
ABSTRACT
The UK has a long history of attempts to integrate child health services to improve outcomes, an ambition renewed in the recent The NHS Long Term Plan. It's therefore timely to review the history of integration to inform future initiatives. Key milestones include the Platt report (1959), Court report (1976), Sure Start (1999), National service framework (2004) and Facing the future report (2015). These stand against a backdrop of national NHS policy changes, with a myriad of local integration initiatives and research efforts in parallel.
We suggest lessons for future integration initiatives: integration may support the quadruple aim; integration depends on addressing divides between primary and secondary care; workforce and funding challenges need to be resolved before integration can thrive; high-quality research and evaluation of integrated interventions is required; strong relationships between professional groups are key to integration; and integration can help address health inequalities.
Introduction
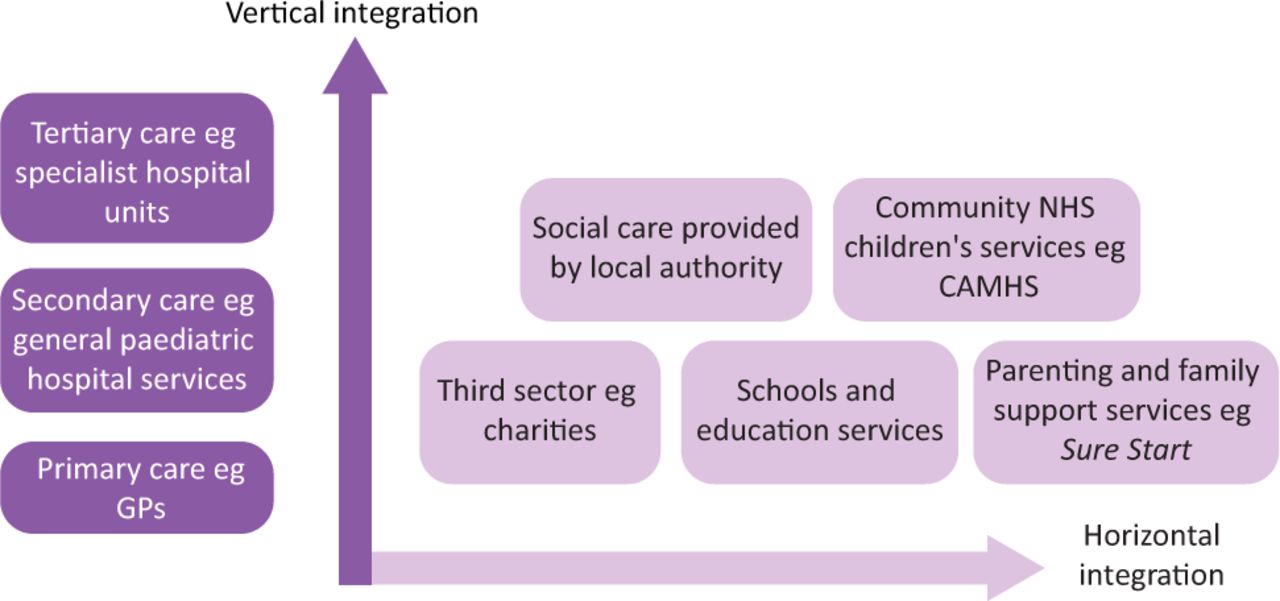
The UK has relatively poor child health outcomes compared with other high-income countries, and integration of health services for children and young people (CYP) has been proposed as part of the solution.1,2 Vertical integration occurs when providers in the same sector but at different levels, such as primary and secondary healthcare, jointly deliver services.3 Horizontal integration happens when providers in different sectors but at the same level work closely together, such as community NHS and social care services (Fig 1).3 The healthcare landscape for CYP in England is complex, but key providers include the general practice multidisciplinary team in primary care; hospital-based paediatricians and associated professionals in secondary care; and community paediatricians based outside the hospital, who work with colleagues to provide specialised care for children with issues such as disabilities and complex health needs. There is a long history of efforts to integrate child health services in England (Fig 2), and the NHS recently articulated a renewed desire for this.4 It is therefore timely to review the history of integrated care and draw lessons to inform future initiatives.
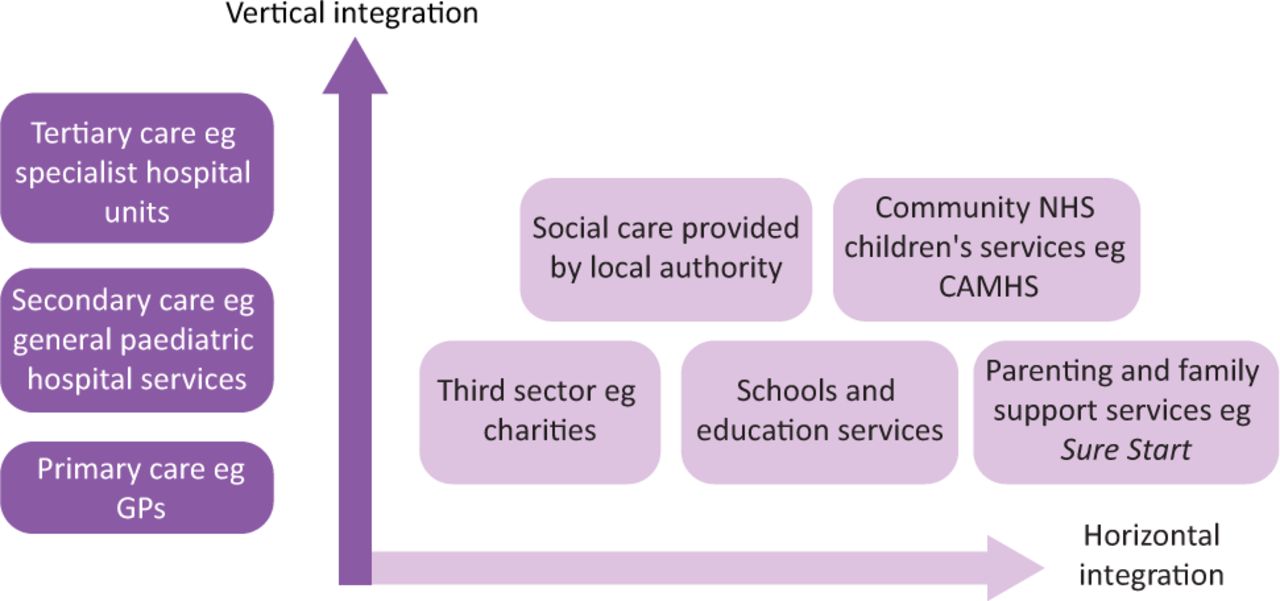
Vertical and horizontal paediatric integration. CAMHS = Child and Adolescent Mental Health Services.

Timeline of milestones in paediatric integration. CYP = children and young people.
Tracing the history of integrated child health services
The 1946 National Health Service Act established a tripartite system, with three parts managed separately: hospitals; primary care providers, such as general practitioners (GPs); and local authorities providing services including immunisations and maternity care.5,6 This led to a void of communication between hospital and community services, resulting in pressure to unify the structure catalysed by the belief that community-based care could be cheaper in the face of escalating costs.7–9 In parallel, the 1959 Platt report into children's healthcare advocated for improved communication between paediatricians and GPs and was supportive of services caring for sick children at home.10 Following this, the 1962 Porritt report recommended unifying services under local ‘Area Health Boards’.11 This created momentum culminating in the 1973 NHS Reorganisation Act, which integrated the tripartite structures into unitary regional health authorities.12 This was broadly viewed as unsuccessful and responsible for a decline in public health and community services.13 However, it created the opportunity to review child health services, resulting in the 1976 Court report. This recommended the development of an integrated child health service, staffed by community paediatricians and new ‘general practitioner paediatricians’: GPs partly specialising in paediatrics.14 While other recommendations were successful, such as integrating child psychiatry services, the main call for an integrated child health service wasn't delivered. This was due to the cost of reorganising the system and differences within and between professional groups resulting in a lack of consensus about the best approach.14 However, there were concurrent examples of local progress in integration, such as an initiative in Sheffield that reduced hospital visits and was particularly effective in deprived areas.15
Attempts to improve coordination continued with the 1981 Acheson report on primary care in London, requiring hospital reconfiguration to take primary care into account.16 Subsequently, the 1990 GP contract expanded the scope of general practice, creating more fertile ground for the integration of child health services. The 1990 National Health Service and Community Care Act was the next wholesale reorganisation, introducing the internal market and purchaser-provider split, with the establishment of GP fundholders offering the chance to create more unified hospital and community paediatric services.14,17 However, this did not materialise as the legislation's competitive philosophy encouraged community providers to become separate trusts, fearing asset-stripping if merged with hospitals.18 This led to ‘unseemly rivalry between trusts who should be cooperating’.14
The Health Act 1999 heralded a shift from competition to collaboration.19 The act also supported horizontal integration between the NHS and social care through pooled budgets and joint delivery of services. Horizontal integration gained further momentum with Sure Start, which combined ‘education and care for the under-fives’ in deprived areas by providing services across schools, local authorities and voluntary groups.20 The initiative was supported by the 1998 Acheson Independent inquiry into inequalities in health, highlighting how child health was shaped by socioeconomic factors.21
In 2004, the Department of Health published the first national standards for children's care, the National service framework (NSF).22 The NSF aimed to change NHS culture to recognise that children have unique needs requiring bespoke services.23 Integration was part of this, with a commitment to ‘high quality services which are co-ordinated around [the individual]’.22 The subsequent development of children's trusts by local authorities offered a path to this by aiming to integrate local health, social care and education services.24 Two-thirds of trusts achieved integration by pooling budgets at least partially.24
In 2007, Lord Darzi's report, Healthcare for London: A framework for action, was published emphasising that patients should be cared for as close to home if possible, reflecting later research that children and families supported this.25,26 The government's 2012 Health and Social Care Act introduced strategic clinical networks working across commissioners, providers and voluntary organisations, but also concerns about service fragmentation due to market liberalisation and commissioning changes.27,28 2014 saw the introduction of personal health budgets, giving CYP with complex needs more choice about how to use funding to support their health and wellbeing.29 The initiative also contained a duty for clinical commissioning groups and local authorities to work together to develop services for children with special educational needs or disability, thus facilitating horizontal integration.30 The Five year forward view, a landmark NHS strategy document also released in 2014, changed the tone to focus on integration and collaboration, envisioning more out-of-hospital child healthcare and primary–secondary integration.31 This was reinforced by Facing the future: Together for child health, a report by a coalition of royal colleges in 2015 that included aspirational standards, such as immediate telephone access for GPs to paediatricians, which research has shown can reduce hospital referrals.32,33
Parallel to formal policies, local initiatives and research continued. In north-west London, Connecting Care for Children hubs, where paediatricians run joint clinics with GPs, led to positive outcomes including up to 39% fewer new hospital appointments.34 Similar services were subsequently developed nationally in areas including Birmingham, Leeds and Newcastle.35 In south London, the Children and Young People's Health Partnership (CYPHP) was developed. This is a ‘clinical academic partnership for health system strengthening’ that aims to foster collaboration between organisations across the healthcare system to deliver co-produced, patient-centred care to CYP closer to their homes, as well as delivering health promotion with the aim of preventing illness.36 Early outcomes were promising, suggesting reduced emergency department attendances with accompanying cost savings, and empowerment of families.36 Additionally, a training initiative in north, west and south London placing GP and paediatric registrars in ‘learning together clinics’ improved trainee experience and reduced hospital utilisation.37
The 2019 The NHS Long Term Plan reaffirmed the commitment to vertical and horizontal integration of CYP services.4 This included a new cross-sector model for CYP mental health services, taking inspiration from the i-THRIVE programme. i-THRIVE uses a needs-led approach to provide mental healthcare to CYP and their families, grouping patients into five categories and emphasising shared decision making and prevention.38 Initial qualitative evaluation was generally positive, although it did highlight challenges relating to funding and collaboration between organisations.39 The NHS Long Term Plan also described a desire for greater integration between health services, local authorities and the Department for Education to support children with learning disabilities and autism.4 Most recently, the Integration and innovation white paper proposed new laws to support integration by reducing competition and increasing local autonomy.40
Lessons from the past
There are several lessons from the history of integrated child health services. The first is that integration generally appears to deliver positive outcomes for patients, staff and the wider system, and therefore helps to deliver the quadruple aim of better health outcomes, improved patient experience, improved staff experience and lower costs. Patients and families are satisfied with integrated child health services, with satisfaction stemming from seeing a specialist closer to home, better communication between clinicians, being seen in a familiar environment and improved quality of life.2,15,34,41 Professional satisfaction relates to strengthening relationships between clinicians, increased access to specialist support and mutual education.15,34 System benefits include decreased secondary care utilisation, fewer diagnostic tests and decreased costs, although one meta-analysis of integrated care for CYP did not find a reduction in emergency department visits specifically.2,15,34,37,42 These benefits are generally echoed by the literature on integrated care for adults, except for costs that are increased.37,43,44,45 However, it should be noted that integrated child health research is not always of high quality, and so we cannot be more than tentatively certain of these conclusions. We discuss this issue in more detail later.
The second lesson is that the ongoing organisational and cultural divide between primary and secondary care impedes integration. The organisational divide was illustrated by failed integration attempts following the 1990 purchaser–provider split because purchasers, often GP fundholders, feared that community services would be diminished if integrated with hospitals.18 The cultural divide was exemplified by GP resistance to Court's proposal for GP paediatricians (GPPs) due to concerns that it might dilute their commitment to generalist care of the whole family.14 Moreover, some paediatricians have reported reservations about community working, due to loss of ‘prestige’ of being in a hospital, as well as more practical misgivings about a ‘lack of specialist equipment and facilities’ in the community and the risk involved with community care.26,46 In contrast, others preferred the ‘more peaceful’ environment of community clinics.26
The third is about the human and financial resources needed to initiate and sustain integrated services. Such services are often driven by individual champions, but their sustainability is vulnerable to wider factors, such as funding and workforce pressures.26 For example, a 2017 audit of the Facing the future report recommendations found that, during peak hours, there weren't enough consultant paediatricians for hospital services, let alone community integration, and 80% of GP telephone hotlines were unfunded.47 Meaningful integration is likely to remain aspirational until structural organisational and financial issues are addressed.48
Fourth, a consistent, long-term approach to research and evaluation of integrated interventions is needed to support improvement and enhance credibility. Current evidence is largely supportive but is primarily observational, small scale and of variable quality, limiting reliability.2 Researching integrated care is challenging due to the heterogeneity of interventions and outcomes, and the multitude of confounding factors. The use of logic models and robust theoretical frameworks can partially mitigate this, but isn't common.2 However, well-designed studies using robust methods, such as cluster randomised controlled trial and systematic review, are currently underway and should provide more definitive evidence.49,50 A planned process evaluation to accompany one of these studies may also offer valuable insights for future interventions about the practical implementation of integrated care for CYP.51
The fifth lesson is that effective integration depends on strong relationships and trust between professional groups.15,46 For example, case studies of integration of community children's nurses with urgent care found that success was predicated on trust between professionals.52 Strong professional relationships encompass both formal interactions and informal contact, such as ad hoc communication via telephone or email, with both supporting integration.15 Nurturing relationships requires collaborative service models that draw on the respective strengths of hospital and community care, not ‘drag and drop’ replicas of hospital clinics in the community.26
Finally, integration may be particularly effective in deprived areas by enhancing access for underserved populations, primarily through outreach clinics that bring paediatricians closer to deprived communities, reducing travel time and cost for patients.15,42 This finding is also supported by research in adult integrated care.43,44 In an era of widening health inequalities where the ‘inverse care law’ still rings true, integration may be a powerful tool to address the gap.53,54 However, this requires a deliberate focus on integration of services in deprived areas, and not just of high-performing services that are early adopters, regardless of location.
The future of integrated child health services
These lessons are pertinent during this time of rapid evolution for the NHS, driven by internal factors (such as policy shifts towards integration) and external factors (such as COVID-19).
In terms of the organisational divide between primary and secondary care, the NHS is attempting to address adversarial contracting relationships by making providers financially co-dependent within integrated care systems.55 Primary care networks, another recent innovation that groups practices together to care for 30,000–50,000 patients, may have the scale to make a role analogous to Court's GPPs feasible.56 This could be delivered via the Royal College of General Practitioners' recent ‘general practitioner with extended role’ framework.57
Workforce challenges in paediatrics and general practice remain deep seated.58,59 Increasing digitisation, catalysed by the COVID-19 pandemic, may provide a partial solution by making participation for professionals in integrated services more efficient by eliminating travel time. Technology may also facilitate more interaction between primary and secondary care, avoiding the scenario of integrated care simply being ‘drag and drop’ of existing secondary care clinics. For example, technology may allow delivery of virtual clinics; rapid collaboration between professionals via email, phone or the e-referral system; easy participation in virtual multidisciplinary team meetings; and collaborative case finding via population level data streams such as the Whole Systems Integrated Care (WSIC) platform in north-west London.60 However, efficiency gains from technology will be incremental, and no substitute for addressing the systemic workforce shortages described earlier.
More broadly, integrated care is key to ensuring that CYP services are responsive to the needs of modern children. In the post-war period, efforts in child health focused largely on community prevention (such as undernutrition, dentistry and immunisation) or acute illness (such as infection or trauma). However, as environmental factors have evolved and medical advances have delivered longer lifespans for children with complex illnesses, the system now needs to respond to the needs of children with long-term conditions such as mental illness, obesity and chronic disease. This demands a vertically and horizontally integrated response. Concurrently, there is regression or stagnation in important areas relating to the social determinants of health, such as immunisation rates and dental health.61,62 There is increasing belief that it is no longer sufficient to simply highlight and attempt to mitigate these causes, but that the system needs to holistically address the social determinants. The social paediatrics approach, where the child is viewed within their social context and collaboration facilitates care, has much to offer.63 Embedding this philosophy within an integrated system that uses population-level data streams shared between providers may be an important approach to addressing the aforesaid challenges.63
Conclusion
Integrated care for CYP in England has progressed in fits and starts over the last 70 years. Although improvements have been made, the picture is of oscillation between periods of advancement and stagnation, illustrated by Spencer's 1993 quote ‘integration is on everybody's lips’ that sounds eerily familiar decades later.15 Recent policy shifts have created fertile ground for integration, but fully capitalising on this opportunity will require us to draw on the lessons of history to ensure that we make the most of scarce resources to deliver better healthcare for our children.
Funding
Edward J Maile is supported by an National Institute for Health Research (NIHR) academic clinical fellowship. Dougal H Hargreaves and Mitch Blair are supported by the north-west London NIHR Applied Research Collaboration (ARC). Dougal H Hargreaves is also supported by the NIHR through the National School for Public Health Research Programme. Georgia Black is supported by The Health Foundation's grant to the University of Cambridge for The Healthcare Improvement Studies Institute.
- © Royal College of Physicians 2022 All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.