
ABSTRACT
Diagnostic capacity in the NHS in England was much lower than that in many other developed countries before the COVID-19 pandemic. The relative lack of diagnostic equipment and workforce is now hampering recovery from the pandemic. In response to this, a major programme of work is now underway to improve access to a wide range of diagnostic tests. Establishment of community diagnostic centres is a key component of this programme.
Introduction
Despite the importance of diagnostic tests in the diagnosis and monitoring of a very wide range of health conditions, the NHS in England has not until recently had a formal diagnostics strategy. However, during the development of The NHS Long Term Plan (2019), it became apparent that many of the commitments on specific conditions (such as cancer, heart disease, respiratory diseases, stroke and musculoskeletal conditions) would not be achieved without a major drive on diagnostics.1
In response to this, an independent review of diagnostic services was commissioned by NHS England in 2019. The scope was deliberately broad, encompassing imaging, endoscopy, physiological measurements/sciences and pathology. A genomics strategy had already been developed, so was not considered in detail, except where it overlaps with other diagnostic disciplines.
Work on the independent review was well under way before the first wave of COVID-19 and the need for radical improvement was already clear-cut. However, the pandemic has further highlighted the urgency of making major improvements in diagnostic services. The independent report, Diagnostics: Recovery and Renewal (also known as the Richards' review) was published in October 2020 and the recommendations were unanimously supported by the board of NHS England.2
Diagnostics: Recovery and Renewal: key findings
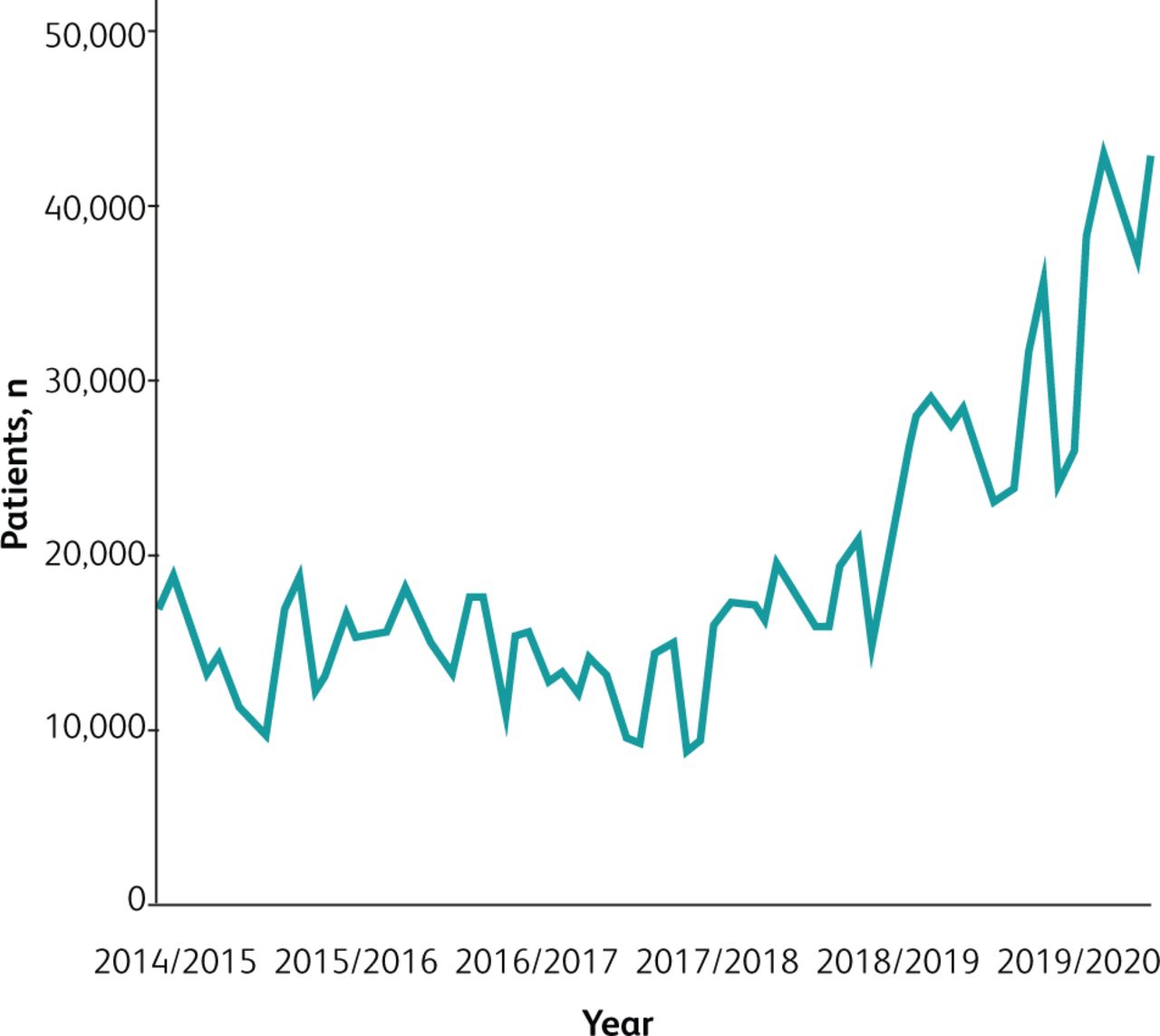
Demand for almost all diagnostic procedures had been increasing markedly in the 5 years before the pandemic, with increases of around 4%–5% per annum for endoscopy, ultrasound and dual-energy X-ray absorptiometry (DEXA) and considerably higher rates (7% or higher) for computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET) – CT. These increases were higher than those for other aspects of activity within the NHS, such as emergency department (ED) and outpatient attendances or emergency admissions. However, diagnostic capacity had not kept pace with demand. As a result, diagnostic services were reaching a tipping point. This was shown by the marked increase in breaches of the 6-week diagnostic standard in the 2 years before the pandemic (Fig 1) and by major increases in outsourcing of imaging, endoscopy and pathology.3 Reliable national data were unavailable for some aspects of diagnostics, including histopathology and physiological sciences, but evidence from individual trusts demonstrated the very substantial pressures experienced in these services. Cancer performance and, in particular, the 62-day standard had been deteriorating well before the pandemic, often reflecting delays in getting diagnostic tests and results.

Patients waiting over 6 weeks for a diagnostic test (pre-pandemic).
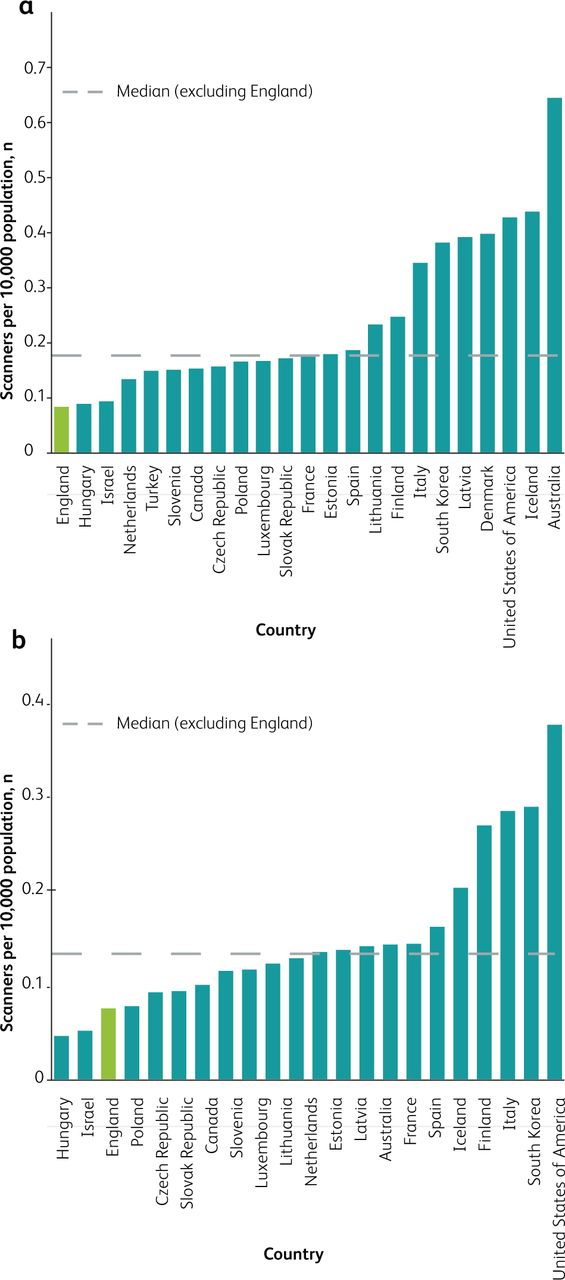
International comparisons are available for CT scanners (Fig 2a), MRI scanners (Fig 2b) and PET-CT scanners per 10,000 population. In each case, England is at or close to the bottom of the international league table. Figures for scans per million population are marginally better than this, showing that our low asset base is used better than in some other countries. CT scanner numbers would need to double just to reach the Organisation for Economic Co-operation and Development median.

Scanners per 10,000 population (2017). a) Computed tomography scanners. b) Magnetic resonance imaging scanners. Data from the Organisation for Economic Co-operation and Development diagnostic exams and population data (2017), NHS England imaging data collection (2017/2018) and Office for National Statistics population data (2017).
In addition to the increases in activity needed to deal with backlogs arising from the pandemic, demand is almost certain to continue to rise over the next 5 years due to wider indications for these technologies. Around one in 10 patients attending a type 1 emergency department now receive CT. The number of urgent referrals for cancer continues to rise, after a fall at the start of the pandemic. These referrals generate a wide range of diagnostic tests including upper and lower gastrointestinal endoscopies, MRI (eg for possible prostate or brain cancers) and CT. Following diagnosis, more patients with cancer are receiving systemic therapies, which in turn lead to more scanning to monitor response. Even larger increases in activity will be needed should lung cancer screening using low-dose CT be recommended. The use of CT angiography for heart disease is also set to increase markedly. Overall, the Richards' review anticipated growth in demand of around 100% for CT over the next 5 years. Commensurate increases both in equipment and workforce will be needed to meet the demand.
The findings and recommendations in the Richards' review leant heavily on those emerging from various Getting It Right First Time (GIRFT) reports relating to diagnostics. Those relating to radiology are summarised in Box 1.
A 10-point plan for NHS imaging services: recommendations from the Getting It Right First Time radiology programme
Diagnostics: Recovery and Renewal: key recommendations
The Richards' review made a total of 24 recommendations. Key elements are summarised in seven points here.
Diagnostic equipment and facilities should be expanded and upgraded as soon as possible. High-quality data on imaging facilities already existed on which estimates of numbers of machines could be made. For other diagnostic modalities (eg endoscopy and physiological sciences) where national data are not available, baseline surveys should be undertaken.
The diagnostic workforce should be expanded substantially across all modalities, with new roles being developed and training academies being established.
New service delivery models with new pathways to diagnosis should be established. These should separate emergency/acute and elective diagnostics, wherever possible, to improve efficiency and reduce delays for patients. Community diagnostic hubs (now called community diagnostic centres (CDCs)) should be rapidly established.
Improving connectivity and digitisation should be prioritised across all aspects of diagnostics.
Innovative approaches to diagnostics should be evaluated as quickly as possible and then implemented across the NHS. These are likely to include the use of artificial intelligence (AI) to assist human reporting in imaging, pathology and endoscopy. The use of new diagnostic technologies that can be used in patients' homes should be expanded, building on learning from home testing for COVID-19.
Clinical and managerial leadership should be put in place for all diagnostic disciplines at national, regional and local/system/network levels.
Standardised data should be collected across all diagnostic modalities to drive operational performance, support business planning and to inform service improvement.
Acute and elective diagnostics
The large majority of diagnostic services have traditionally been provided in acute hospital settings in this country. However, separation of ‘acute’ diagnostics (those required by the ED or for inpatients) from ‘elective’ diagnostics (those requested by a general practitioner (GP) and those requested as an outpatient by a specialist) will improve efficiency of throughput for both sectors. Before the pandemic, growth in CT in the acute sector (9% per annum) was somewhat higher than in the elective sector (6% per annum). A similar picture was seen for MRI done for emergency indications, though the overall number of MRI done in the acute sector is much smaller. Endoscopy is largely an elective procedure, though an important minority of cases are done as an emergency.
Demand for non-elective imaging (particularly CT) has continued to grow in recent months. Diverting some of the elective demand to CDCs should relieve the strain on acute hospital services. This is much needed to enable stroke patients to be scanned within an hour and inpatients to be scanned on the day of request, thereby facilitating earlier discharge for some patients.
The uses of both acute and elective diagnostics in one specialist area (respiratory diagnostics) are shown in Box 2.
Respiratory diagnostics: a vignette
Community diagnostic centres
Although the establishment of CDCs may appear quite radical in this country, most other countries undertake a very significant proportion of their diagnostic work outside of acute hospitals. Six overarching aims lie behind the recommendation to establish CDCs in this country (Box 3).
Key aims for community diagnostic centres
It is also anticipated that CDCs will contribute to improve staff satisfaction, making every contact count, research and innovation, and net zero carbon emissions. They should also act as anchor institutions for the populations they serve.
Three archetypes of CDC have been defined. A standard CDC will deliver a minimum range of tests including imaging (CT, MRI, ultrasound and plain X-ray), physiological measurements (including spirometry, fractional exhaled nitric oxide (FeNO), electrocardiography (ECG) and Holter monitoring, blood pressure measurement, echocardiography, and some sleep studies), phlebotomy and some point-of-care tests. A large CDC will provide all of these services and any other diagnostics required locally; examples include endoscopy, mammography and ophthalmology. A ‘hub and spoke’ model is the third archetype, with services radiating out from a standard or large CDC to bring diagnostics closer to patients.
One of the main aims of CDCs in the short to medium term is to contribute to elective recovery following the pandemic and to assist in the recovery of cancer performance standards, which have been hit hard by the pandemic.
Significant capital and revenue funding was provided in 2021/2022 to get this programme underway, with over 80 sites being established (or expanded if they were already providing some community diagnostics) by end of March 2022. Over 800,000 additional diagnostic tests were provided in 2021/2022 through this programme, with activity set to increase markedly over the coming years.
Further capital (₤2.3 billion) and revenue funding has now been secured to take the overall diagnostics programme forward over the next 3 years. Integrated care systems (ICSs) are now being asked to develop their plans accordingly.
Securing additional workforce is well recognised as being the greatest challenge to the programme. Several actions are being taken at a national level through Health Education England and NHS England and at local levels to secure the workforce needed. These include provision of additional training places for diagnostic specialties, establishment of diagnostic training academies and international recruitment. New workforce models are also being tested with additional support workers and apprenticeships freeing up qualified staff to work at the top of their licences. Efforts are also needed to promote retention of existing staff.
Clinical pathways involving CDCs
Much of the attention to date has been on getting facilities up and running, and on undertaking additional activity, diverting some requests for diagnostics from acute hospitals to CDCs.
However, it is also recognised that several of the key benefits of CDCs will not be realised unless clinical pathways are also changed. Work is now underway involving national clinical directors and national specialist advisers to define pathways that are particular priorities for development and testing.
One pathway that could well utilise CDC facilities is at an advanced stage of development. This relates to the diagnosis of patients with chronic breathlessness. Breathlessness accounts for around 4% of primary care consultations, with late diagnosis and wrong diagnosis being frequently observed. It can be difficult for GPs to know whether the patient has heart failure or a respiratory problem, and thus which specialist service a patient should be referred to.
A range of ‘cancer-related’ pathways could also be channelled through a CDC in the first instance. These could include lower gastrointestinal, prostate/urological, lung, gynaecological and skin pathways. Telephone triage developed during the pandemic could be used to direct appropriate patients straight to tests, many of which could be undertaken in a CDC, especially if consulting/clinic rooms are made available. Some patients referred urgently with lower gastrointestinal symptoms could be triaged to CT colonography (CTC) or colon capsule endoscopy (CCE) based on risk determined by faecal immunochemical tests (FIT) levels. Those at highest risk would still require colonoscopy, but this approach should release more capacity to extend the bowel screening programme. Technologies such as dermoscopy could be undertaken in a CDC by non-medical staff, reducing pressure on hospital dermatology services.
Looking forwards
CDCs are only one step in a journey towards high-quality diagnostic services in this country. A major programme to promote IT connectivity and digitisation is underway. This is vital to avoid duplication of workloads, to share workloads across institutions and to promote home reporting. Digitisation will also underpin the validation and subsequent use of artificial intelligence to support diagnostics.
Nor should the decentralisation of diagnostics stop at CDCs. Provision of diagnostics at home is now becoming increasingly feasible with point-of-care ultrasound, portable X-ray machines and a range of point-of-care blood and urine tests. Work is now underway at NHS England to develop a Diagnostics@Home programme to capitalise on these and other new technologies. Home testing by patients has become commonplace through the pandemic. We should build on this for health promotion and screening interventions, earlier diagnosis of symptoms and, thus, better outcomes for patients.
Conclusion
Diagnostic services are now recognised as being a very high priority by the government and NHS England. Very significant levels of funding have been committed and good progress has been made to implement the recommendations of the Richards' review with, in particular, the establishment of CDCs. However, major challenges persist relating to backlogs in diagnostics arising from the pandemic on top of pre-existing deficiencies in diagnostic capacity. Severe shortages in the diagnostic workforce remain the largest barrier to the provision of high-quality services, but initial steps to remedy this long-standing problem are encouraging.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.