
ABSTRACT
Hospitals have the potential to create value beyond the direct clinical care that they provide through tackling the social determinants of health as an ‘anchor institution’: shifting the way in which they employ staff; procure goods and services; use their physical and environmental resources and assets; and partner with others. However, the societal value of this work is not automatically or accidentally created, it must be intentionally designed and delivered, particularly if it is to tackle inequities.
This article proposes five equity principles for healthcare leaders to consider in their hospitals' anchor institution work. There have already been important shifts from the ‘traditional way’ of conceiving of a hospital's role in the community, but going ‘one step further’ could help to maximise the equity impact.
Introduction
A core function of hospitals is to provide safe, effective acute and specialist healthcare to manage and treat a range of conditions. However, healthcare is not the primary determinant of our health. Our education, employment, income, housing, local community and other ‘social determinants of health’ (SDOH) have a much larger role to play.1–3 Their unequal distribution creates, and perpetuates, inequities in health; inequalities that are unfair and unjust.4 Acting on the SDOH could enable hospitals to go beyond the direct provision of clinical care and do more to improve health.
Increasingly, healthcare leaders are recognising that not only would this be desirable but it is also possible. In the UK and the USA, hospitals are looking beyond their traditional role, and are considering how they can create value by changing how they employ staff (and who they employ); procure goods and services; use their physical and environmental resources and assets; and partner with others: often referred to as acting as an ‘anchor institution’.
However, societal value is not automatically or accidentally created, it should be intentionally designed and delivered, particularly if it is to tackle inequities. It is vital to consider not only how to maximise value but also the distribution of that value. Herein, we propose five principles that we believe will help to embed equity at the heart of anchor institution work.
Hospitals as anchor institutions
The Health Foundation defines anchor institutions as large public sector organisations that are rooted in place and connected to their communities.5 Hospitals, as anchor institutions, can impact on the SDOH through influencing core business functions (Fig 1).
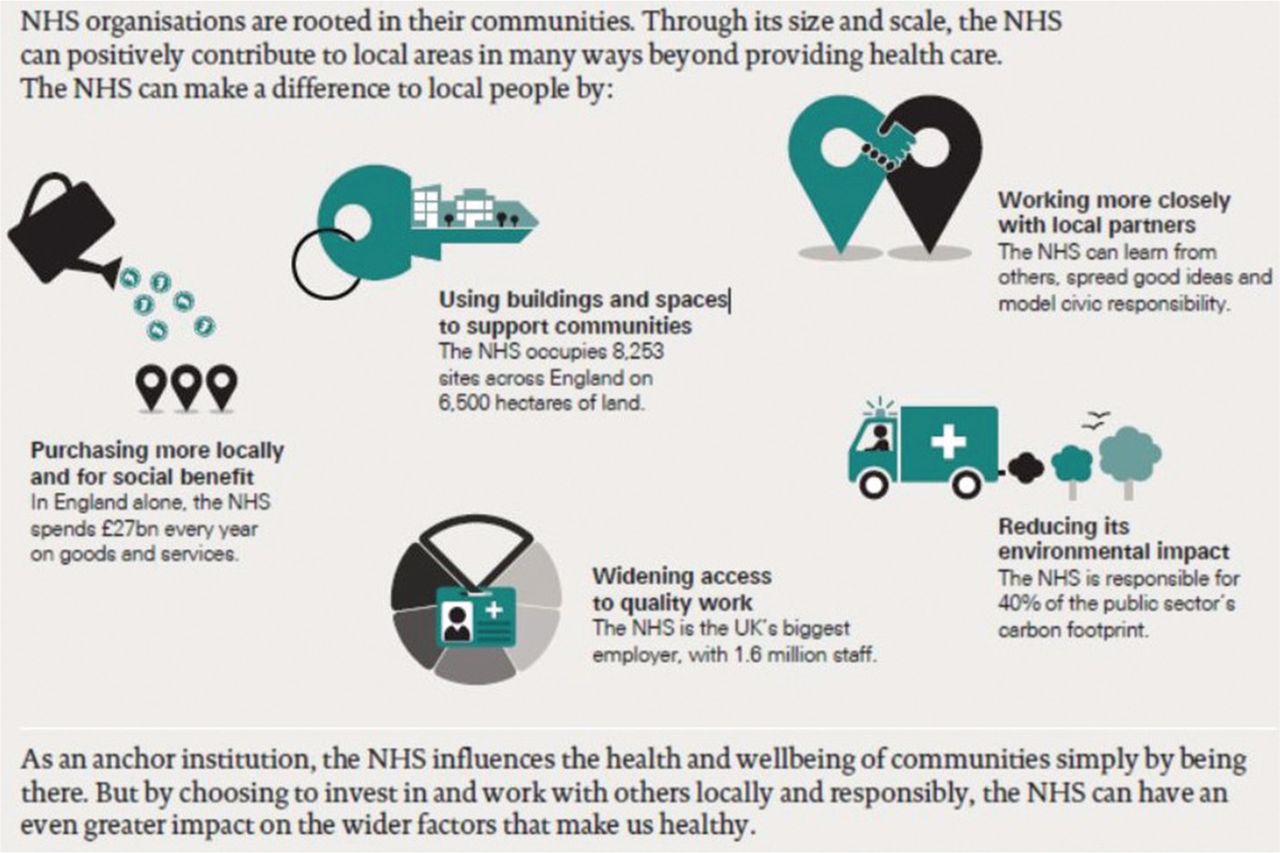
What makes the NHS an anchor institution? Reproduced with permission from Reed S, Göpfert A, Wood S, Allwood D, Warburton W. Building healthier communities: the role of the NHS as an anchor institution. The Health Foundation, 2019.
Since the publication of key healthcare policies and reports, there has been a noticeable increase in engagement with anchor institution work from healthcare organisations in the UK, including through both local activity and regional and national networks.6–9 COVID-19 provided additional motivation for hospitals to adopt anchor work.10 Anchor institution work also aligns with similar agendas, including community wealth building, social value, and the role of healthcare organisations in reducing poverty and acting on the SDOH.11–14 Much of the anchor work in the UK builds on similar approaches in the USA led by the Healthcare Anchor Network and a wider, growing literature on the potential for hospitals to go beyond being the ‘repair shop’ to act on the SDOH.15–17
Anchors and equity
Hospital anchor strategies often have an explicit aim of reducing health inequities in their local population, and the focus on the SDOH provides clear potential for success. However, we have often seen a kind of ‘magical thinking’, presuming that adopting anchor strategies will automatically reduce health inequities, without specifying how, for whom and in what ways this will be achieved.
The five principles presented each provide ‘one step further’, an additional consideration or broadening of accepted practice, that we believe would be helpful in ensuring the value created by anchor institutions is also reducing inequities (Box 1). Examples are provided from our insights in the UK and the USA of how hospitals are adopting these principles in their anchor work.
Five principles for embedding equity in anchor institution work
Beyond equality to equity and justice
There is an established difference between equality (treating everyone the same) and equity (ensuring people have the same outcomes), which may involve treating people differently. Within anchor institution work, there are important gains to be made by ensuring equality; for example, Imperial College Healthcare NHS Trust in-sourced their hotel services staff to ensure that they had the same quality of employment (rights, pay, and terms and conditions) as those staff that were directly employed by the trust.18
However, particularly within the employment pillar, it is important to consider equity as well as equality, meaning that a hospital may need to provide additional support to particular groups or populations to ensure they can benefit from a work experience offer or other employment support. Barts Health NHS Trust, for example, have recognised this in their ‘Community Works for Health’ programme, which works with partners (such as the local authority) to identify local candidates for vacancies in the hospital. Rather than providing the same offer to all, the programme offers additional support through adult learning or further education provision for those with low or no qualifications, or English as a second language. Since its inception, the programme has supported over 1,000 local people into NHS employment.19
The move from equality to equity requires thinking differently about how to measure and respond to a community's need. An essential component of equity is to consider justice (how to change systems and structures that create and perpetuate inequities) as well as recognising and responding to injustices (such as institutional racism within healthcare). Rush University Medical Center in Chicago focuses on equity as a health system strategy and have explicitly designed their anchor strategies to address structural racism and economic deprivation, including through ‘West Side United’, a collaborative of anchor institutions and other partners working together to reduce the gap in life expectancy between neighbourhoods in Chicago.20,21
Justice should include both a differential response to unequal levels of need and efforts to reduce the inequities in the first place. This could include, for example, working to ensure universal human rights or tackling hunger and homelessness.16
Acting on justice may be a less familiar approach or a new language to many UK hospitals, but has the potential to create lasting impact on health inequities, since the SDOH are themselves shaped by systemic inequities in power, money and resources.
As part of their work on equity and justice, some US hospitals are looking outside their own institution and using their social and political capital to advocate for policy change; for example, hospital staff from St Alphonsus Regional Medical Center in Idaho, USA, have successfully advocated at the state legislature for greater legal protection and financial assistance for renters, motivated, in part, by the large number of their patients reporting housing insecurity to the hospital (personal communication with Rebecca Lemmons, St Alphonsus Regional Medical Center).22
The US-based Healthcare Anchor Network expanded its portfolio in 2018 to include policy and advocacy and there may be a case to expand the definition of anchor institution work in the UK in a similar way.23 This could build on some early examples from UK healthcare institutions and their partners in advocacy work (such as Great Ormond Street Hospital who have engaged with policy change efforts to reduce air pollution, which disproportionately affects the most vulnerable).24,25 Healthcare system partners have also called on the UK government to take further action to protect the public from the cost of living crisis in order to reduce poverty and, therefore, improve health, and over 150 healthcare organisations including a number of NHS hospitals have publicly called for the reinstatement of the cancelled health inequalities white paper.26,27 While this type of activity does not currently fall under the generally accepted definition of anchor institution work, it is motivated by a concern for justice and equity in health.
Beyond individual projects to intentional and integrated anchor approaches
Even though anchor work can be a powerful tool to improve equity, most anchor activity won't automatically deliver on this potential unless equity is intentional within anchor approaches, and strategies focusing on equity are aligned and integrated across clinical and non-clinical activity in the organisation.
This expansion from siloed and isolated anchor projects to an organisation-wide, intentional and strategic approach requires that equity is prioritised throughout the life-cycle of anchor work. Considering local need is becoming a more familiar activity at the planning stage of hospital strategy development and anchor work, and significant data exists on place-based health inequities. However, this equity focus can ‘fall away’ as anchor strategies begin to be implemented. There should be clarity on the dimensions of equity being targeted and a continuous focus on equity.
It is also essential to recognise that while anchor work can contribute to health equity, it cannot deliver the full equity agenda alone. Anchor work is, by definition, primarily focused on the non-clinical aspects of a hospital's function and, therefore, even an excellently designed and delivered anchor approach will not achieve a hospital's equity aims in terms of access, experience and outcomes of clinical care.
Hospitals can strengthen their anchor work and potential impact on equity by aligning with other organisational work and strategies to achieve equity aims. Both Barnsley Hospital NHS Foundation Trust and Imperial College Healthcare NHS Trust, for example, have integrated their anchor work with wider population health and health equity strategies.28,29 Alignment of priorities can include work in quality, improvement, integrated care, health improvement, digital, and net zero or carbon reduction work. Equity aims will often be similar, and there is much to gain by ensuring better alignment and sharing learning and approaches between teams and work.
Beyond solely local to equitable and proportionate
Hospitals adopting anchor strategies have often successfully moved beyond a traditional healthcare focus on patients and services, looking instead to communities and the places in which they live, and strengthening local partnerships.
However, working locally does not automatically result in a reduction in inequities. Many hospital footprints will include multiple neighbourhoods that vary in terms of deprivation and health outcomes. If hospitals do not effectively consider these local inequities, their interventions could benefit only relatively healthy local areas, potentially increasing inequities and leaving behind areas more in need.
Adding an equity lens to a local frame allows hospitals to identify and target areas of greater deprivation or communities that have historically been excluded from opportunities (such as employment or procurement contracts); for example, Leeds Teaching Hospitals NHS Trust have targeted employment opportunities to local communities in the 20% most deprived areas nationally, and are measuring the proportion of their employees drawn from these areas.30
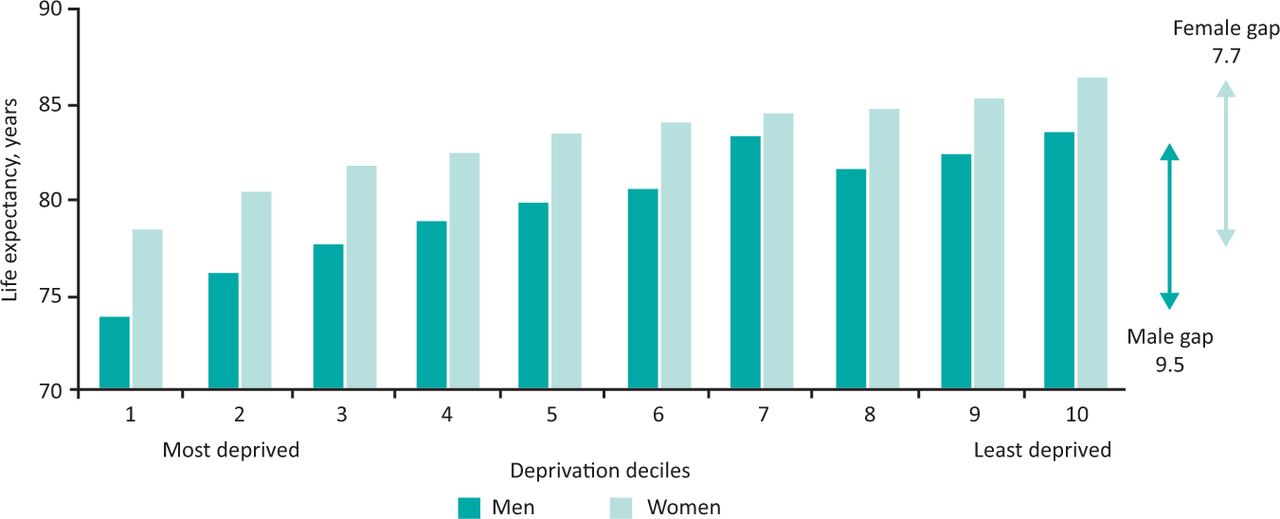
Hospitals seeking to tackle inequity through their anchor work can also adopt a ‘proportionate universalism’ approach.4 This recognises that health inequities are consistently patterned along a gradient. They are not simply a case of those ‘with’ and ‘without’ good health; at every level of deprivation below the least deprived, people experience slightly worse health (Fig 2).31
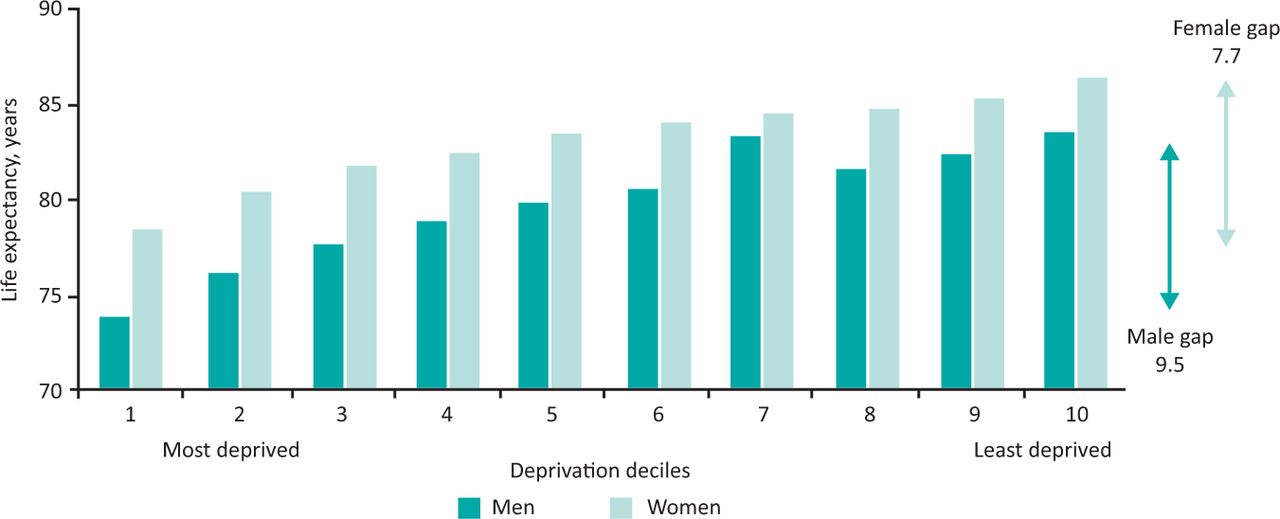
Life expectancy at birth by area of deprivation deciles and sex, England, 2016–2018. Adapted with permission from Marmot M, Allen J, Boyce T, Goldblatt P, Morrison J. Health equity in England: The Marmot Review 10 years on. Institute of Health Equity, 2020.
A proportionate universalism approach makes proportionately more available to those lower down the hierarchy: delivering programmes and resources at a scale and intensity proportionate to need; for example, MetroHealth in Cleveland, USA, are taking an anchor approach to their hospital redevelopment, providing a community green space, low to moderate income housing, an economic opportunity centre, education provision, a community kitchen and other community assets. While these will be available to all local people, they are designed to be proportionate to need, with increasing support for and outreach to those on lower incomes (personal communication with Gregory Zucca, MetroHealth).
Beyond traditional patient involvement to community partnership
In recent years, the importance of patient and public involvement and engagement has increasingly been recognised as an essential strategy to improve NHS quality and equity. However, anchor strategies that prioritise equity require hospitals to expand from individual patients to whole communities; from consultation and feedback to power sharing and partnership; and from a focus on services and the hospital as an institution to a place-based view: looking out rather than in.
As part of this shift to considering communities and the places they live, hospitals often have to build new, different or stronger partnerships with non-healthcare organisations (such as local authorities, education and, voluntary, community and social enterprise organisations).32 Importantly, as hospitals design and deliver their anchor strategies, they should be ensuring that these intentionally build capacity in the community sector, rather than just utilising local community partners for hospital benefit. This may involve sharing resources (financial and other) and working for sustainable collaborations rather than one-off project-based partnerships.
However, sustainable and systematic impact on equity is likely to require not only good partnership work with local organisations but intensive and open power-sharing with local communities. This could build on the principles of asset-based community development, which recognises communities not as collections of needs and problems but as powerful sources of talents, skills and assets.33
Providing community power-sharing work with significant time, resource and effort can help hospitals to design and deliver effective anchor institution work, and also to ensure equity of impact as local inequities are often the product of multi-factorial, complex, long-term factors that are best understood by those who experience them, rather than institutions (Box 2).
Anchor institution work at the East London NHS Foundation Trust
Beyond short-term and immediate to long-term and wider impact
Healthcare funding, programmes and measurement often operate on a relatively short time frame, and the average tenure of hospital executive leaders in the UK is only 2 years.34 However, reducing health inequities through action on the SDOH is a long-term endeavour, entrenched and complex systems of power and privilege take time to shift. Anchor work, therefore, needs vision and commitment that outlasts short funding cycles and board level turnover.
Initially, anchor programmes and activities may benefit from the acceptability and available resources associated with a short timescale. Short-term measurement can also be valuable, to modify programmes to improve and learn, and to justify further institutional attention and investment where positive impacts are seen. Utilising a range of metrics, creating a central role for qualitative feedback from staff and local community members, combining data and insights, and ensuring an ethos of continuous learning are all essential to successful delivery and measurement of anchor programmes.
Mid and South Essex NHS Foundation Trust anchor programme has developed a workforce dashboard that measures progress against anchor recruitment and retention measures and is developing a wider measurement dashboard that provides real-time feedback on progress against wider anchor targets.35 A recent evaluation report showed that work to widen workforce participation among residents of particularly deprived areas has a client group of which 79% are claiming benefits, demonstrating the programme's success in reaching those most in need of support.36
However, hospitals seeking to invest in and measure anchor work can find that it is harder to understand and justify interventions where the benefits might accrue to other organisations (a ‘wrong pocket’ issue) and/or only be seen in the long term, outside of normal healthcare funding cycles (a ‘long pocket’ issue).
While constraints and disincentives exist, leadership is needed to encourage a culture change, recognising that long-term outcomes that benefit many sectors is positive, a sign that the work is focusing on SDOH. This may require supplementing healthcare metrics with data from other sources; for example, the affordable housing provided by Bon Secours Hospital in Baltimore, USA, has been shown to produce a significant social return on investment: every dollar spent resulted in estimated benefits of between $1.30 and $1.92 across a range of economic, social and environmental impacts.37
Cincinnati Children's Hospital in the USA has measured positive healthcare impacts of SDOH work in the short term; a programme that refers urban, low-income families in need of legal support to a medical–legal partnership resulted in a 38% drop in hospitalisations among children in the year after the referral compared with a control group of children also seen by the hospital but not referred.38 However, their collaborative ‘All Children Thrive’, a learning network of Cincinnati partners working together, also focuses on the long term, uniting partners around the goals of eliminating infant mortality, ensuring all 5-year-olds have a healthy mind and body, eliminating neighbourhood disparities in inpatient bed days, and ensuring all children can read proficiently by the third grade.39
Conclusion
Anchor strategies provide an opportunity for hospitals to increase the societal value they provide, and acting as an anchor institution can be a powerful approach to reduce health inequities through action on the SDOH. However, anchor strategies don't automatically reduce inequities, this impact must be carefully designed and delivered.
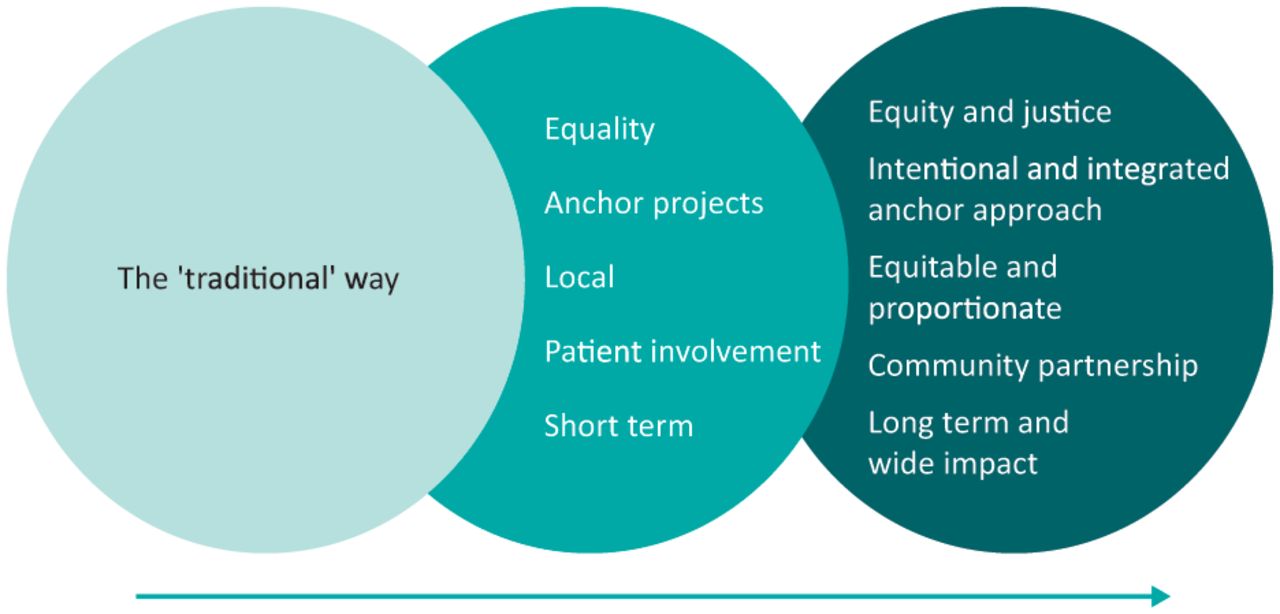
Herein, we have proposed five principles for healthcare leaders to consider in their hospitals' anchor institution work. There have already been important shifts from the ‘traditional way’ of conceiving a hospital's role in the community, but going ‘one step further’ could help to maximise the equity impact (Fig 3).

Five principles for moving anchor institution work towards equity.
It is important to consider equality, but more can be gained by also ensuring equity of impact and working to increase justice. Anchor projects can evolve into an intentional and integrated anchor approach across an organisation. Thinking about local impact is essential but insufficient; instead anchor work must consider how to act equitably and proportionately within a local area. Patient involvement is unlikely to have the power-sharing impact that genuine community partnership could achieve. And finally, while we must measure impact in the short term, it is also vital to know the impact that we have in the long term and across multiple sectors.
While adopting these principles may have other benefits, our focus has been on their potential to embed and ensure equity. We believe that ‘doing anchor well’ doesn't just mean having lots of projects, demonstrating a certain scale of investment or even positive impact on process measures and outputs in the aggregate, but also ensuring that anchor work is successfully reducing health inequities.
Closer scrutiny of anchor work is essential to consider as healthcare goes through policy and delivery shifts and, particularly in England, as integrated care structures and collaboratives develop. In addition, while we focus on hospitals, the lessons may also have wider relevance to other healthcare organisations and systems (including integrated care systems, integrated care boards and primary care) and to other anchor institutions (including local authorities and universities).
As with any proposed increase in scope, these principles could be criticised for requiring a potentially impossible increase in resources and stretching of bandwidth at a time when hospitals are facing multiple crises and operational challenges (including long waiting lists, staffing shortages and limited funding). However, in a context where the urgent can crowd out the important, it is essential to scrutinise and evaluate existing anchor work, especially when this is already using valuable scarce resources, to ensure it is having the impact and fulfilling the equity promise that we hope it will. In addition, most of the expansions we propose in this piece can, at least in part, be achieved by changing how anchor work is framed; they do not necessarily require a doubling of resource, for example. For hospitals already committed to anchor work, these expansions could help to maximise impact. For those not yet engaged, we hope they will be inspired by the potential to improve equity.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.