
ABSTRACT
As internet of things (IoT) technologies are increasingly adopted by healthcare and hospitals, new opportunities are emerging to transform patient pathways and achieve efficient delivery of care. This implemented project follows the drivers and requirements of industry 4.0, based on surgical process analysis and optimisation using IoT technology, with the goal of creating ‘4.0 hospitals’.
Our study presents the implementation of a novel IoT application, aiming to give support to multidisciplinary surgical teams through the optimisation of patient pathways to facilitate the surgical process. The implemented solution is based on real-time location systems (RTLS) technology, a subgroup within IoT, and it originated through the hospital needing to address the sudden surge of surgical elective care demand. The solution also enhances patient safety, facilitates quality of care by increasing communication and reduces costs. This IoT tool has facilitated the increase of theatre utilisation from 70.02% to 82.5% in 2 years, which has translated into an increase of surgical activity capacity, with an impact on reducing the waiting list.
Introduction
Healthcare systems have started to take a pathway approach to standardise process times and to manage referral-to-treatment (RTT) services. One benefit is to help organisations control patient care on a pathway basis and to remove ‘hidden’ waits.1 In this context, in 2016, Vall d'Hebron University Hospital opened a new surgical building for general surgery with 19 theatres in two wings, with the latest surgical technology, aiming at improving care and patient journey experience and, in turn, boosting surgical capacity.2 To facilitate the standardisation of the surgical process and the automation of patient pathways, the hospital decided to introduce an innovative, real-time location systems (RTLS) technology to streamline patient flow data collection.
This article presents the new technological intervention implemented in the general surgery block and the surgical key performance indicator results obtained after several years of observation.
Background
Over the last decade, RTLS solutions have emerged in the healthcare sector, generating expectations for potential improvements in several areas of the hospital.3 After an initial hype in 2010, with passive radio-frequency identification (RFID) solutions dominating this domain, the first active solutions took off, implementing use-cases of asset tracking, usually to locate expensive medical equipment in large areas. The difference between active and passive solutions is having to exert a manual action, or not, to obtain the data; for instance, passive RFID tags need to be manually read, which limits automation possibilities, innovation and data quality.4 Active solutions relying on Bluetooth, Wi-Fi, ultrasound and other wireless technologies are able to automatically collect the information without needing an operator to execute the action, thus relieving staff from the tiresome task of manual data entry, boosting automation. As technology prices have increasingly dropped over the years, RTLS active technologies have become more viable, which has enabled an explosion of potential, new, automated applications with an increase of usability, adherence and data quality.
At a different level, the main reported benefits of these systems in clinical settings are:
patient flow improvement by identifying and correcting bottlenecks, time wasting and errors in the process5
operational costs reduction by improving time collection, planning and staff coordination6
usability improvement by eliminating manual input of data in other IT systems and phone calls, and offering updated real-time information in the same way airports do with passenger arrivals and departures; this, in turn, is directly linked to staff and citizen satisfaction by improving the usability and way of working for staff and transparency to families during clinical interventions7
patient safety improvement by providing systematic electronic means, eg checking that the right patient is in the right operating theatre to prevent catastrophic events such as receiving the wrong treatment due to human error; RTLS is also used to detect patient falls in other applications8
energy efficiency increase by using the automation generated by these systems to save energy spending in high consuming areas, an important challenge in healthcare.9
Other potential uses of RTLS within the hospital include asset management, hand hygiene control, improvement of patient flow in the emergency department and outpatient clinics, and streamlining time sensitive processes such as the stroke code and cardiac arrest among the most relevant. More interestingly, the vast collection of high-quality data enabled by RTLS solutions opens new horizons in the implementation of process mining, simulation and artificial intelligence applications.
The challenge
As part of its value-based healthcare strategy, in 2016, Vall d'Hebron University Hospital identified a hidden waiting list at outpatient surgery level.10 As this backlog was corrected, its release generated a sudden increase of surgical demand and, in turn, a surge in waiting times, now at a different point in the elective care process. The surgical waiting list started to grow from 8,288 patients in 2015 to 10,459 in 2016 and 11,695 in 2017, compromising legally binding RTT times for patients. For this reason, the hospital had to find ways of increasing its surgical capacity to control the growth of the waiting list and comply with maximum waiting times for patients' operations. Therefore, the hospital decided to support process standardisation and the provision of collaborative tools to streamline patient flows, identify bottlenecks and enable continuous improvement to drive surgical block performance from 70.12% at the time to the optimal target of 85%.11 Furthermore, reducing the stress of relatives and professionals was part of the new strategy with improved communications. To do all that, the hospital took the innovative approach of implementing a RTLS approach, which would provide accurate data to support the constant improvement and real-time communication between all the stakeholders, including families.
Methods
Main objective
The main objective of this work has been to assess the progress of the surgical block key performance indicators between 2017 (roll-out) and 2019. 2020 was not included as surgical activity was dramatically affected by COVID-19.
The new intervention
The digital process intervention (Fig 1) was piloted in the new general surgery block with 19 theatres and 20 beds for both patient preparation and the post-anaesthetic care unit (PACU). The following elements were included:
automatic registering of all the steps and timestamps of the surgical process relieving professionals from manual entering of data into their information system, with the aim of improving data quality
a new digital intervention based on tailored apps that leverage the generated live data by the RTLS solution to smooth collaboration and communication between patient-facing staff teams across the surgical process (ie admission, preparation, theatres, recovery, discharge, porters and cleaners), as well as communications with families
aggregation of accurate real times to enable the monitoring of key surgical performance indicators (ie theatre utilisation, late starts, early finishes, downtimes between cases, turnaround times etc).

Concept of surgical pathway automation through real-time location systems solution. RTLS = real-time location systems solution.
The solution, design aspects
The novel digital approach was built in collaboration with MYSPHERA, which developed a bespoke technological solution for the surgical process.
An important design decision taken by the company was to use Bluetooth Low Energy (BLE) instead of other active RTLS. The main reason was to obtain a solution that could solve the real-time location problem for the specific use-case in the hospital cost-effectively, ie patient flow at the surgical setting. While technologies like ultra-wideband (UWB) can provide greater accuracy, the cost is increased by having more expensive hardware and a more complex solution architecture, which might be justified in industrial applications where high precision is needed or for very specific cases in the hospital, resulting in much higher installation and operational costs. The same arguments apply for ultrasound technology. In the case of RFID real-time technology, applications are limited by the need of having a by-hand operation and prices for its hardware also tend to be very expensive. Alternatively, Wi-Fi could have been a good candidate for RTLS in the hospital as it is already implemented in most facilities with its network of access points. The main problem of Wi-Fi is the fact that it has not been designed to enable accurate real-time location solutions but rather to provide internet. Costly Wi-Fi access point antennas tend to have very poor radiation diagrams and are spread as far as possible to optimise cost vs internet access. The result is a density of access points and a coverage that does not allow the kind of application presented in this work. Finally, Bluetooth technology is adopted massively across sectors, which enables low prices for electronics compared with any other technology. This is key for the mass adoption of RTLS solutions in hospitals. While not as accurate as UWB, Bluetooth can provide accuracy of around one metre, which is enough to solve the problem and optimise the cost-effectiveness of the presented use-case.
The Bluetooth solution consisted of two main hardware elements: a patient tag and a series of gateways (Fig 2).
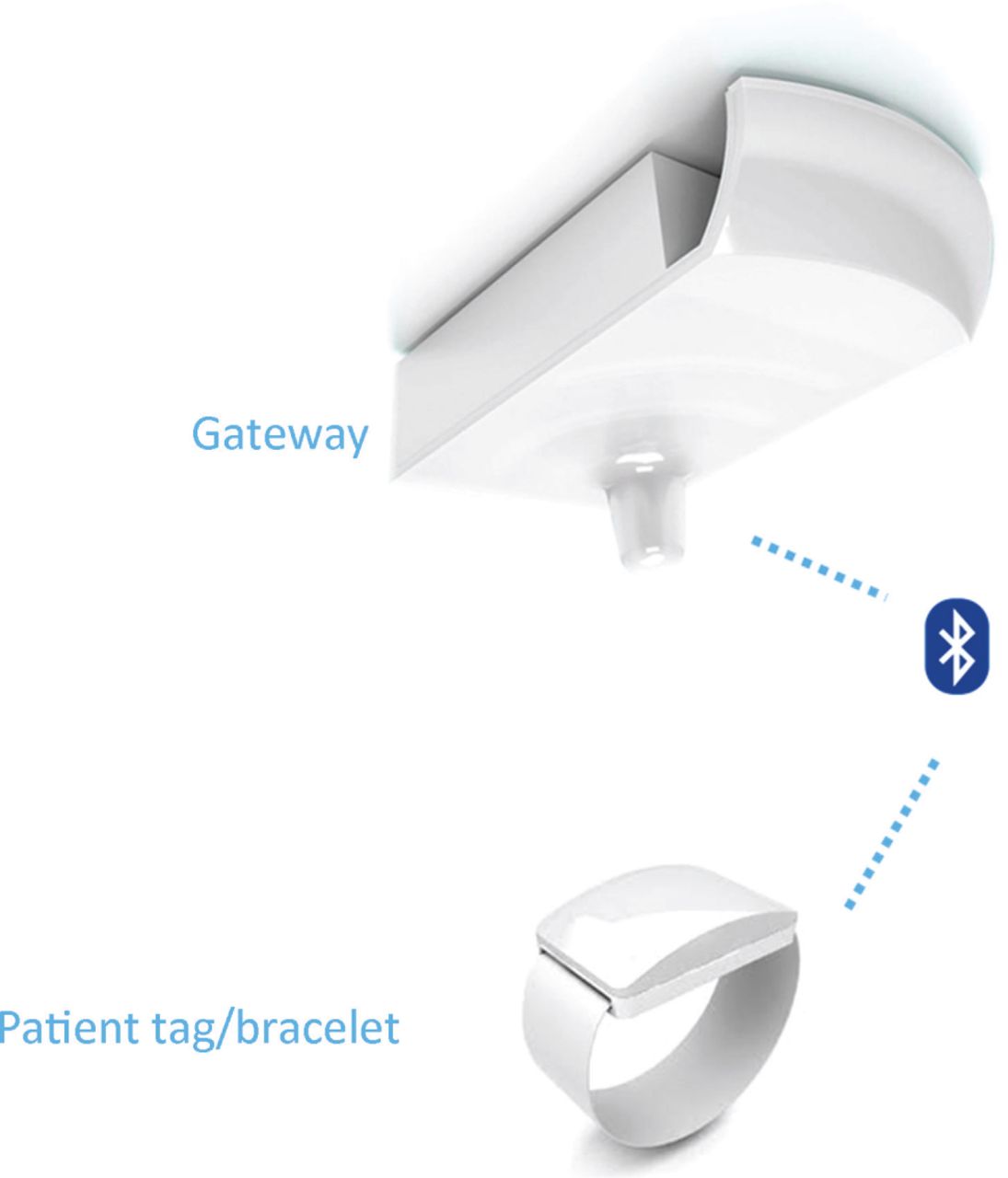
MYSPHERA's real-time location systems hardware used in this intervention.
These gateways were installed strategically across the surgical ceiling to record the patient journey in real time. In turn, this generated the live data and location events to automate the intervention. The next step was to develop a platform that was able to leverage the real-time data and to orchestrate the process automatically while engaging each of the teams with tailored applications. These applications provided patient-flow live data, notifications and tasks as patients moved concurrently across each step of the surgical process. Patient and operating theatre flows were visualised showing their current status. Most remarkably, it was decided that automated notifications would be sent to:
PACU to improve bed management with seamless communication with admissions and theatres areas
PACU and porters to speed up patient transfer to theatre as soon as it was ready (ie that was generated by detecting that the theatre is in ‘clean’ status and the patient is ready to be transfer to the PACU area)
cleaners to reduce times between cases, activating faster theatre cleaning.
Applications were presented as agreed with the team specifications (ie large screen panels as well as the use of their PC/laptops in PACU and admission areas, touchable screens in theatres, handhelds for porters and cleaners to support jobs reception in mobility scenarios, and panels and handhelds for relatives).
Intervention roll-out strategy
The new intervention was structured in two main phases (Fig 3).
Phase 1 (2017): the RTLS solution was installed to set the performance baseline and standardise pathways with real and accurate times. As a result, the real surgical block behaviour could be monitored, enabling the identification of inefficiencies, bottlenecks and improvements.
Phase 2 (2018 and 2019 onwards): this was built upon the RTLS solution, the new digital intervention was released adding the tailored applications for each team.

Phases of the study. RTLS = real-time location systems solution.
Patient pathway
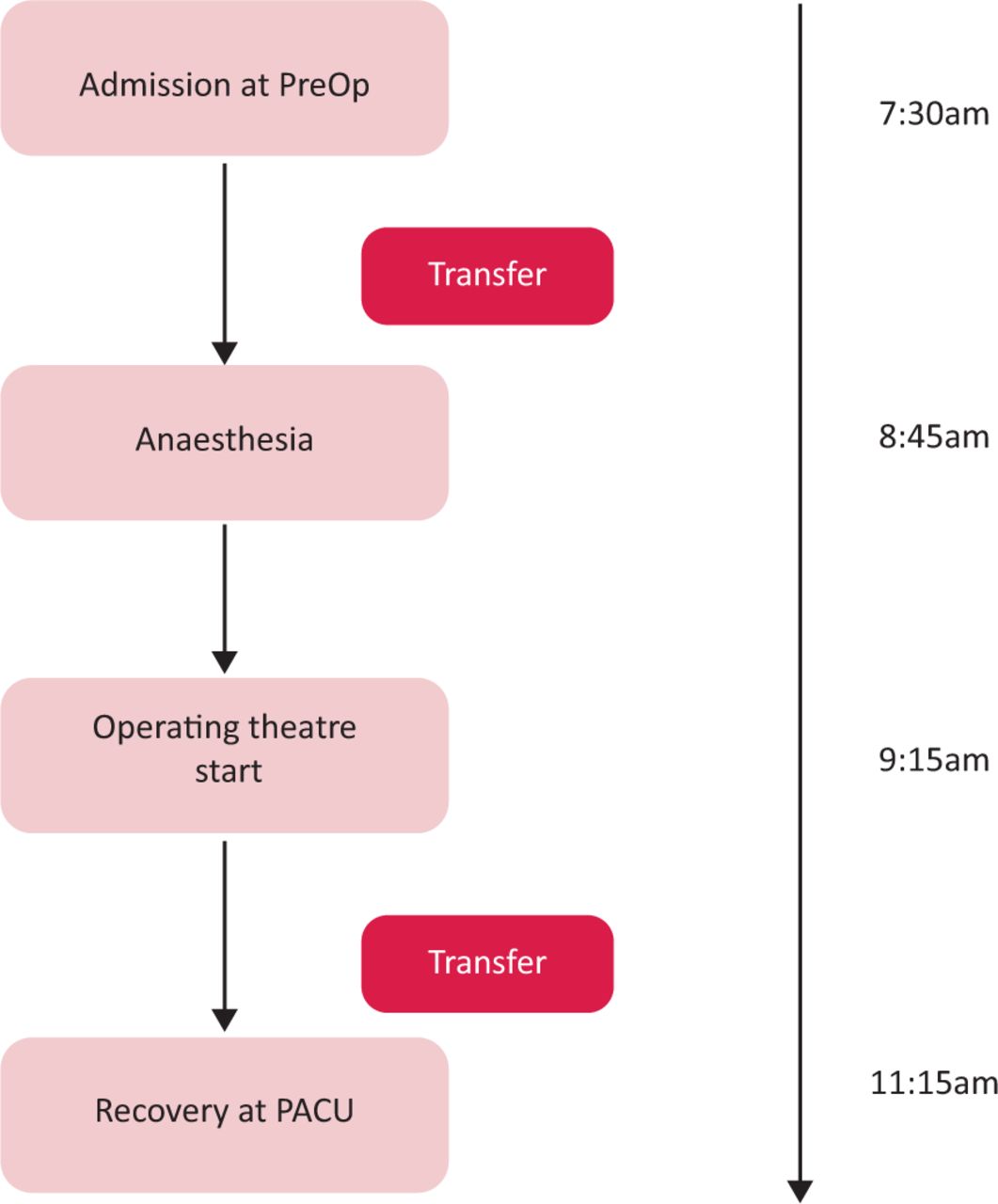
During the first 3 months of the implementation of phase 1, a monitoring study was carried out on the first patients in the surgical slots. A total of 52 patients were counted, giving a standard pathway (ie admission at pre-operation, then anaesthesia start, then operating theatre start then recovery at PACU). The gathered average process time is shown in Fig 4.
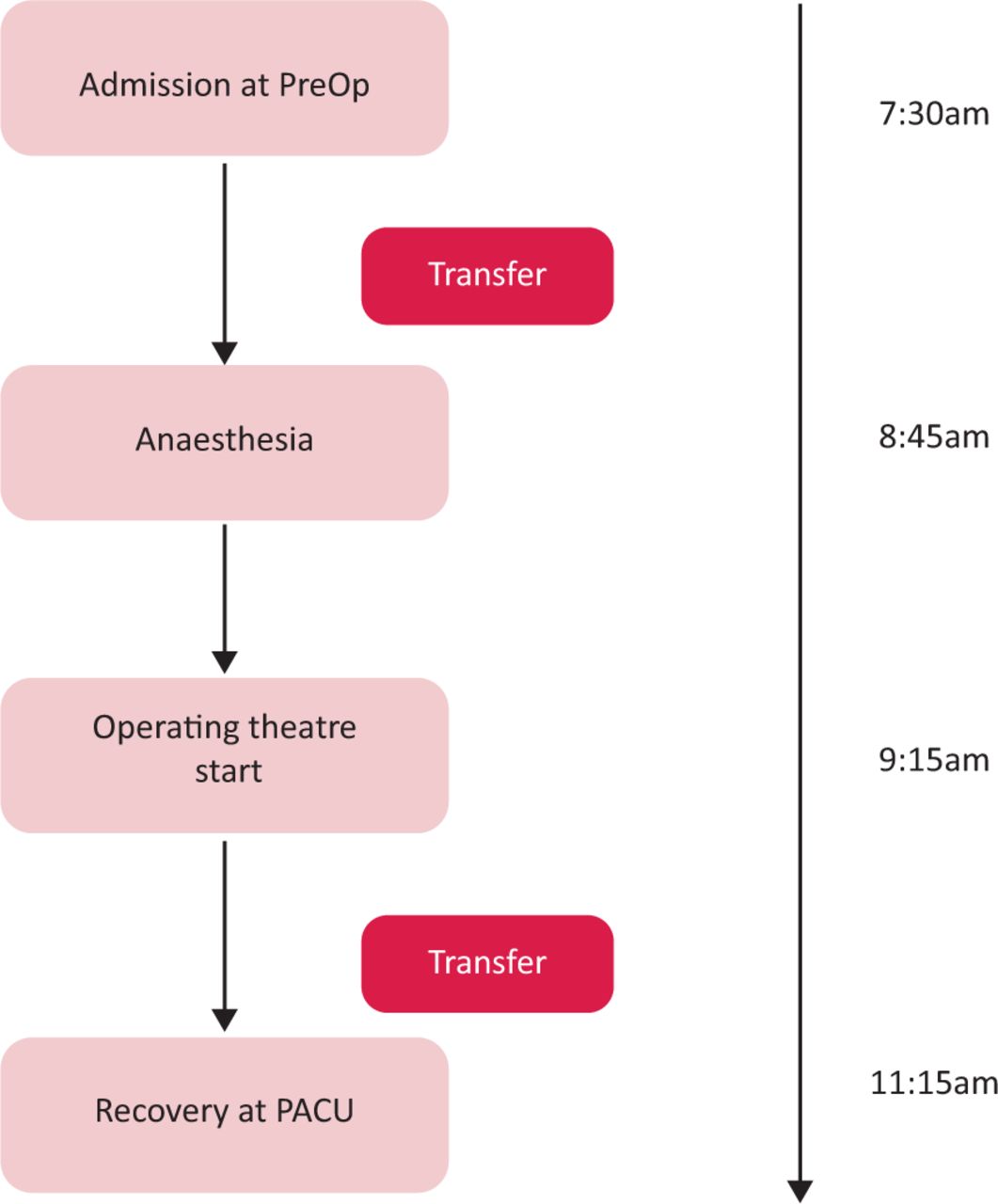
Average pathway steps and times during phase 1. PreOp = pre-operation.
Across many different interventions, the average surgical process time had a duration of 4 hours.
Endpoint monitoring
To assess the surgical block performance, the following endpoints were monitored over several years (Table 1). A more detailed table can be seen in supplementary material S1.
Endpoint monitoring and surgical key performance indicators
Data collection
This was an observational pilot study done in one centre with the goal of evaluating the implementation of a new RTLS patient-tracking system. There were no direct patient data involved. In fact, the patient Bluetooth tag does not transmit any sensitive data, only an anonymised ID. Thus, patient consent was not required by the hospital. Data collection was based on the real times captured by the new RTLS solution, which were automatically registered in the hospital's electronic medical record (EMR) system based on SAP (Feltham, UK) technology. While times were registered on a regular basis, outcomes based on those times were aggregated and calculated on a yearly basis (Table 2).
Data sampling
Staff training
As staff were involved in the co-creation process, final apps were highly tailored according to clinical feedback to ensure a high level of usability. As the use of the new apps was meant to be very straightforward, only a maximum of 2 hours of training for the new service was required. The idea was to replace the old ways of working (consisting of manually operated boards in combination with continuous phone calling) with screens with updated real-time information. A training plan was implemented targeting specific groups within the surgical teams. To optimise engagement, training sessions were planned a week before the go-live date, following the group distribution in Table 3.
Training groups
Administrative clinical staff were given a bit more time as they received training in patient tag assignation and un-assignment, which included the use of specific hardware and a standard cleaning process for the reuse of tags for other patients. During the first 2 weeks after the go-live date, a more intensive on-site support to solve issues that arose and to help staff with questions was provided.
Solution deployment
Phase 1 deployment involved MYSPHERA in the installation and adaptation of the RTLS system in the general surgery area. This included two design sessions with key surgical stakeholders to understand patient flow in the surgical block and the installation of the Bluetooth gateways in the right locations. Several check-ups were carried out to verify that patient flows were captured without any black spots.
As Wi-Fi and Bluetooth share the same frequency band, MYSPHERA's Bluetooth gateways use a special channel within its radiofrequency band to avoid any interference with the Wi-Fi access points already in place in all hospitals. Furthermore, this solution passed the CE mark, which involves being compliant with electromagnetic medical equipment compatibility tests specified in the European directive EMC 2004/108/EC. These tests verify each device from two aspects: emission and electromagnetic immunity.
Another critical aspect of deploying a RTLS was the integration with the hospital EMR system, a powerful integration software tool that allowed a fast interoperability with Vall d'Hebron's EMR was used. This allowed adaption to timestamp location data generated by the new solution to health level seven (HL7) standard messages used by the hospital to register them into its EMR. Another essential integration was with the theatre management system, which passed the surgical list of patients in a daily basis so that the solution could orchestrate the workflow in real time.
Phase 2 was focused on deploying the new automated workflow platform and tuning the possible patient pathways. A remarkable aspect of Vall d'Hebron was the fact that the PACU area suffers a lot of pressure as it receives patients for preparation but also those in recovery. Thus, flows are mixed in this area and the new solution had to be flexible enough to model patients in the same physical space but in a different step in the surgical process in real time. Phase 2 was refined gradually as it did not involve any RTLS hardware, already installed in phase 1.
Solution running
As with any new digital service, technical support needed to be in place, establishing a flow chart to escalate incidences according to the level of severity. MYSPHERA provided a list of potential risks and response times accordingly as part of the service level agreement (SLA) between the hospital and the company. Thus, IT technical support level 0 and 1 was provided by the hospital, while for more in-depth technical support MYSPHERA was involved. A ticketing platform based on Jira (Atlassian, San Francisco, USA) was used to coordinate the incidents. In general, the new service has been very stable. Most of the issues reported were due to refinements in the information shown by the apps and corrections in gateways location at early stages. For rare situations, such as databases running out of space or any problem with the server, MYSPHERA provided a continuous monitoring system that allowed the prevention of downtime situations and the correction of any technical problem in advance. A back-up system was not necessary as this was not seen as a critical service by the hospital and the technical support provided by MYSPHERA guaranteed the required quality of service. In the whole phase 2, 156 minor events were recorded, most of which could be sorted out quickly and remotely. No downtimes caused by the RTLS solution were observed.
Results
The aggregated theatre utilisation in 2017 was 70.02%, far from the optimal goal of 85%. By the end of 2019, the general surgery block was close to the optimal performance, reaching 82.5%. That increase propelled surgical activity from 8,154 operations in 2017 to 9,235 in 2019. These improvements in theatre productivity were possible for the combined breakthroughs on key performance indicators (such as late starts, early finishes, turnaround times and downtimes between cases; Table 1). Furthermore, the new way of working drove global process gains and saved nurse time as a result of better coordination between teams and automating activity registering into the hospital's EMR. Interestingly, the access to accurate times and real-time applications allowed better scheduling and activity management, which seems to have had an impact by reducing the number of operations that need to be extended and, in turn, producing fewer cancellations on the day.
Cost assessment
The increase of surgical activity enabled the addition of 577 new operations in the block in 2018, which, at an average cost of €3,258 per surgical intervention, represented an economic gain of €1.88M. On the other hand, the cost of a RTLS project varies depending on the rooms, corridors and size of the area to cover. It is also important to consider the types of surgery and other aspects including screens and smartphones for professionals, app adaptations according to staff needs, and number of integrations to be performed with the hospital system. According to MYSPHERA and taking in consideration the scope of this project (ie size, 19 operating theatres and other rooms, integrations, and adaptations), the market price of this project is about €425,000, which gives a return of investment (ROI) the very first year of implementation of 342%.
Discussion
The significant surgical performance improvements obtained in 2018 and 2019 are clear. They are the consequence of a combination of transformations, which were prompted by genuine interest and change in cultural attitude to improve the surgical process. This was part of an overall strategy to optimise the patient pathway using a ‘lean’ approach. Thus, as the hospital was measuring process times provided by the new solution, this information revealed important opportunities. Specifically, in phase 1, it was revealed that average late starts and theatre downtimes between cases could be improved significantly, especially during surgical session changes, to increase capacity.
As a result, by early 2018 (phase 2), more activity could be scheduled simply by making a better use of the slots in each surgical session. Furthermore, as the optimised and automatised process was launched in phase 2, notable team coordination gains were obtained. ‘Corridor-shouting’ was replaced by straightforward communication between theatres, preparation and recovery areas, porters, and cleaners. Casual testimonials from the various stakeholders, including families, suggest an increase of satisfaction as the pathway experience improved. It has been calculated that 5 minutes of nurse-time per operation has been gained by eliminating the manual data entry of activity into the information system. Furthermore, surgical patient journeys have been reduced, on average, by 15–20 minutes as a result of optimised coordination across the process. All in all, the gains in process times and theatre utilisation have allowed an increase in the number of surgical interventions, year after year (Table 1).
Verbal feedback given by all groups of surgical staff encourages us to think that satisfaction across all staff members has improved significantly. Interestingly, porters were the group who proactively continued to ask for additional features in their smartphone app. It might be that they are more visible and now feel more engaged, part of the team and recognised for their key role in smooth delivery. No problems related to feelings of been spied upon have been reported to date. Our impression is that involving all the different stakeholders during the creation of the new apps has helped to integrate different perspectives and needs, and has showed that the change was implemented to support staff and not to spy on anyone.
Likewise, the feedback given by families is very positive too. Typically, family members would have to waylay health professionals in hospital corridors to find out what was going on with their loved ones. Now, they can check real-time information on the waiting room screens and they can also use the smartphone app at home. As these messages are automated by the platform, messages are delivered as soon as a new status change happens. This system hardly caused any problems and, in the case that problems do occur, personal feedback is always part of the back-up plan. It must be said that professionals have also felt the relief of improving this critical part of the process. In phase 2, the solution was rolled out on a new site that undertook daily surgery with six theatres. The preliminary results obtained suggest an even greater increase of activity as shorter procedures provided greater opportunity to schedule more operations. A dedicated study for this new site and the COVID-19 year will be considered. Although the first attempts to use RTLS technology in the surgery area are emerging, there are no similar developments reported in literature to compare. To our knowledge, this is the first time that the surgical process has been digitalised using this approach. The significant strain that surgery units endure, together with the specialisation of surgical blocks and the idiosyncrasy of each type of surgery, limits the implementation of randomised controlled trial (RCT) studies in the same hospital. It is difficult to compare the technology implemented in one block dealing with general surgery with another one (eg orthopaedic or daily surgery), that don't use the same technology, as operations, times and dynamics are very different. Multicentric RCT studies in this field are encouraged to overcome these difficulties.
Lessons learnt
The design of the new solution required several working sessions with a designated staff team acting as co-creators. A wide group of surgical professionals were involved, including nurses, surgeons, porters and a cleaning team. This was essential to reassure them that this new way of working was not to spy on them but to improve their daily work. Also, understanding how patient flows work and the architectural barriers of the unit is essential to enable an optimal design of the solution, avoiding blackspots and enabling a seamless real-time location experience as patients move along the process.
On another level, the usual problems of integrating a new IT system within the hospital can be smoothed using a powerful integration software and the light integration needs of our RTLS solution. The adoption of communication standards by many systems in the hospital allows for much easier and faster integration times.
Finally, a significant pain point in the general surgery unit process was due to some inefficiencies with the communication with the PACU area, both for the transfer of patients from pre-operation to PACU and for the coordination of transfers from PACU to theatre, and vice versa. The automation provided by the new solution allowed for notification of the teams when the patient and theatre were ready for the next step, which has mitigated a problem by eliminating many stressful phone calls through shared communication via real-time screens.
Conclusion
RTLS automated, patient-flow solutions can be used to support the standardisation and monitoring of patient pathway times across the surgical process. It is key to have an automatic and unbiased way to obtain accurate times for all stakeholders. This has been essential to implement the improvement strategy in the hospital. Furthermore, the new approach has shown how multidisciplinary coordination was driven among surgical teams by enabling real-time information and push notifications. The result has been more proactive delivery of care.
The results obtained suggest that the novel intervention could support significant improvements in productivity for elective care activity in surgery. The Vall d'Hebron University Hospital was able to meet the sudden increase of demand by implementing this novel innovation and subsequently went on to implement the same approach in its other four surgical sites, across 51 theatres. Lastly, this novel approach is currently being deployed in other international sites (such as in France, Belgium and in the UK's East Kent Hospitals University NHS Foundation Trust). Therefore, further opportunities to study the impact of RTLS patient flow solutions in the management of patient pathways will emerge.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj:
S1 – Extended information about measured endpoints.
Acknowledgements
Thanks to the contribution of the MYSPHERA team, which has developed a unique and novel technology that supports the automation of clinical pathways. Thanks also to to everyone at Vall d'Hebron University Hospital that contributed to and are using this solution. We would also like to thank Sylvia Jackob, the Project Officer of this European project, for the given support.
Conflicts of interest
Jordi Rovira joined MYSPHERA as he was doing his PhD at the Vall d'Hebron Barcelona Hospital Campus, leading to the European Innovation project, ‘Operating Room 4.0’ (OR4.0; grant agreement ID: 812386).
- © Royal College of Physicians 2022 All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.