
ABSTRACT
Changing population demographics and needs are resulting in a continual rise in acute medical admissions. This review draws on the observations of the NHS GIRFT programme across England. Fundamental aspects of acute medical care are not universally provided, resulting in preventable hospitalisation and over-use of emergency departments. Such aspects include care outside hospitals; appropriately sized, staffed, located and configured acute medical units; multispeciality same-day emergency care (SDEC) pathways; multidisciplinary care on wards; and readmission prevention. ‘Hospital at home’ services are developing, and require local evaluation. SDEC is expanding. Digital technologies make it possible to provide acute care in and across more settings. Addressing the fundamentals of acute medical care, evaluating new service opportunities, strong clinical and managerial partnerships, better data for analytics, and a multispeciality, multiprofessional approach will enable a better level of care to be achieved.
Introduction
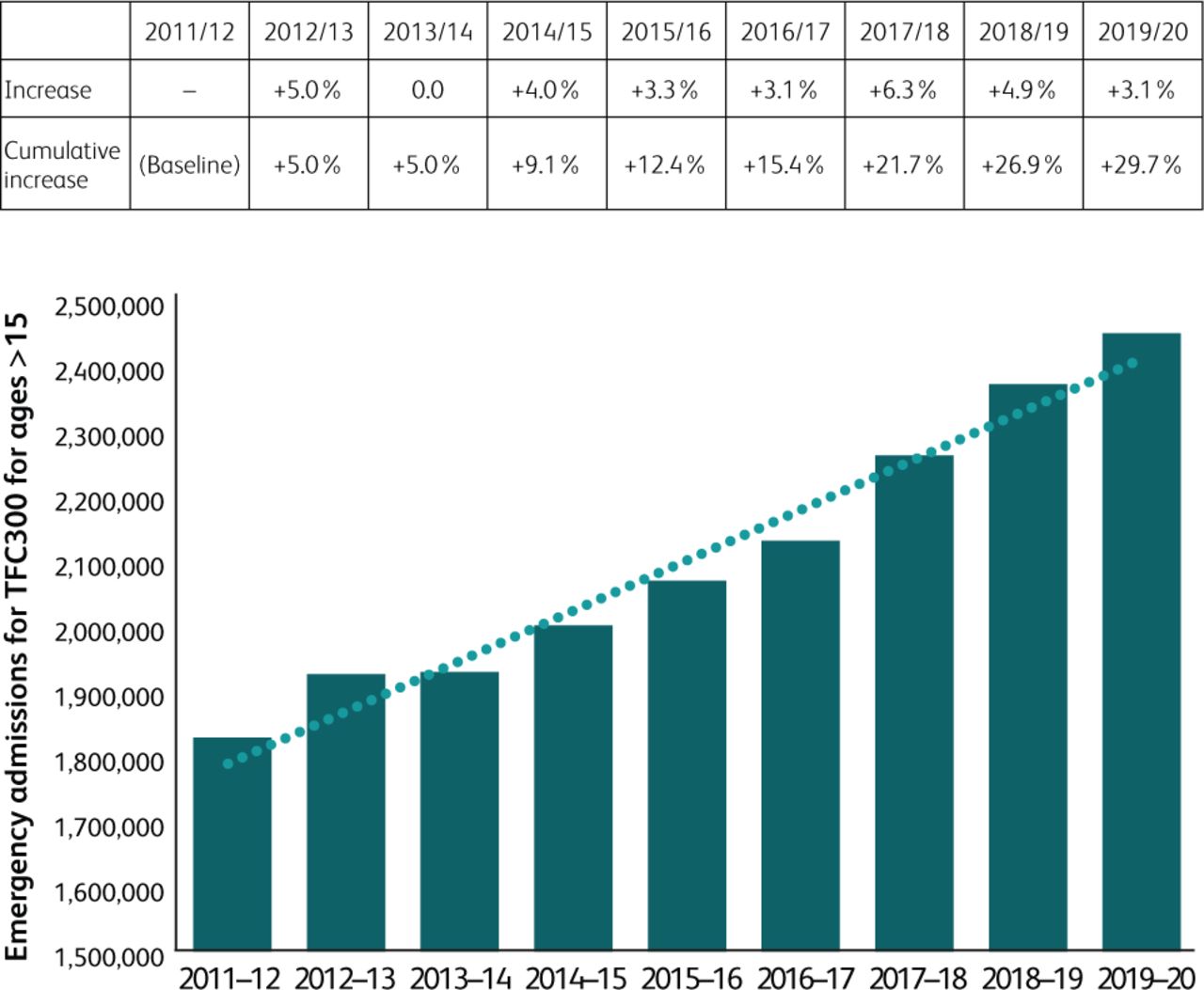
Changing population demographics, increased numbers of available treatments and public expectations are causing a continual rise in the demand for acute medical admissions to hospital (Fig 1).1 People are living longer with multiple medical conditions,2 there is increasing polypharmacy3 and new approaches to treatment and clinical risk increase the need for clinical investigations. Populations are culturally diverse,4 further increasing the complexity of acute medical care and decision making.
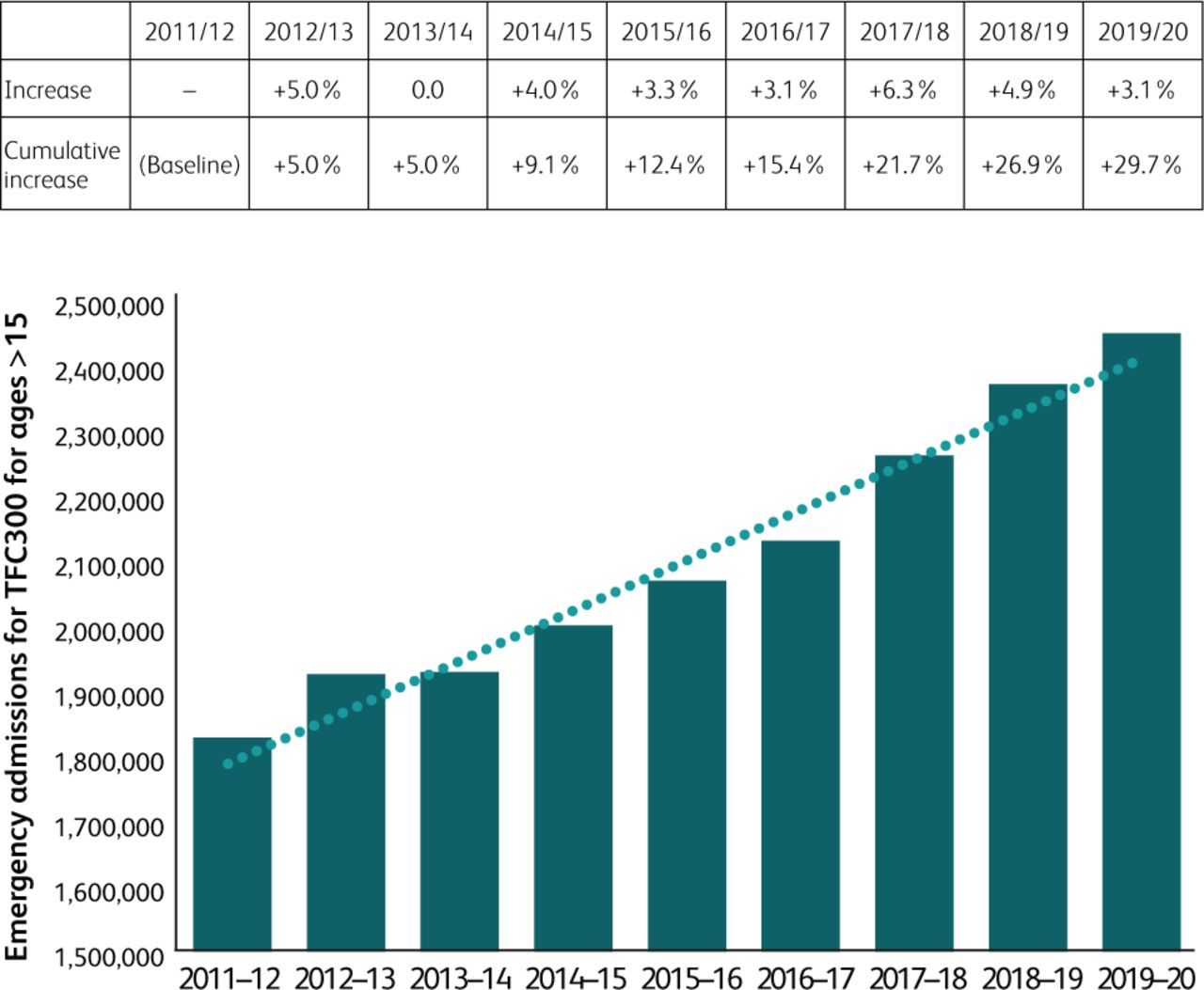
Annual increase in emergency admissions in the NHS in England from 2011 to 2020.1 Data source HES APC, 2011 to 2020.
Acute medical care commonly manages the exacerbation of a known condition, often in the setting of multiple morbidities or frailty.5 Frail older people nearing the end of their lives may present with acute deterioration. Although multiple alternatives to admission have been developed for these and other patients, they are not systematically applied or consistently available throughout the NHS.
The local geography, demographics and hospital configuration also influences acute medical care. Hospitals serving smaller populations, often in more geographically remote or coastal areas, may find recruitment and retention of staff more challenging, and have fewer specialist services.6 Hospitals may also need to configure services differently to meet local needs.
All medical specialities have an integral role in delivering acute medical care. The Royal College of Physicians (RCP), together with NHS GIRFT medical leads, has published a position statement outlining key aspects.7
In this article, we explore how care could be delivered in the future to address current and future acute medical needs within the NHS, drawing on examples of practice across the UK. We emphasise the fundamental elements of provision that must be prioritised, in addition to emerging opportunities that require local adaptation and evaluation.
These are summarised in Boxes 1 and 2. Workforce availability is the major constraint. Examples of innovative practice that have been successful in one setting and show potential to be replicated and evaluated more widely are shown in Table 1.8–12
Examples of innovative practice
Fundamentals of acute medical care
Developing models for local adaptation and evaluation
Care outside the hospital
Many acute medical presentations are exacerbations of chronic conditions.5 Patients should have pre-emptive self-management plans that can be supplemented as required by acute advice from primary care or specialist teams; this requires mechanisms for urgent contact. Support can include early support from community-based healthcare teams, rapid access to speciality teams and units, or ‘hospital at home’ services. The National Audit for COPD and Asthma 2019/20 report found that only 61% of patients had a self-management plan on discharge from an acute admission of COPD in England Scotland and Wales, and 27% an emergency drug pack.13 In inflammatory bowel disease, it is recommended that patients should have access to a dedicated helpline. Although 98% of hospitals in England report this, patients report difficulties in accessing these at times.14 Simply ensuring self-management plans for all patients and improving access to advice would prevent many unnecessary admissions.
Patients with newly presenting conditions or undifferentiated symptoms may initially present to primary care, or seek advice from telephone advice centres such as NHS-111 or NHS-24. These services use clinical decision tools such as NHS pathways15 to give advice on self-management and direct the patient where to present for further assessment and advice if required. It is essential that local healthcare systems and advice centres agree and coordinate these access points. However, more than 60% of nationally recommended alternatives to hospital admission are not consistently available (C Moulton, personal communication). This may result in overuse of emergency departments (EDs) and emergency ambulance services.
The NHS in England is working towards patients having an assessment within their home within 2 hours of contact for a health or care crisis by community-based teams. This can supplement ambulance service paramedic assessment.16 While a considerable commitment for constrained community health and care services, this has the potential to prevent attendance to hospital for some. Links with other services to aid ongoing acute care may be necessary. The possibility of video links from the home to specialist from paramedics or community based urgent assessments has potential (Table 1).
Point of care (POC) testing in conjunction with clinical assessment has been demonstrated to reduce hospital conveyance in a population of the frail elderly.17 Joining these additional services to acute specialist assessment, such provided by an acute medicine consultant or SDEC service, AMU or the ED, can further assist decision making on whether conveyance is needed and also on which unit or department is best suited to receive the patient. It is important that all areas work together in a coordinated way.
Primary and community practitioners should have direct phone access to specialist medical advice within normal hours, enabling more holistic and appropriate initial assessment. A system to capture semi-urgent details outside of these times so the patient can be contacted the following day is required. The on-take team with registrar on-take can provide urgent opinion out-of-hours, but should be trained in how to provide access to local alternatives.
Initial assessment
The aims of initial assessment of acute medical patients are shown in Box 3.18
Aims of initial assessment of acute medical patients
Access to health and care records is essential for such assessment and can be achieved by bringing together current electronic systems (Table 1). As a minimum, there should be access to GP record summaries. Patient-held records and care plans, such as insulin passports,19 can also enable better transfer of information. Unfortunately, this is often hindered by poor IT infrastructure and maintenance, leading to problems such as inadequate access to hardware and software in the appropriate location and multiple logins being required. This creates significant inefficiencies and safety risks.
Using a common assessment approach for physiological measurement helps to determine illness severity. NEWS220 is performed by all hospitals and ambulance services in England and increasingly by emergency primary and community care services. NEWS2 provides a common language of illness severity and can help determine urgency and identify the most appropriate location for more detailed assessment and care.21 Changes from baseline are helpful, and some patients and health records have this information, often using technology at home. Risk stratification tools have also been developed for a number of clinical conditions, such as community acquired pneumonia22 and pleuritic chest pain,23 and these can also help determine urgency and best location of assessment and care. They must however be evaluated for each care setting.
EDs aim to stabilise the patient, identify the need for time-critical treatments and investigations and commence these where appropriate. The working diagnosis and illness severity dictates the best location for ongoing care. However, in England, currently 40% of attendees have already spoken to a healthcare professional before ED.24 This suggests that there is greater potential to direct patients to an alternative route rather than the ED, if the mechanisms discussed above for telephone advice were in place. The increasing percentage of medical admissions from emergency departments rather than from community-based practitioners (Fig 2) suggests that out-of-hospital assessment and direct admission are underutilised, causing unnecessary delays. Furthermore, increased illness severity on attendance and admission at weekends appears to be due to differences in out of hospital service access.25

Emergency admissions from emergency departments vs GP direct access 1990 to 2020.1 Data source HES APC, 1990–2020.
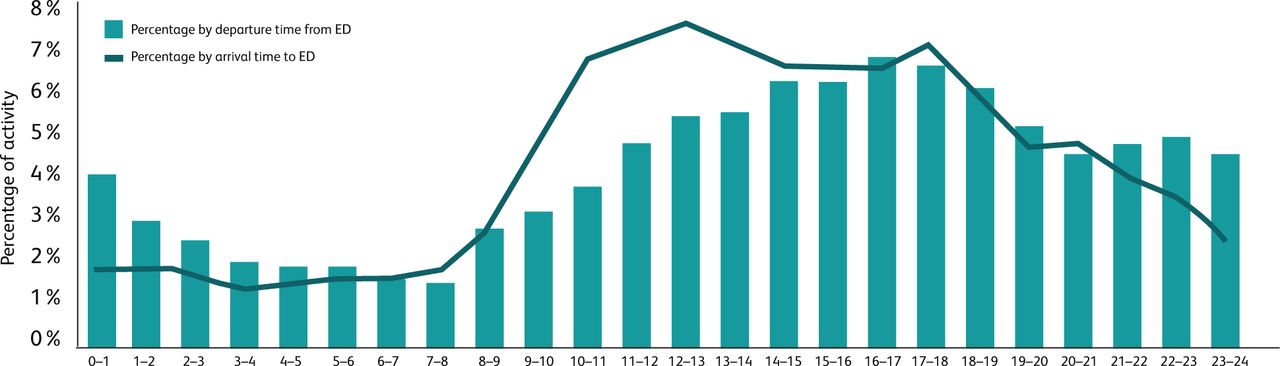
Delays in transitions of care from EDs (Fig 3) have led to more ongoing care being delivered over extended periods in these environments. This causes significant risks and increased mortality as they are not designed to provide this care.26 Delays can be caused by inadequate use of direct admission or SDEC pathways, lack of beds, blocks to discharge, or a mismatch between staffing levels and peaks of activity. If these issues arise then ideally care should be provided by the appropriate speciality team, also facilitating early transfer to the right care environment; however, this requires a redistribution of an often-constrained workforce.
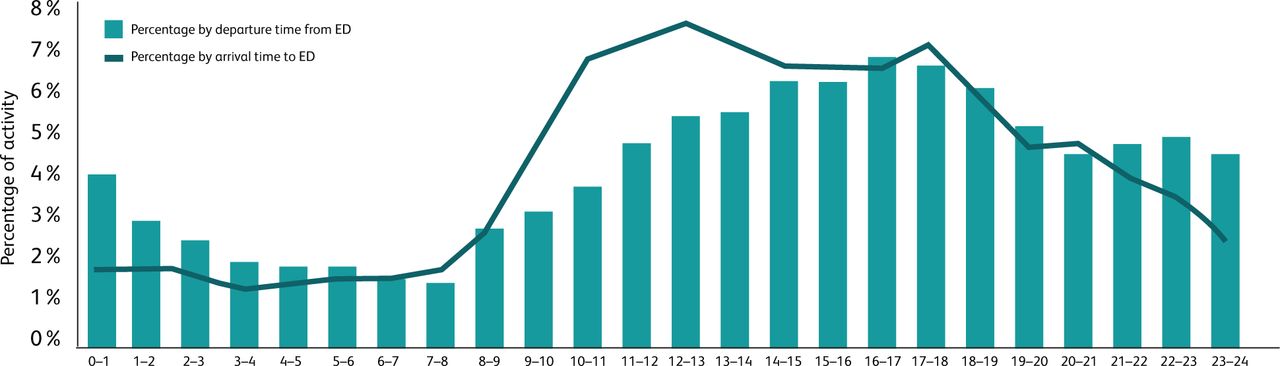
Weekday time of arrival at ED and time of discharge from ED for medical patients aged 16 years and over, for a site where all patients are directed to the ED.1 Data source ECDS, 2019/20.
Acute receiving and diagnostics – the acute medical unit
For patients presenting with acute medical conditions who require hospital assessment and treatment, the vast majority are admitted to acute medical units (AMUs). These usually incorporate bedded inpatient areas, an assessment function to determine the need for admission, and SDEC areas. The ideal AMU should have adequate capacity for patients who do not require transfer to a speciality unit to stay for up to 72 hours, as this continuity reduces length of stay.27 Bypassing acute medical units to general medical or speciality beds can increase length of stay unless they are specifically established for acute receiving and short stay (Table 1).
The AMU should also include an enhanced care area for patients requiring closer monitoring and more complex interventions, as well as areas for procedures (with prepared equipment packs for common procedures), for learning, and for the multi-professional team to come together to handover and plan care. The AMU and SDEC should be part of an emergency and urgent care ‘floor’, with proximity to the ED, radiology, other speciality assessment areas and critical care (Fig 4). This enables working between departments for patients with cross-speciality needs. In smaller hospitals, assessment units may be multi-speciality or even integrated with the ED.6

The acute emergency floor and acute medical unit. AMU = acute medical unit; ASU = acute surgical unit; ED = emergency department; LoS = length of stay; SDEC = same-day emergency care.
The same access times for investigations, often recommended in national guidelines, must apply to all patients in the emergency and urgent care floor. This prevents bottlenecks or the use of ED just for timely diagnostics. Near-patient testing is increasingly being deployed in acute medicine, including point of care ultrasound (POCUS) as part of acute assessment. This provides rapid assessment to clarify diagnoses and can be performed in all care settings.
National evidence-based guidelines for acute medical conditions should be implemented locally. Teaching and ready access to these pathways is required to ensure reliable application. The use of ‘care bundles’ has been applied where a combination of assessments and interventions are required for common and critical conditions. It is important that rationalised decision making is documented within them. One successful example in acute kidney injury has linked laboratory-based identification and education, reducing length of stay and enhancing quality of care.28
The role of AMUs, given that these patients have already been assessed in the community or by ED practitioners, is shown in Box 4.
Role of the acute medical unit
Duplication of previous assessments wastes clinical time and is a poor patient experience. Some patients transferring from EDs may be appropriate for immediate senior review, rather than ‘double clerking’. For many a more detailed assessment is required, building on the previous assessment. Structured record proformas, on paper or in electronic records, can aid this.
Patients who are expected to stay in hospital for longer than 72 hours must transfer from AMUs once stabilised without delay to promote most effective use of AMU and acute medical teams. This responsibility should be shared across specialities.
Same-day emergency care
Many patients presenting with acute medical conditions do not require an admission for inpatient care. Over a number of years, ambulatory acute medical care services have developed in different formats, both for specific conditions and for particular presentations, eg chest pain. Evidence-based risk stratification and scoring systems have been used to help identify these patients.29 Same-day emergency care (SDEC) is now being embraced from a policy perspective by the NHS in England; accordingly, SDEC units are rapidly expanding and can assess and treat most patients who do not need to remain in hospital overnight. Key aspects of successful SDEC units are shown in Box 5.
Key attributes of successful same-day emergency care units
The AMU, inclusive of SDEC, should be the ‘hub’ of acute medicine, being a triage point for acute medicine telephone referrals and enabling rapid follow-up after hospital admissions, day case acute treatments, and monitoring of patients remotely following initial assessment. Considering patient appropriateness to receive care ‘ambulatory first’ can reduce acute medical bed requirements.30 Receiving directly to SDEC from NHS 111 or ambulance services has been tested in a number of units. Senior clinicians receiving referrals or advice calls from GPs and EDs can reduce admissions (Table 1).31
Medical specialties can provide ‘hot clinic’ slots, ideally within their own outpatients clinic, but spread through the week; if space is not available the SDEC units can be used (Table 1). The GIRFT gastroenterology report gives the example of the opportunities available for day case acute paracentesis, with rates varying from 1% to 67%.14
The SDEC benchmarking report of 2021 showed that 64% of hospitals in the UK had a SDEC unit open for at least 12 hours a day 7 days a week,32 meaning that units are most likely to be open during the day but not necessarily when hospital attendances peak between 5pm and midnight.
Acute frailty services
Many hospitals in the NHS have now developed acute frailty services in response to the NHS England Long Term Plan for seven-day provision of comprehensive geriatric assessment in acute settings.33 There are many models, but the aim is for rapid assessment and discharge of patients with frailty who present with acute deterioration. Different models include dedicated units, cohorted areas of acute medical units, assessment with EDs, and community-based units with direct access from ambulances and community practitioners. However, audit of acute frailty service provision shows there are substantial gaps between potential demand and availability of local services.34
Hospital at home
Hospital at Home is a service that provides acute, hospital-level care by healthcare professionals in a home context for a condition that would otherwise require acute hospital inpatient care.35 Key features are shown in Box 6.
Key features of ‘hospital at home’35
Point-of-care blood testing, along with POCUS, has increased the possibilities of acute medical care in the patient's home, reducing the need to attend hospital primarily for investigation.36 Although a wide range of acute medical conditions can be diagnosed and treated in the home,37 this is not currently a widely developed or deployed model of care in the UK.38 Physician-led acute ‘hospital at home’ care models show improved clinical outcomes for older adults with frailty when compared with in-patient admission, in particular reduced incidence of delirium and progression to institutional care.38 For the NHS an average of over €2,000 per patient treated can be saved in this model.39,40 Their development is a dominant feature of acute care policy in the UK.41,42 Clarity in what is encompassed in ‘hospital at home’ or ‘virtual wards’ is required. Continuing evaluation of emergent models will be essential43 and training will need to be incorporated into current programmes.
Multidisciplinary (multispeciality) care of acute episodes
Acute medical care, although led by acute physicians, should be multiprofessional and appropriate levels of multidisciplinary staffing to meet demand is essential over 7 days.
Many AMU and SDEC teams include advanced care practitioners and physician associates, who are a valuable part of the workforce, providing acute medical assessment and treatment monitoring under the supervision of a senior decision maker.
Pharmacists provide a crucial role in acute medical care. Adverse effects of medication account for 6.5% of hospital admissions, most of which will present as unselected acute medical problems.44 Furthermore, half of all patients have a medication error and 20% have a medicine-related adverse event on or immediately after hospital discharge.45 Patients with multiple conditions have polypharmacy. When prescribing new medicines, reminders of possible interactions are needed and deprescribing may be pertinent.
Allied health professionals such as physiotherapists and occupational therapists provide important assessments of function, and treatment for many patients particularly those who are frail. Nursing staff provide essential bedside care and monitoring and will get to know patients and families well, often being the most important source of information and communication. Nurse staffing levels on AMUs need to be appropriate to the intensity of care provided, bearing in mind the faster turnover of patients.
The RCP and Royal College of Nursing guidance on Modern Ward Rounds emphasises the multidisciplinary nature of these that is essential for effective care.46 Integrated board rounds, ward rounds, handovers and other activities are essential. Patient and family involvement in care decisions is also critical. Multiple examples are given of excellent practice in team working and patient involvement. Structuring ward activities to ensure certain reviews are prioritised and care plans well communicated is fundamental. (Guidance diagrams from the reports are provided as supplementary material S1 and S2.)
While acute medical teams are competent to provide care for the majority of patients with acute medical conditions, joint work with specialities for certain patients during the first few days of admission will be needed to ensure the best possible care is provided. For high-volume acute specialties and conditions, such as cardiology, respiratory, geriatrics, gastroenterology and diabetes, ‘in-reach’ to AMUs, advising acute medicine teams on individual patient management, should be a routine commitment each day. For lower-volume acute specialties and conditions, daily availability should be planned. Where geography prevents this from happening physically, remote access may be appropriate. This requires clear planning as part of a speciality team's commitment (see Table 1). Specialist nurses will provide important care in acute medical units, including in diabetes, respiratory, oncology and palliative care.
Clear pathways for common presentations that may not be speciality-specific have developed in several areas, for example blackout clinics.12,47 These can be protocol-driven and nurse-led. Also, some specialities that have previously largely involved outpatient services are developing models of acute care that will link with acute medical units. The future of acute neurology services is described in the GIRFT neurology report, with models for different sized units.12 Patients with neurological presentation comprise 10% of acute admissions (Table 1).
For certain conditions, to ensure access to specialities 7 days a week, services need to be provided across a number of hospitals, particularly for smaller hospitals and in rural areas. A networked arrangement is important to ensure consistency of access for all patients.48 Clear examples are in cardiology and stroke, but the approach can be applicable in other specialities.
If AMUs are ‘right sized’, approximately 40% of acute medical admissions will be transferred to general medical and speciality wards. However, only 20% of these patients may have a pure ‘speciality need’. Referring wisely,49 published by the Royal College of Physicians clarifies which conditions should have direct speciality care. Hospitals should use bed modelling to determine the best size and distribution of speciality beds. However, the majority of inpatients beyond acute medical units will have general medical or multisystem needs, often with associated frailty.33 The general medical skills of all physicians therefore remain paramount, including the ability to assess and manage frailty and its complications, often including delirium and deconditioning. This will include using the Clinical Frailty Scale, 4AT score, and delirium assessment tools.
Preventing readmission and end of life care
When a patient has recovered from an acute medical condition, prevention of readmission to hospital must be a key element of their care. For some patients with relapsing conditions, readmission may not be fully preventable; however, key factors and interventions that reduce the risk of readmission include:
contact with a healthcare professional at 48–72 hours following discharge to check the patient's condition and ensure follow up arrangements
medication review and reconciliation at home
a way to contact a healthcare professional should their condition change
clear transfer of care plans for ongoing coordination of the patient's care, particularly if they have long-term conditions or frailty
advance care planning, clarifying the interventions the patient and practitioners agree are appropriate should they deteriorate. This is particularly important for patients who may be in their last year of life.
In the last few weeks and days of life, facilitating rapid transfer to home requires close coordination with palliative care teams and primary care. While this is NHS policy, it is only achieved for less than 30% of patients.50 Having a system-wide approach to advance care planning and education, and transfer of information focused on care homes for the elderly, reduces hospitalisation and length of stay.51
In England and Wales a discharge medicines review service has been established, whereby a community pharmacist supports the patient with their medicines immediately following discharge, ensuring medication reconciliation and supporting self-management. This has been shown to reduce readmissions.52
In single-organ conditions, follow-up following acute hospital care is commonly in place and the use of the wider clinical team is key. For frail older people, seamless transition from hospital to home is essential. For patients with less well differentiated needs there can be gaps in follow up to ensure recovery or next steps of investigation and management. Development and evaluation of service models is urgently required.
Conclusion
The NHS is not currently coping with acute medical care, and demand and complexity will continue to increase for the foreseeable future. While models of acute care are continually developing and adapting many of the basic proven elements of care are commonly lacking, and their consistent implementation constrained by a focus on new initiatives that require adaptation and evaluation. We urge local healthcare systems to focus on the fundamentals first (Box 1), and then test and evaluate potential futures (Box 2). We urge all local medical specialities to play their part in delivering acute medical care.
The biggest constraints to ‘getting the basics right’ are workforce, physical estate, up-to-date IT, and local data systems for accurate planning and analysis. There is very significant variation across the NHS in how acute medical services are provided, despite national guidance from the NHS and professional bodies. Where excellent services are developed, strong clinical leadership and managerial partnership is observed.
Variation is expected and appropriate because of local needs. However, when services are underdeveloped, then building a critical impetus for development rather than just keeping ‘afloat’ is difficult. Working across wider geographies, with extra support from NHS and professional bodies, will be needed.
Even if the fundamentals are in place and potential developments reap rewards, it remains unclear whether these will meet acute medical demands to the expectation of patients and professionals. Overarchingly we need strong and consistent data for local evaluation and feedback, as well as spreading effective practices, this will drive continuous improvement and enable modelling against the changing and growing demand.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj:
S1 – Ward round fundamentals.
S2 – An effective ward round.
- © Royal College of Physicians 2022. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- Introduction
- Care outside the hospital
- Initial assessment
- Acute receiving and diagnostics – the acute medical unit
- Same-day emergency care
- Acute frailty services
- Hospital at home
- Multidisciplinary (multispeciality) care of acute episodes
- Preventing readmission and end of life care
- Conclusion
- Supplementary material
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.