetings and collaborations became more regular and organised, with policy makers hoping that, through flat organisation structure, shared decision making and more collaborative working, there would be improved knowledge sharing, resource use, problem-solving and service delivery, and hence the first managed clinical networks (the cardiac networks, cancer networks and stroke networks) evolved.
In the process, networks gained formal clinical leadership and project management support. Implementation has not always been smooth, with existing professional hierarchies, external targets and inter-organisational competition confounding the shared vision to improve patient outcomes.
By the early 2000s, managed clinical networks were ‘promoted’ to non-statutory bodies that advised and assisted commissioners and senior management on clinical policies, pathways and innovations to improve care. New ones were formed to preside over large areas, often the size of a region or county, and were usually hosted by a local primary care trust. Managed clinical networks used national and regional priorities to guide their work and looked at local unwarranted variations to advise on service improvement programmes in their region.
Due to their early success, they grew in number and evolved into more complex entities. The 2000s saw clinical networks expand to cover specific cohorts (such as children), functions (such as critical care) and specialties (such as vascular surgery). However, because they often arose from local demand, their remit, funding, staffing and individual programmes still varied considerably. Some networks were also regarded with scepticism by parts of the NHS, viewed as being focused on the ambitions of groups of clinicians rather than the interests of the wider service.
With the NHS reform of 2012/2013, managed clinical networks were amalgamated into a new and more formal structure with independent cardiac, stroke, cancer networks etc, grouped together under a single NHS-funded organisation: strategic clinical networks (SCNs). These were set up to have a more strategic role but did not have the same level of resource as the clinical networks and varied in their ability to promote service change. In some parts of the country, their influence, mandate and funding substantially reduced, such that the network's function effectively ceased.
In the years since, networks have extended further into other disciplines and areas, incorporating palliative and end-of-life care, with the main difference being that their aim is to aid in the local delivery of The NHS Long Term Plan.1
Clinical leadership is a key component to the success of networks
Repeatedly, whether in analyses of major healthcare system failures or in recommendations to improve organisation and delivery of care, leadership within networks is identified as an important factor.2–8 Evidence suggests that delivering high-quality care is influenced by leadership at macro (national/system), meso (organisational), and micro (individual/team) levels.9,10 At the macro level, leadership sets the tone for a whole system, setting policy priorities and shaping regulation (in turn influencing directly both organisations and individual professionals).11,12 At the meso level, leadership sets organisational strategy and engages both local staff and external organisations to support delivery of high-quality care.13–17 At the micro level, patient-facing leaders engage staff to ensure shared purpose and collaboration in providing high-quality care.15,18,19
Peer-to-peer support is also key in high-functioning teams, whether in formal terms of mentoring and coaching, or informal supportive relationships. This has never been more vital than now as we progress through the COVID-19 pandemic and need effective structures to ensure the welfare and wellbeing of our teams. Leadership and culture are already recognised as a key enabler that supports the delivery of high-quality care.
Evidence on improving quality suggests clearly that there is no ‘magic bullet’ in behaviour change: improvement efforts rely on a combination of factors operating at multiple levels; for example, evidence on audit and feedback (a key example of how performance data may be shared to support improvements in quality) notes that sharing data can have a positive impact on behaviour, but that these effects tend to be small and variable.20–23 Further, it is not just what is shared that matters, it is how it is shared. While the quality of the data presented is important, its impact is influenced by several factors, including the credibility of the individual(s) sharing the feedback, whether the feedback is linked to meaningful action plans and the extent to which staff are engaged and facilitated to put change into action (eg whether they have the time and capacity to make changes).24–27
The GIRFT programme has published a summary of its learnings on leadership based on over 1,600 deep-dive visits.28 The Care Quality Commission (CQC) explicitly assesses leadership as part of its review process with healthcare providers to ensure that ‘[an organisation is] providing high-quality care that's based around individual needs, that it encourages learning and innovation, and that it promotes an open and fair culture.’29
The NHS People Plan reinforces the importance of culture through its ‘People Promise’, which sets out a commitment to create a culture that is positive, compassionate and inclusive.30 The People Promise focuses on seven hallmarks of a positive culture:
we are a team
we work flexibly
we are always learning
we are safe and healthy
we each have a voice that counts
we are recognised and rewarded
we are compassionate and inclusive.
Developing integrated stroke delivery networks across England
The clinical case for networks in stroke care is based on strong evidence that investigations and interventions (such as brain scanning and thrombolysis) can best be delivered as part of a 24/7 networked service, including initial assessment and intervention units (now to be known as comprehensive stroke centres (CSC) or acute stroke centres (ASC)) that admit above a safe minimum number of acute patients with stroke a year.31 The National Stroke Strategy, published in 2007, first made the case for major system change in acute stroke services, creating ‘hub and spoke’ networks of ‘hub’ hyper-acute stroke units (HASUs).32 Creating integrated stroke delivery networks (ISDNs) are an evolution of this, bringing commissioners, community and third-sector partners into the network, with funding and governance structures to support and sustain improvement (Fig 1).33

The 20 individual integrated stroke delivery network regions grouped (by colour) into the seven NHS England regions. BNSSG = Bristol, North Somerset and South Gloucestershire; BSW = Bath, North East Somerset, Swindon and Wiltshire; ICS = integrated care system. Adapted with permission from NHS England. Integrated stroke delivery network footprints. NHS, 2020.
Several stroke pathway optimisations, based upon a networked approach, have been implemented before ISDNs came into fruition, the highest profile being London and Greater Manchester. Independent research found that such systems saw significant improvements in patient outcomes and care delivery, and that systems of this kind were cost effective. Research has also shown that improvements associated with such systems can be sustained over time. Importantly, the benefits of networks of this kind were most likely to be achieved if all patients accessed the hyper-acute element of stroke care, rather than just a selection eg within a specific time frame from symptom onset.31
Networked configurations with HASUs have led to a 5% relative reduction in mortality at 90 days and reduced length of stay.34 An evaluation of networked provision in Northumbria demonstrates value from a networked approach in rural areas. The average annual benefit of full national reconfiguration is estimated to be around €48 million, accounting for a reduction in staff costs, and increased ambulance costs, transition costs and future tariff payments.35
A second critical function of clinical networks is to coordinate, facilitate and sustain change. They may have responsibilities around workforce competency and development, and freedom to develop local data dashboards to inform the selection and focus of local priorities, and monitor change. Research on implementing major system change in London and Greater Manchester describes how local clinical networks played important roles in planning, implementing and sustaining change.
Our own experience from meeting every acute stroke service in England is that local leadership and coordination across services is variable. The intention is that ISDNs provide a framework that will support stronger leadership to drive and manage change across their areas. ISDN leadership teams will be in a unique position to evidence, coordinate and lead change among members of their local providers.
One of our reflections from our very first GIRFT stroke visits in 2018 was the obvious benefits of shared learning between providers, commissioners and the third sector, acknowledging that these groups functioned better when working together in a network. The NHS Long Term Plan now highlights this vision and ISDNs are operational in all areas of England, bringing people and organisations together to deliver the best possible care for their population.1 This model is hoped to be an effective way to improve standards of health and social care outcomes for patients with stroke. We believe that ISDNs are essential to delivering the individual commitments of The NHS Long Term Plan for stroke.36
ISDNs became operational from April 2021. ISDNs should be responsible for designing and delivering optimal stroke pathways for their local populations, making sure that more people who experience a stroke receive high-quality specialist care; from pre-hospital through to rehabilitation and life after stroke.35
There are three key delivery goals of ISDNs, highlighted in the national service model.
Best practice personalised stroke pathways: configured and managed from pre-hospital care onward, including ambulance, thrombectomy, integrated community stroke service model and 6-month reviews within initial implementation, building to include the full pathway from prevention through to life after stroke.
A flexible, future-proofed competency-based stroke workforce: supported by a skills and capabilities framework and toolkit.
A comprehensive dataset: meeting the needs of clinicians, commissioners and patients describing the quality and outcomes of care provided.
The formation of ISDNs should be coordinated with integrated care systems (ICSs) and sustainability and transformation partnerships (STPs). Many ISDNs will align with existing network structures (Fig 2).37
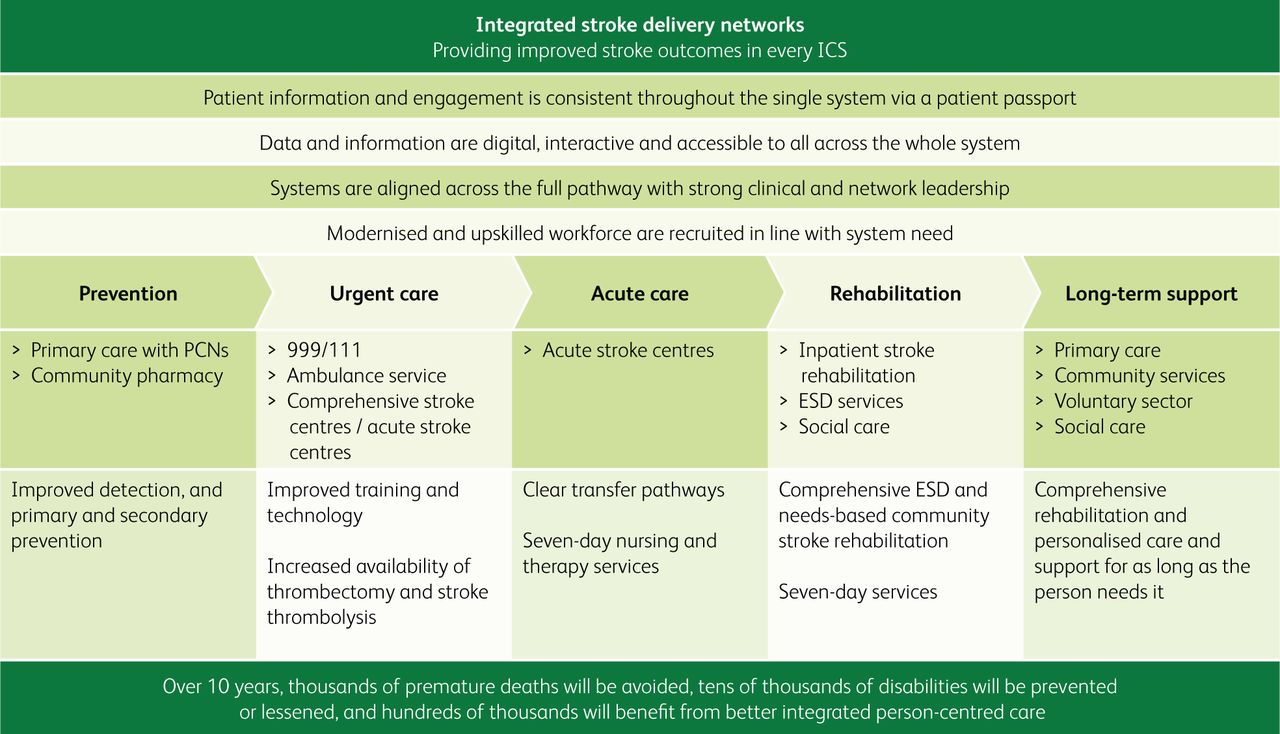
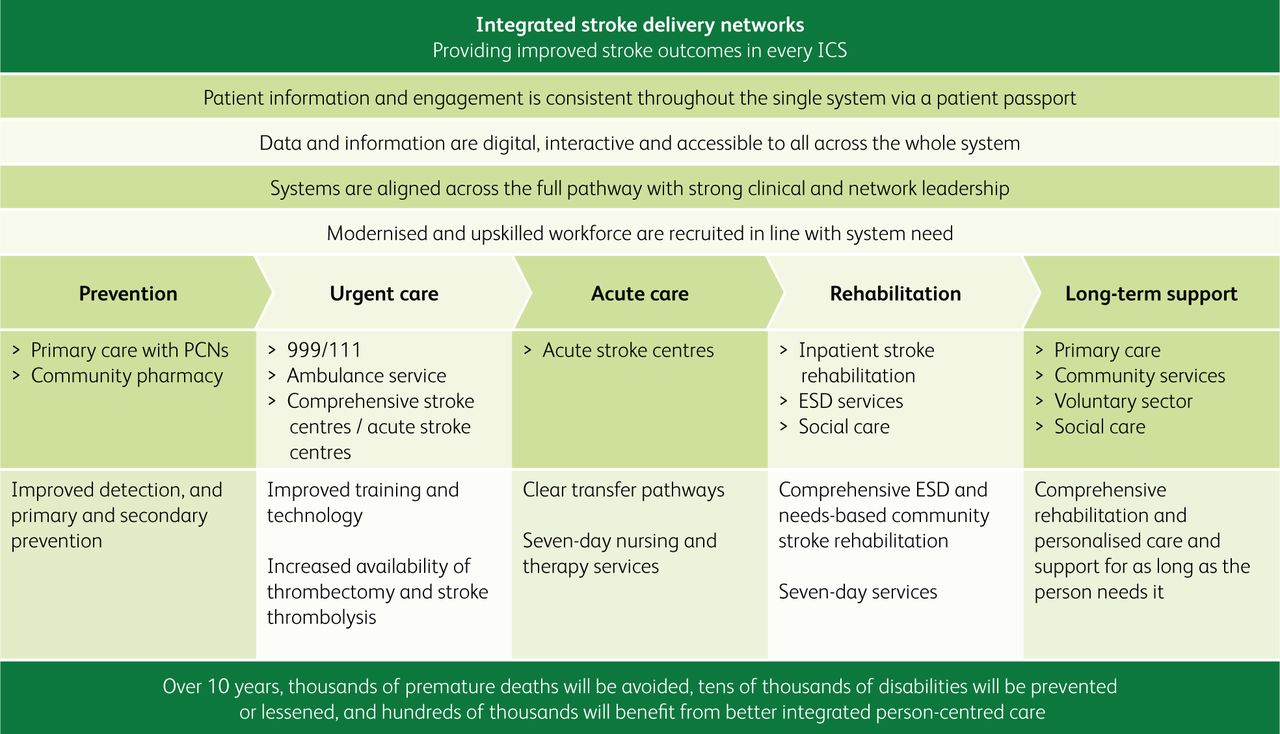
The responsibilities and breadth of integrated stroke delivery networks covering the entire stroke pathway. ESD = early supported discharge; ICS = integrated care system; PCNs = primary care networks. Adapted from NHS England. National stroke service model: integrated stroke delivery networks. NHS, 2021.
An important feature of the ISDN specification is that it defines a clear set of objectives that should be achieved. These objectives are clinically driven and focus on the enabling factors that will support success, including ensuring representative leadership from across the stroke pathway, including patients.
There are four immediate objectives of ISDNs.
Leadership: The provision of robust clinical and stroke programme leadership, which includes medical, nursing and therapy senior leadership to ensure both the acute and community pathways are given equal focus.
Strategic approach: ISDNs should support ICSs, work collaboratively with ICSs and provider workforce leads to manage system capacity, and to demand and develop robust workforce plans. ISDNs should participate in national forums to ensure that, as healthcare technologies advance and new intelligence is introduced, the local workforce is supported to develop and deliver innovations in patient care.
Optimal configuration and collaboration: ISDNs must support the delivery of an optimal configuration of stroke services within their geography and lead collaboration with stakeholders and partners. This collaboration should extend to agreed pathways and ways of working with adjacent specialisms (eg neurology and rehabilitation) and networks (eg imaging networks and vascular networks). They must also manage cross-boundary issues (both geographic and across primary, secondary, community and voluntary care sectors).
Data, digital, monitoring and reporting: ISDNs must ensure full engagement with national programmes (such as the Sentinel Stroke National Audit Programme (SSNAP)) and support the delivery of recommendations suggested from NHS England, NHS Improvement and the GIRFT stroke programme. ISDNs should use innovative technology to improve the patient experience and quality of care: examples include the use of artificial intelligence for brain scan interpretation and pre-hospital telemedicine. Dashboards, using recent data, should be used to ensure performance.
The ISDN national stroke service model (NSSM) also includes a detailed summary of best practice care within each stage of the stroke pathway. This evidence is based on a review completed by King's College London with supporting input from our visits.38 While ISDNs are not expected to be meeting best practice on every step of the stroke pathway, the NSSM gives clear goals and guidance on what ISDNs should be aiming for and how.
Networking in cardiology
The GIRFT report for cardiology identified significant structural problems with the provision of cardiology services.39 In many instances, delivery of care was based more on competition between institutions than on collaboration, with hospitals focused on the development of their own services as a means of securing and retaining income and clinical prestige, rather than on the coordinated delivery of care to a population. Competition between providers resulted in perverse incentives to develop or continue services in isolation rather than to focus on consolidation and collaboration. As a consequence, referral pathways were sometimes outdated and illogical, owing more to the personal or institutional allegiance of clinicians than to any concerted attempt to provide joined-up care to patients. Many of these anomalies were well recognised and longstanding but had never been addressed, as they were perceived as being too entrenched and, therefore, not sufficiently high on the priority list of overstretched commissioning teams.
It is also important to recognise that cardiology is evolving rapidly, and this too impacts on the way that services need to be provided. Many hospitals acquired catheterisation laboratories following the publication of the National service framework for coronary heart disease in 2000 and the subsequent drive to widen access to coronary angiography.40 Improved non-invasive imaging is now largely removing the need for coronary angiography as a purely diagnostic procedure on the stable chest pain pathway and, as a consequence, there is a rapidly declining need for cardiac catheterisation laboratories that perform diagnostic angiography but not coronary intervention. Catheterisation laboratories are expensive to run and require specialist staff to operate. We found instances of hospitals running laboratories at reduced hours, close to other institutions with similar underused capacity while, at the same time, there was insufficient access to non-invasive imaging, particularly computed tomography coronary angiography, recommended by the National Institute for Health and Care Excellence (NICE) as the investigation of choice for the majority of patients on the stable chest pain pathway.
It rapidly became evident from the first 30 or so deep dives that the current model for cardiology was neither sustainable nor delivering a uniformly high standard of care to patients. The overarching recommendation of the GIRFT national report for cardiology is that services should be reorganised and delivered on the basis of functional networks. It defined six common cardiology pathways that should be completed within a network: heart failure, stable chest pain, unstable chest pain, valve disease, endocarditis and heart rhythm abnormalities. This structure means that each network must have at least one cardiac surgical centre within its footprint, and there is envisaged four possible levels of service within each network (Fig 3).39 It also recognises that for some low volume or highly specialised activity, formal inter-network pathways will be required.
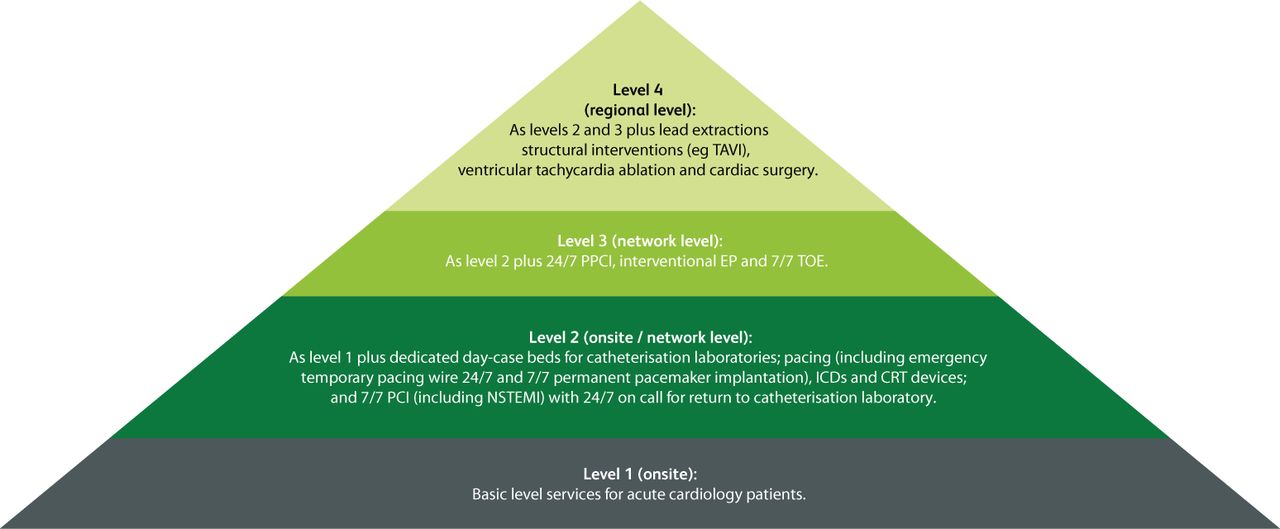
Cardiology network levels of service. All hospitals must be a part of a network with access to all four levels; supra-regional centres will provide more specialised services for more than one network. CRT = cardiac resynchronisation therapy; EP = electrophysiology; ICDs = implantable cardioverter defibrillators; NSTEMI = non-ST segment elevation myocardial infarction; PCI = percutaneous coronary intervention; PPCI = primary percutaneous coronary intervention; TAVI = transcatheter aortic valve implantation; TOE = transoesophageal echocardiography. Adapted from Getting It Right First Time. Cardiology: GIRFT programme national specialty report. NHS, 2021.
The network will need to coordinate care across its footprint. This means that decisions about planning of future services needs to be done on a network basis rather than by individual institutions. To go back to the example of cardiac catheter laboratories, the networks will need to determine how many are required to provide the services for their population that are detailed within the GIRFT report. This will require considering the potential for closing laboratories that are not running to full capacity and consolidating activity on a smaller number of sites, such that expensive facilities are used in the most effective and efficient way. The flip side of that particular coin is that non-invasive diagnostic capacity needs to be increased, should be accessible to all patients within the network and so, by definition, must be available outside tertiary centres.
The network model also facilitates two other key areas of service provision. The first is flexibility of the workforce, such that those members of the wider heart team who are able to can contribute to the service across multiple sites without having to seek additional permissions. This allows scarce skills to be utilised to the maximum benefit of the population served by the network. The second is the embedding of network-wide virtual multidisciplinary meetings (MDMs) within locally agreed patient pathways.41 This will facilitate streamlined decision making, avoiding serial or duplicate investigations and allow all appropriate clinicians within the network to contribute to the decision-making process.
The model proposed in the GIRFT cardiology report has been adopted by NHS England and NHS Improvement.39 There are 15 cardiology networks being established across England under the auspices of the Cardiac Pathway Improvement Programme (CPIP), led by Prof Nick Linker, national clinical director for heart disease. The scope of the networks has been expanded to include primary care, prevention and rehabilitation in addition to the secondary and tertiary care elements that were the focus of GIRFT.
Networking in pathology
The concept of networks of pathology services was first introduced in a consultation paper, Pathology – the essential service: draft guidance on modernising pathology services, published by the Department of Health in 2002.42
Establishing pathology networks has been a recurring theme in central guidance since then, including the two ‘Carter reports’ that followed reviews of pathology services chaired by Lord Carter of Coles.43,44 Perceived by many in the specialty as simply a tool to drive down costs at the expense of quality while at the same time opening the door to privatisation of pathology services, there were few early adopters.
The identification of ‘variation’ of provision by the NHS, in both resource utilisation and productivity, across all aspects of non-specialist acute hospital care (described in a 2016 independent report for the Department of Health also by Lord Carter of Coles), became a driver for change.45 In September 2017, NHS Improvement announced an outline structure of 29 pathology networks in England, with a target date for formation by 2021.46
The GIRFT pathology project commenced data gathering in 2018–2019, using a questionnaire sent to individual departments for completion together with limited nationally available information. It became clear from the trust responses that, although some were already starting to collaborate, the majority continued with longstanding work patterns. However, as we analysed the data, we recognised that there was likely to be benefit for organisations to review the variation across their proposed network, as well as seeing it against the national background picture, regardless of the stage of development that they had reached. We, therefore, offered to conduct deep dive visits on a network basis.
Although agnostic to network structure at the outset, through undertaking the visits, we saw features that were associated with faster progress towards successful network development, and that the more established networks were better able to drive improvement in the quality of their services. Embedded clinical and scientific leadership, engaging staff in service re-design and ongoing dialogue with users are important markers for success. However, network structures need to be allowed to adapt to local needs and geography. We saw a traditional ‘hub and spoke’ model working well in some areas, whereas, particularly in the larger networks, a distributed model that included several laboratory ‘clusters’ across the area had been successfully adopted. Mapping the network to a local ICS or group of ICSs also worked well in some areas.
Across the country, we saw significant variation in all of the measures that we looked at; examples include rates of requests for any given analyte, approaches to timely delivery of results and use of nationally agreed reference ranges. In the GIRFT pathology report, we have described an over-arching framework for pathology (the ‘clean framework’) to help widen the focus beyond the walls of the laboratory and include other issues that impact on the ability to provide a high-quality service. Examples include sample management, such as pre-analytic stabilisation and transport times, which frequently has an adverse effect on the quality of the sample when it reaches the laboratory for testing and, thus, on the reliability of the results generated. There was also a surprising variation in the approach to result issue (the output of pathology services), such as locally derived reference intervals, turnaround times, the use or not of national guidance on re-test intervals, and more. These impact on understanding and interpretation of results, potentially leading to confusion among users and patients, and adversely affect the quality of the service. We saw examples where unwarranted tests, generating unexpected results and/or repeat testing, provide a poor patient experience. We also saw how networks with high levels of training and support for all grades and types of staff had been able to increase both staff and user satisfaction, driving better recruitment and retention in challenging times.
For networks to understand and monitor their performance, staffing and other measures, access to data is essential. A significant finding was the variable availability of high-quality, easily accessible and comparable data. At the patient and clinician level, being unable to see results of tests or even what tests have been taken (for example, when moving across clinical settings) leads to frustration and potential duplication and delays in care. At the network level, ‘business intelligence’ and service delivery is likely to be adversely affected. As networks develop, urgently tackling this variation, agreeing common data standards and coordinating the provision of interoperable systems is essential.
Through a clear governance framework, establishing consistent network-wide standards, sharing best practice, benchmarking and audit, networks become drivers for improved quality. Importantly, the GIRFT focus on quality from the perspective of the service user (through reducing variation and unwarranted interventions) generates savings through improving rather than at the expense of quality (Fig 4).45

Flexible pathology networks that reflect local needs. ICSs = integrated care systems; POCT = point-of-care testing. Adapted from Getting it Right First Time. Pathology: GIRFT programme national specialty report. NHS, 2021.
Patient and public involvement
Active involvement of service users is essential if networks are to be responsive to the needs of the population they serve. This is particularly the case when considering optimisation of particular services within a network to concentrate expertise and allow continuous provision of expert care. Examples of this are hyper-acute stroke care, primary angioplasty for acute myocardial infarction and services for acute aortic dissection. In all instances, the lived experience of patients who have benefited from this type of service or who have suffered from its absence is a potent driver for change, even in the face of clinical or political opposition.
The involvement of service users cannot be a passive process and has to be actively sought out and supported. Networks will need to provide appropriate training to lay members of network committees or panels and ensure that, where appreciable time is spent on network business, it is appropriately compensated.
Conclusion
The COVID-19 pandemic has been a difficult time; we have seen some of the best and the worst of the NHS. Often out of adversity, however, there is great innovation, adoption of new practice and emergence of great leaders. We need to continue to work smarter and collaboratively if we are going to maintain and hopefully improve patient care in the NHS. Reducing duplication, siloed working, unwarranted variation in service delivery and improving standards of care are essential. The significant workforce challenges that exist within health and social care need a joined up, innovative approach, that is much more easily served by clinical communities working together rather than in competition.
Where networks work, they broker collaboration, manage change and facilitate inter-organisational learning. They must be adequately resourced and staffed, and have ‘teeth’ to drive the changes required for sustainable high-quality healthcare. They must have a clear voice in the new operating structure of the NHS and be closely linked, with clear lines of governance and accountability to the seven NHS England regions and, importantly, the integrated care boards (ICBs).
Networks need outstanding, compassionate leadership with effective and inclusive cultures, empowered agents of change and a shared vision. Effective digital enablers and communication of shared-based practice pathways across local trusts and networks must be driven by high-quality data, which will result in many of the improvements we need to see. We need agile data platforms that enable connectivity and a single source for performance monitoring.
In combination with the proven GIRFT methodology for quality improvement and using relevant data and clinician-led programmes of work, there is a framework for us to support our workforce to deliver the best care to patients in the most efficient and effective way.
The expression ‘The whole is greater than the sum of its parts’ aptly describes the concept of collective power, synergy and potential of networks.
- © Royal College of Physicians 2022. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.