
ABSTRACT
England's current review of clinical negligence and consideration of alternatives (such as no-fault compensation) should be welcomed. Valuing what patients and families want, and need, after harm in healthcare necessitates a system that enables their needs to be met. Medical negligence litigation is misaligned with patients’ needs after harm events. By contrast, alternatives (such as no-fault and communication-and-resolution programmes) offer opportunities to place patients’, families’ and providers’ values at the forefront of resolution efforts. This article offers empirical insights and lessons from two alternative systems for resolving medical injuries: New Zealand's (NZ's) administrative compensation scheme, and the US communication-and-resolution programmes (CRPs). The review in England presents an exciting opportunity to design a system for responding to medical injuries that harnesses the strengths of alternative approaches for resolving medical injuries, while also improving on the challenges with treatment injury in NZ.
Introduction
Families are often coping with the demands of looking after a brain injured child and are not always emotionally ready to pursue a claim and when they do those who earn more often get a higher level of financial settlement. This is grossly unfair and needs to be changed completely.1 Stephanie Prior, head of medical negligence, Osbornes Law, London.
Prior's observation not only captures one of the many miseries of medical malpractice litigation for patients and families, but also highlights the importance of the British government's announcement in 2021 that they will review medical negligence and consider replacing it with an alternative system, such as an administrative no-fault compensation scheme.2 In a letter to the prime minister, the Medical Defence Union, The Academy of Medical Royal Colleges and the Hospital Consultants and Specialists Association have ‘sought urgent reform’ of clinical negligence in England.3
The latest call for urgent reform is not surprising given the well-documented, and long-standing, evidence from patients, healthcare providers and lawyers that medical malpractice litigation is unsatisfactory, slow, unpredictable (referred to as the ‘liability lottery’ in negligence), stressful, traumatic and unfair for all parties, and, therefore, does not meet their needs.4 Furthermore, it is well-documented that medical malpractice litigation stifles the patient voice and harms patient–provider relationships by, for example, conceptualising patients as adversaries rather than partners. These issues hinder transparency and communication, and perpetuate distrust, inequities and inequalities; thus, disproportionately disadvantaging ‘vulnerable’ populations. The evidence also documents the adverse impact of medical malpractice litigation on healthcare; for example, it is misaligned with health policies on quality and safety in healthcare and encourages defensive medicine and a punitive, blame culture.5 Moreover, medical malpractice litigation is expensive; for instance, in the past 10 years, the cost for annual clinical negligence claims for the NHS has risen by over 200%. A significant amount of this rise is related to the discount rate, which was changed from 2.5% to −0.75% in March 2017 and −0.25% in March 2019. These changes have had a disproportionate impact on future cost calculations. Nevertheless, research has demonstrated that medical negligence litigation is more expensive than its alternatives, such as no-fault compensation.
Overall, medical negligence litigation is an anathema to values in healthcare, particularly patient-centred care. Medical negligence and tort law is underpinned by functions and values (such as compensation, deterrence and, some would argue, retribution). However, many commentators have questioned whether torts law fulfils its purposes.6 The Harvard Medical Practice Study found also that most Americans injured by medical malpractice do not receive compensation when they litigate.7 Recent studies report that it is difficult for injured patients in the USA to find lawyers to take their cases, and defendants win in approximately 80% of cases.8 Torts law is an area of private law concerned with our obligations to each other, how people should treat one another and the principles for determining when compensation for harm is due. Torts cover harms related to a range of issues, such as trespass, defamation, nuisance and negligence. For medical negligence, there is strong evidence that the torts system fails patients, families and providers.9 In addition, there is very little evidence that injured patients and families want retribution after harm in healthcare.10
If we are serious about valuing what patients and families want after harm in healthcare, we need a system that enables their needs to be met. Medical negligence litigation is a system that cannot be aligned with patients' expressed values and needs when harm occurs; for example, it is well-known that medical negligence litigation facilitates a ‘deny and defend’ approach following medical injuries, whereas alternatives (such as administrative no-fault compensation) facilitate a ‘disclose and apologise’ approach.11 The latter is aligned with values-based bioethics and the values and needs of patients, families and providers. There is both normative and empirical evidence that alternative approaches to medical malpractice (such as the US communication-and-resolution programmes and New Zealand's (NZ's) no-fault administrative compensation scheme) are underpinned by values that are aligned with patients’ and providers’ needs following harm in healthcare.12,13
This article offers empirical insights and lessons from two alternative systems for resolving medical injuries: NZ's administrative no-fault compensation scheme and the US communication-and-resolution programmes (CRPs). NZ's administrative no-fault compensation scheme, the Accident Compensation Corporation (ACC), is a tax-funded, government-administered body. The scheme covers all personal injuries, including medical injuries. The community assumes responsibility for injuries. Injured New Zealanders are statute-barred from bringing civil claims in personal injury. By contrast, the US CRPs are concerned only with medical injuries. They operate within healthcare providers and operate alongside medical negligence. CRPs offer not only ‘open disclosure’ but also other remedies (such as compensation).
By their nature, CRPs are less onerous to implement than administrative no-fault schemes because CRPs do not require an entire system overhaul. A CRP-style alternative may be considered irrespective of government appetite for a large-scale reform of the entire personal injury system.
Despite critiques about administrative compensation schemes, and communication and resolution programmes, the evidence suggests that these alternatives are, nonetheless, preferable to medical malpractice litigation.14 The alternative systems place the needs of the injured at the centre, which is consistent with patient-centred care. The alternative systems are underpinned by values (such as honesty, disclosure, transparency and communication) that are consistent with the needs and values of injured patients. The alternative systems also cost less money.15
A system and culture that facilitates the over-arching value of ‘doing the right thing’ when ‘things go wrong’ in healthcare is important because researchers have consistently found that, firstly, the organisational culture, values and systems-level environments can influence practitioners’ behaviour more than personal morals and values; and, secondly, when practitioners share the values of the organisation and system, they are more likely to remain in healthcare work and provide high-quality and safe care.16,17
Patients' perspectives
A large body of international literature documents that injured patients and families value efforts to prevent recurring medical injuries.18 Patients value safety in healthcare and, when things go wrong, they value patient safety efforts so that other patients and families do not need to endure the same suffering. When harm events lead to death and investigations by coroners, the families reiterate the same need and value: they want efforts to prevent recurrences so that other families do not experience this distress.19 With an ACC or CRP approach, the value of patient safety is held higher than the need to assign individual blame. By contrast, assigning blame or fault is a required element in a torts action in medical negligence. Even if an injured patient plaintiff is successful in their medical negligence claim, the outcome will not involve patient safety learning because the main purpose of torts is to provide compensation.
The international literature also demonstrates that injured patients and families value disclosure discussions that are compassionate, efficient, transparent, honest and include a genuine apology.20 Following the dominant bioethics principles, healthcare providers should be guided by moral principles, such as beneficence, nonmaleficence and respect for patient autonomy. Respect for patient autonomy involves, among other things, informing patients and families of what happened when harm occurs. Unfortunately, however, legal action in medical negligence is primarily concerned with proof of the elements of the tort (duty of care, breach and causation) and not with facilitation of compassionate disclosure communication. Indeed, there is evidence that health providers are unable to undertake such communications in the context of a medical negligence claim.21
A system that values integrity will support individuals to do the right thing and, thus, meet the needs of patients and providers following medical injuries. By contrast, a system (medical malpractice) that emphasises liability (identifying someone at ‘fault’ who ‘caused’ the injury) will support an environment that undermines the values and needs of providers and patients following medical injuries.
Lessons from NZ's ACC
The ACC scheme: purposes, values and operation
NZ's 1967 Royal Commission of Inquiry report identified the numerous shortcomings of the torts system and recommended radical reform.22 Since 1974 (which was when NZ's Accident Compensation Act 1972 came into force), most claims for compensation arising from personal injuries have been statute barred and, instead, New Zealanders apply to the ACC scheme for rehabilitation and compensation. The scheme is not based on fault. Instead, the system is underpinned by distributive justice, aiming to spread the economic consequences of injury across the community.23 The underlying philosophy of the scheme emphasises community responsibility; therefore, ‘[it] is not an insurance scheme’.24 The current legislation is the Accident Compensation Act 2001.25 The core values are captured in section 3 of the Accident Compensation Act, which states that:
The purpose of this Act is to enhance the public good and reinforce the social contract represented by the first accident compensation scheme by providing for a fair and sustainable scheme for managing personal injury that has, as its overriding goals, minimising both the overall incidence of injury in the community, and the impact of injury on the community (including economic, social, and personal costs).
Despite amendments over the years (most notably in 1982, 1992, 1998 and 2001), the fundamental operation of the scheme remains the same. The right to claim compensation is based on the injured person coming within the statutory conditions for cover, not on questions of liability. The first step in the process for obtaining cover is that an injured person should get treatment from a healthcare provider. The healthcare provider should submit a claim to the ACC. If the injury is covered by the scheme, the ACC will pay part of the cost of the provider's bill and the injured person will pay for the remaining part of the treatment. Within approximately a week, the ACC will confirm whether the injured person is covered.26 An injured person who is covered by the scheme may be entitled to treatment, rehabilitation, earnings compensation and, if applicable, death benefits or lump sum compensation for permanent impairment. Table 1 compares administrative compensation to medical negligence in torts.
Functions, processes and remedies of torts and the Accident Compensation Corporation
The ACC scheme: treatment injuries
In 2005, the concept ‘treatment injury’ replaced the prior legislative provisions relating to ‘medical mishap’ and ‘medical error’. The amendment resulted from a 2003 government review that expressed concerns with the legislative concepts for medical injuries and their application.27 According to Prof Todd, the need to prove medical error was an anathema to a no-fault scheme and it ‘perpetuated a blaming culture and meant that the scheme was required to resolve the same kinds of difficulties that arose under the tort system that it replaced.’28 The 2005 amendments to medical injuries aimed to move away from negligence-type concepts and application; to facilitate cooperation between the ACC and the health sector; and to encourage learning, health quality and safety.
Pursuant to section 32(1) of the statute currently in force (the Accident Compensation Act 2001):
(1) Treatment injury means personal injury that is—
suffered by a person—
(i) seeking treatment from 1 or more registered health professionals; or
(ii) receiving treatment from, or at the direction of, 1 or more registered health professionals; or
(iii) referred to in subsection (7); and
caused by treatment; and
not a necessary part, or ordinary consequence, of the treatment, taking into account all the circumstances of the treatment, including—
(i) the person's underlying health condition at the time of the treatment; and
(ii) the clinical knowledge at the time of the treatment.25
Subsections (b) and (c) have generated much scholarly attention and legal action because they too often preclude injured patients from receiving cover from the ACC. The NZ courts have been tasked with delineating the boundaries of these statutory provisions.
Similarly, subsection 32(2) from the treatment injury provisions has also precluded injured patients from receiving compensation and attracted critique and legal action:
(2) Treatment injury does not include the following kinds of personal injury:
personal injury that is wholly or substantially caused by a person's underlying health condition.
personal injury that is solely attributable to a resource allocation decision.
personal injury that is a result of a person unreasonably withholding or delaying their consent to undergo treatment.25
Both 32(1) and 32(2) of the Accident Compensation Act require injured patients to prove that their treatment injury was ‘caused’ by treatment given or sought. Cover may be granted by the ACC in cases where there were multiple causes. For some treatment injury claims, demonstrating causation will not be onerous; for example, if a surgeon made an incision in the patient's right leg instead of their left leg, it will not be difficult, at law, to show that the treatment caused the injury.29 However, there are many cases where causation is contentious and precludes injured patients from being captured by the ACC scheme; for instance, causation is often contentious when an injured patient claims for the impact of a delay in treatment.
In ACC v Stanley, the injured patient suffered from a cervical disc prolapse that worsened because of a delay in proper diagnosis.30 The ACC refused to cover the patient's injury. However, on appeal, the court found that ACC cover could be granted for an ‘exacerbated personal injury.’ The injured patient had, therefore, on appeal, proven a treatment injury and could obtain compensation and other benefits. While this may seem a successful outcome for the patient, he had to endure the well-documented cost and stress of litigation to receive cover; a problem that the spirit, values and philosophy of the ACC was designed to avoid. Furthermore, legal scholars have noted that the judgment in ACC v Stanley can be interpreted as an exception to the general rule that exacerbation of a pre-existing condition does not constitute a personal injury.22 Legal scholars have written extensively about a multitude of other barriers to successful claims by injured patients that these causation provisions create. According to Todd, for example, ‘While negligence is not formally required, all of these points suggest that it necessarily reappears in deciding whether treatment injury can be shown to exist.’28
Although, the ACC scheme, overall, attracts widespread support in NZ (even across political lines), there is growing public discontent about the treatment injury provisions. Information released under NZ's Official Information Act, and published in the media this year, revealed the information about treatment injury claims from 1 July 2011 to 30 June 2021:
total claims lodged: 138,810
claims accepted: 89,656
claims declined: 49,154
reviews of decisions: 2,715
district court decisions: 209
court decisions upholding ACC: 152.31
According to the ACC website, approximately 37% of treatment injury claims are declined.32 The purpose of the this critique of NZ's treatment injury is not to suggest that medical malpractice litigation should be maintained in England. The point is to highlight how reformists in England could improve upon NZ's approach to treatment injury, should they decide to replace clinical negligence with no-fault compensation.
Lessons from patients, providers and ACC lawyers
The promise of, and problems with, the ACC's treatment injury were examined in research undertaken by Profs Mello and Bismark, and myself. We explored the experiences of patients and family members with medical injuries, and non-litigation approaches to ‘resolution’, to understand the different aspects of organisations’ responses to medical injury that facilitated and impeded resolution.8,19,21,33,34 Overall, the results from this project added more granular detail to the fundamental principles about injured patients’ needs, also outlined earlier. The findings highlighted the core needs and values of patients and families involved in harm events. Firstly, they value tailored responses, rather than ‘one size fits all’ responses to medical injuries. To facilitate a tailored response, organisations involved in ‘resolution’ should ask, rather than assume, what patients value, want and need. Secondly, injured patients and families place much value on opportunities to tell their stories and to be heard. Thirdly, apologies should be sincere and culturally appropriate, and not used as a replacement for other remedies. Finally, safety efforts should be undertaken and then communicated to patients and families.
Some of the NZ injured patients’ and families’ experiences were consistent with the treatment injury challenges that were outlined in the previous section of this article. Causation, for example, was frequently mentioned by participants as a troubling threshold that created difficulties in obtaining cover and/or prevented them from securing compensation. An oft-cited issue was section 32(2)(a) of the Accident Compensation Act that states that treatment injury does not include injury that is ‘wholly or substantially caused by a person's underlying health condition.’ One injured patient participant was excluded from cover and compensation because the ACC determined that his injury was ‘caused’ by his underlying health condition. Case vignette 1 summarises his experience.
Case vignette 1
Negligence is not suited to identifying systems-level causes and, thus, causation often involves identifying a practitioner who is at fault. These legal assumptions are inconsistent with learnings from medicine and other disciplines that demonstrate that many accidents and injuries are ‘caused’ by multiple factors, some of which come from systems failures.35 For all these reasons, and because causation does not fit with the underlying values of no-fault, many commentators have argued that causation should be removed from the ACC legislation. The operation of these causation tests in the current NZ ACC legislation complicates and slows the ACC process, thus undermining the core values and purposes of the ACC scheme.
In his 2022 review of the ACC, specialist ACC lawyer, Warren Forster, identified numerous problems within the system, such as the causation tests.36 With reference to the original 1967 values proposed for the ACC system, Forster outlined a vision for enabling those values in NZ in the near future. The stories in Forster's report highlight that injured people ‘want a person-directed integrated system for all people with impairments’.36 Likewise, a common refrain from participants in our research was that the ACC system should ‘return to the first principles of the ACC scheme. If we did that, it'd be fantastic. On paper, in its fundamentals, the system is about as good as you can get.’
Despite the current limitations of treatment injury, our research participants highlighted aspects of the regime that they valued. Specifically, injured patients and families valued five aspects of ACC treatment injury. First, the ACC process is low cost. Second, it is accessible because patients are able to complete a simple document themselves or have their health practitioner do it for them. Third, the ACC's decisions about cover are efficient; participants appreciated this efficiency even when their claims were declined. As one participant explained, ‘at least we do not have the stress of waiting forever for decisions.’ Fourth, patients and families value the ACC's efforts to gather data about patterns to facilitate patient-safety learning and prevent recurrences. Finally, participants reported that they value the possibility of ongoing trust and communication between patient and provider, even during the ACC processes.
One research participant (who had experienced medical malpractice in Australia before relocating to NZ to experience the treatment injury process) provided useful insights. Her initial claim was denied by the ACC due to causation issues. However, upon review, her claim for treatment injury was upheld. Despite the additional hurdle required to obtain compensation and rehabilitation, her opinion was that: ‘the NZ system is still superior. My father, to this day, has never got anything positive from suing in the court for the errors that his doctor made. He went through all that stress. It cost a fortune. It took years. His doctor wasn't allowed to talk to him or apologise because of the court case. And dad got nothing at the end. By comparison, my journey through ACC was ... less stressful, less costly and I managed to get some support in the end.’
Evaluation
There are several oft-cited fears about replacing medical negligence with an alternative, such as a no-fault compensation scheme. The main fears are accountability, costs and deterrence.
Introduction of an administrative no-fault scheme does not mean that health providers involved in harm events cannot be held accountable, or that they ‘get away with harming patients’. Instead, the NZ system separates compensation from accountability. An injured patient applies to the ACC for compensation and rehabilitation. If that patient is also concerned with accountability, they may file a complaint with the NZ health and disability commissioner. There are several remedies available, such as communication (eg an apology), restoration and correction (eg patient-safety learning). It is also open to the commissioner to refer the complaint to the director of prosecutions, who can escalate to disciplinary proceedings or civil proceedings in a Human Rights Review Tribunal.37 Furthermore, section 284 of the Accident Compensation Act 2001 requires the ACC to report certain medical injuries to the ‘authority responsible for patient safety’.25
In the UK, referrals to disciplinary proceedings as an alternative remedy for accountability would need careful consideration because of the allegations of racial bias in these processes; for example, research found that ‘doctors from ethnic minorities are twice as likely to be referred to the [General Medical Council] by their employers for fitness to practise concerns than White doctors, and the referral rate for doctors qualifying outside of the UK is three times higher than that for UK doctors.’38 Another common refrain is that the cost of administrative no-fault schemes is unsustainable and that they are more expensive than medical negligence. A significant advantage of a no-fault scheme is that claims are made to the ACC (rather than via the courts) and, thus, can be made and processed efficiently. Commentators’ conclusions about the costs of the scheme vary; for example, in an article about treatment injury published in 2011, Prof Todd argued that:
The costs of administering the scheme are relatively low and have remained stable over the last five years ... Comparisons with the costs of litigation are revealing. An estimate of the cost of tort litigation in the UK concluded that about fifty-five pence of the insurance pound was paid out to injured victims, and about forty-five pence was swallowed up in administration ... at least some of the increase [in costs of the ACC] is due to widening provisions for cover and entitlements.’28
According to ACC data, in 2021, new claims cost the ACC approximately NZD ($)1.5 billion.39 Ongoing claims from previous years cost an additional $3 billion. The ACC paid the following amounts in 2021:
$391 million towards the cost of elective surgery claims
$92 million to cover the cost of accidental death benefit claims
$634 million towards the cost of emergency hospital care
$1.8 billion to financially support New Zealanders who were unable to work due to their injuries.
In his 2022 report about the ACC, Forster estimated that the costs of administering the ACC system range between $500 million to $700 million per year.36 In 2008, PricewaterhouseCoopers undertook an economic analysis of fault and no-fault schemes in several international jurisdictions. In their conclusion, the authors summarise the evidence on costs:
There is no clear evidence that fault, no fault or blended schemes are, overall, more expensive than the other scheme types in aggregate, but we note that more people are compensated under no fault schemes, hence the per claimant cost is overall cheaper under no fault schemes. Where schemes allow common law access, tight controls need to be maintained on the common law system to ensure that scheme costs remain in check.
No fault schemes come out ahead on this evaluation, with a higher portion of claimants covered, a higher portion of scheme cost going to claimants, better claimant outcomes, a more equitable distribution of claimant outcomes and a similar level of scheme costs, average benefits and prevention effects. This needs to be weighed up against potentially less equitable allocation of scheme costs and the freedom of people to pursue tort law remedies in response to their injuries and grievances.40
In terms of the underlying values in the different systems, if a country places high value on injured patients’ needs, the evidence suggests that no-fault schemes are preferable because more injured people are compensated and there are better outcomes for the injured.
Another common critique of no-fault schemes is that they remove deterrents to injury-producing conduct and that this operates as a disincentive to safety. There are two main counter-arguments to this critique. First, there is very little, and weak, evidence that medical negligence, and torts overall, has a deterrent effect.41 Therefore, if one's core value is deterrence, arguing that a fault scheme should not be replaced by no-fault is not compelling because there is little evidence that fault schemes have a deterrent impact. In relation to medical injuries, the Harvard Medical Practice study did not find any evidence that medical injuries were reduced by litigation.7
Second, for medical injuries, there is strong evidence that medical malpractice has deleterious impacts. Health providers, for example, engage in defensive practises and may over-service because of the risk of civil liability.42 As outlined earlier in this section, there are alternative systems for holding practitioners accountable for their conduct.
This analysis suggests that the fears and critiques of no-fault may be based on misunderstandings about the operation of fault and no-fault schemes. Despite highlighting the limitations of the current NZ statutory formulation of treatment injury, my view is that the evidence, nevertheless, suggests that no-fault schemes are preferable to medical negligence. The evidence demonstrates that no-fault is better able to meet patients' needs. Therefore, if we wish to reform a system so that it values patients' needs, a no-fault system is better able to facilitate that aim. Another alternative to medical malpractice litigation, which also values patients’ needs, is the CRP.
Lessons from CRPs in the USA
CRPs: purpose, process and values
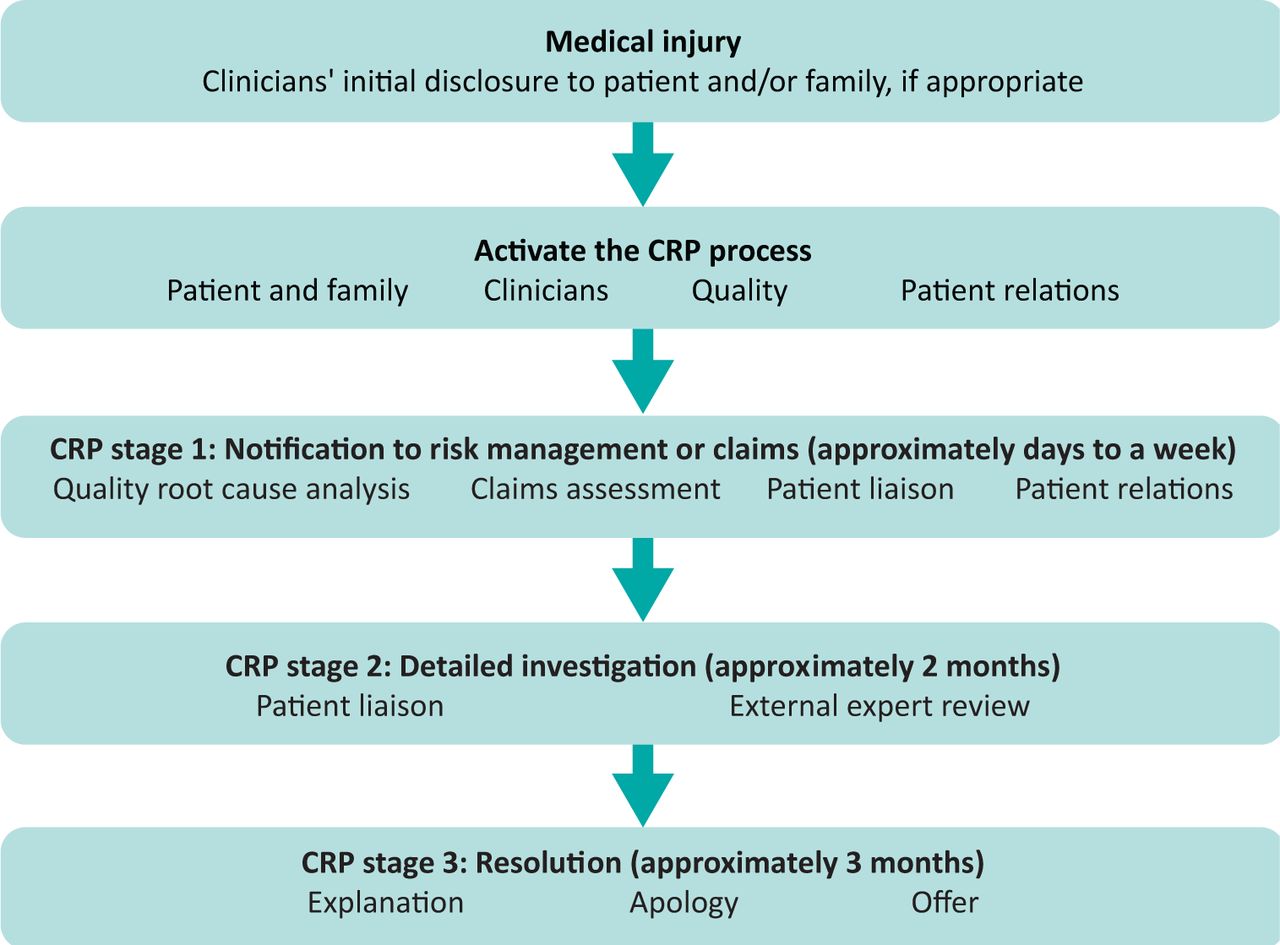
The well-documented shortcomings of medical malpractice litigation prompted US hospitals and policymakers to explore alternative systems for resolving medical injuries before injured patients and families file civil claims. In the USA, CRPs are an alternative to medical malpractice litigation in which hospitals disclose medical injuries, investigate, explain what happened, apologise and, sometimes, offer compensation to injured patients and families. Fig 1 describes the CRP process.
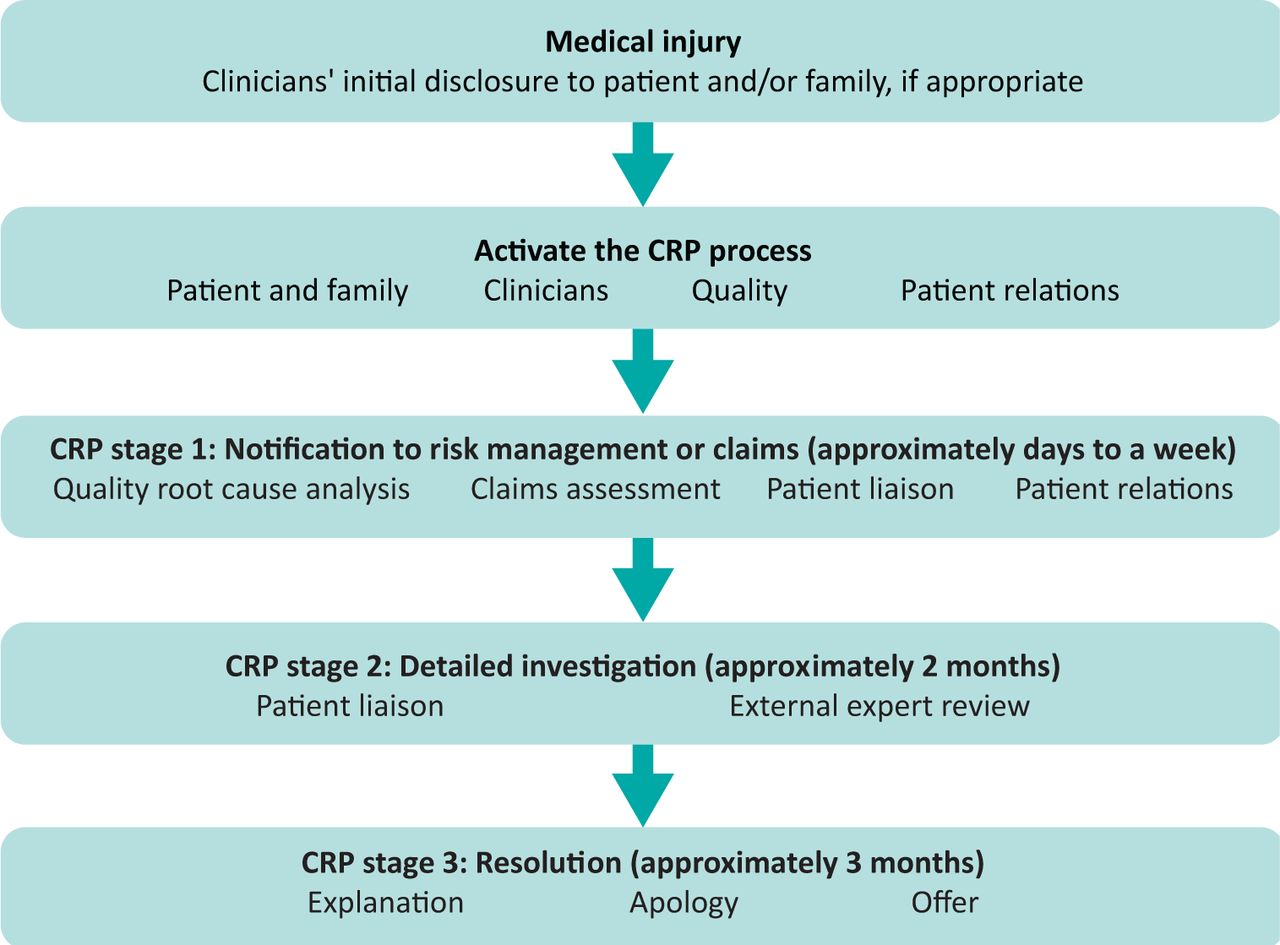
The communication-and-resolution programme process. CRP = communication-and-resolution programme.
CRPs have not replaced torts. CRPs operate within a small number of healthcare organisations; however, the US Agency for Healthcare Research and Quality is disseminating the CRP model. CRPs are touted as improving patient safety and reducing liability costs.43 These programmes value patient-centred care, patient safety and patients' needs.
Lessons from patients and providers
In our US research with injured patients, families, providers and CRP administrators, we explored the aspects of institutional responses to harm events that facilitated and impeded resolution.8 The findings highlighted what injured patients and families value about institutional responses to harm events. Specifically, injured patients and family members reported that they value:
compassionate, empathetic and non-adversarial communications throughout the process
discussions about compensation that are equally compassionate, empathetic and non-adversarial
opportunities to tell their stories and to be heard
patient-safety efforts and institutions that communicate those efforts to them
the involvement of lawyers (who are familiar with CRPs)
the efficiency of the process
the atmosphere of ongoing communication and interest in meeting their needs
the ability of the process to heal broken trust between provider and patient
opportunities to continue to receive care from the providers involved in the harm event when trust was restored because of the CRP.
The participants’ accounts highlight the pivotal place of compassion throughout ‘resolution’ processes. This need is consistent with normative scholarship on the power of compassion. Nussbaum, for example, argues that compassion is the foundational or ‘basic human emotion’.44 Other values stem from compassion. It is not surprising, therefore, that injured patients and families reported that they also wanted negotiations about compensation to be infused with compassion. Patients and families reported that they felt dissatisfied with ‘resolution’ when institutions communicated with adversarial and hostile tones, failed to communicate patient-safety efforts to them, and offered compensation too slowly.
Providers and administrators involved in the CRPs reported that they valued the system because it supports and values disclosure and apology. By contrast, medical malpractice discourages these communications. Research on the ‘second victim’ phenomenon (whereby practitioners feel distraught following medical injuries) has demonstrated that practitioners believe disclosure is the right thing to do, but they are unable to disclose because of liability concerns in negligence claims.45 Thus, when the system supports and values disclosure (as in administrative compensation schemes or CRPs), this approach will be in alignment with values held by many healthcare practitioners.
Evaluation
The points raised about deterrence in the evaluation of NZ's ACC are equally applicable here. There is little evidence that US medical malpractice litigation deters negligence. There is strong evidence that the threat of litigation increases healthcare costs by prompting defensive medicine.46 There is also evidence that the threat of legal action discourages doctors from reporting medical injuries.47 As mentioned earlier in this section, advocates of CRPs note that these programmes are cost effective; for example, Stanford University's CRP has reportedly saved $3.2 million in annual premiums since its establishment.48 Importantly, advocates of CRPs note that the cost savings are not the most important benefit of the programmes. Valuing patient voice, improving quality and safety, and meeting patients' needs are enabled in these programmes.
Conclusion
England's current review of clinical negligence, and consideration of alternatives such as no-fault compensation, should be welcomed. Valuing what patients and families want, and need, after harm in healthcare necessitates a system that enables their needs to be met. As outlined herein, medical negligence litigation is misaligned with patients' needs after harm events. By contrast, alternatives such as no-fault and CRPs offer opportunities to place patients', families' and providers' values at the forefront of resolution efforts.
Historically, Australia has considered the possibility of introducing no-fault compensation. In 1973, for example, the Whitlam government established a committee of inquiry into a National Rehabilitation and Compensation Scheme for Personal Injury. This committee was chaired by Justice Woodhouse, who had also chaired the 1960s royal commission into personal injury in NZ, which led to the establishment of NZ's no-fault compensation scheme. The Australian Woodhouse committee recommended the introduction of a no-fault scheme in Australia. However, all Australian states and territories rejected this recommendation. Many commentators have lamented Australia's approach and there are increasing calls for re-consideration of an overhaul of torts.49
One reason for the discontent is that when one asks, ‘Does medical malpractice fulfil its purposes?’ the answer is a resounding ‘No.’ Assuming policymakers, patients and providers value patient-centred care, honesty, integrity, transparency, communication, trust, and meeting the needs of patients and providers after medical injury, then the ACC or CRP approaches are much better able to fulfil those values than medical malpractice litigation.
England's current review of clinical negligence presents a timely and valuable opportunity to introduce an alternative dispute resolution system to address patients' needs and values after medical injuries. England would need to make challenging decisions about the parameters of the scheme. However, there are also exciting opportunities to design a system for responding to medical injuries that improves on the pitfalls identified herein that exist in treatment injury in NZ. In a climate where quality and safety, patient-centred care, and compassion in healthcare have been heralded as important values in the health sector, shifting away from a system (negligence litigaton) that is misaligned with those values, appears to be appropriate and much-needed.50 No-fault and CRPs have an evidenced ability to facilitate core values in healthcare (such as patient-centred care), while also meeting the values and needs of injured patients, their families and healthcare providers.
- © Royal College of Physicians 2022. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.