
ABSTRACT
Background The Royal Berkshire NHS Foundation Trust outpatient services transformation programme is a strategic change programme delivered as a collaborative approach through the Berkshire West Integrated Care Partnership. The main aim of redesign is to improve capacity in clinics and improve patient experience.
Methods This was done through a best practice menu and ‘how to’ guides. This simplified and standardised the process for moving activity from face-to-face to virtual, maximising remote monitoring and moving clinics off the main acute site.
Results We have successfully implemented six different work streams to transform outpatient services. Referrals are now triaged and streamed. The number of patients reviewed virtually, on patient-initiated follow-up and seen closer to home has increased.
Conclusion The outpatient services transformation programme has resulted in improvements within the trust and the integrated care partnership. This programme supports the vision by the Royal College of Physicians and NHS England to modernise and transform outpatient services.
Introduction
The Royal Berkshire NHS Foundation Trust (RBFT) provided around 550,000 outpatient attendances annually in 2016/2017 in a multi-site model including the Royal Berkshire Hospital (RBH), Bracknell Healthspace, Townlands Memorial Hospital and West Berkshire Community Hospital. The majority of outpatient attendances were at the main RBH site in Reading. This contributed to increased traffic, congestion and oversubscription to car parking. It also resulted in lack of space to develop new services and facilities on the RBH site. The problems faced by RBFT outpatients were not unique. The Royal College of Physicians' (RCP's) report on outpatients of the future states that this traditional model of outpatient care is no longer fit for purpose.1 The NHS long term plan aims to reduce up to a third of the face-to-face appointments delivered by outpatient services by the use of technology and giving patients greater control of their appointments.2
Aims
In 2017, the RBFT developed its outpatient services transformation programme (OTP), which set the long-term goal of improving care, developing clinical services and increasing convenience for patients attending outpatient clinics. This was part of the ambition to redesign our estate and work in collaboration with partners in the Berkshire West Integrated Care Partnership (BWICP): for patients, it provided a choice of the location, type and time of appointments; for referrers, it allowed easier and more convenient access to advice and assessments; for the provider (RBFT), there was increased efficiency and reduced congestion on the main RBH site; and, for the system (BWICP), they had closer integration and seamless working across providers.
Outpatient services transformation work streams
We developed multiple work streams that were technology enabled and provided digital solutions to transform outpatient clinics.
Referral streaming, and advice and guidance
Referral streaming is a method to influence and control patient referrals, predominantly those from general practitioners (GPs), in order to facilitate an improved flow of patients and information.
Patient-initiated follow-up
Patient-initiated follow-up (PIFU) allows the patient to decide when they will receive their follow-up appointment, rather than automatically being booked in at regular time intervals (eg every 6 months).
Virtual consultations
Patients are able to have a video consultation without the need to travel into hospital while maintaining the ability to see their clinician on the screen.
Care closer to home
The OTP actively encouraged all specialities to increase their clinic activity across all our sites to support the care closer to home model and reduce congestion on the RBH site.
Remote monitoring
Remote monitoring uses information technology (IT) software packages designed for disease or medication management, which aids healthcare professionals in monitoring long-term conditions.
Improving operational delivery
This involves work to improve efficiency and management of outpatients.
Methods
Starting in 2017 by mapping patient's journeys, we completed over 400 patient questionnaires and staff surveys. From this, a comprehensive scoping document was developed and the OTP designed (Box 1). We developed a best practice menu for all specialties to implement the different work streams. The content of the six work streams and specialties involved are shown in Table 1.
Outpatient services transformation programme work streams (2017–2021)
Outpatient services transformation programme design principles
Referral streaming, and advice and guidance
Streaming of GP referrals were done on the electronic referral system (eRS). Referral triage via eRS was mandated in quarter 3 of 2018/2019. Pathways for referrals and management of conditions were co-produced on the eRS with GPs. Referrals were triaged to ensure that advice was given promptly to referrers and appointments were booked if clinically necessary.
PIFU
PIFU pathways were used for patients of any age, provided the patient and their clinician agreed that it was right for them. The ‘how to’ guide for PIFU is shown Fig 1. The standard operating procedure (SOP) for patients suitable for PIFU is also shown in Box 2. Since January 2021, RBFT had been actively taking part in the NHS England (NHSE) south-east regional PIFU meetings to share learning and ideas with other trusts that are implementing the pathway. We are also actively involved in the development of a national reporting dashboard. From October 2021, we started reporting on progress as per the latest guidance on elective recovery.3 Patient information leaflets and contact numbers for advice were provided for patients on PIFU.
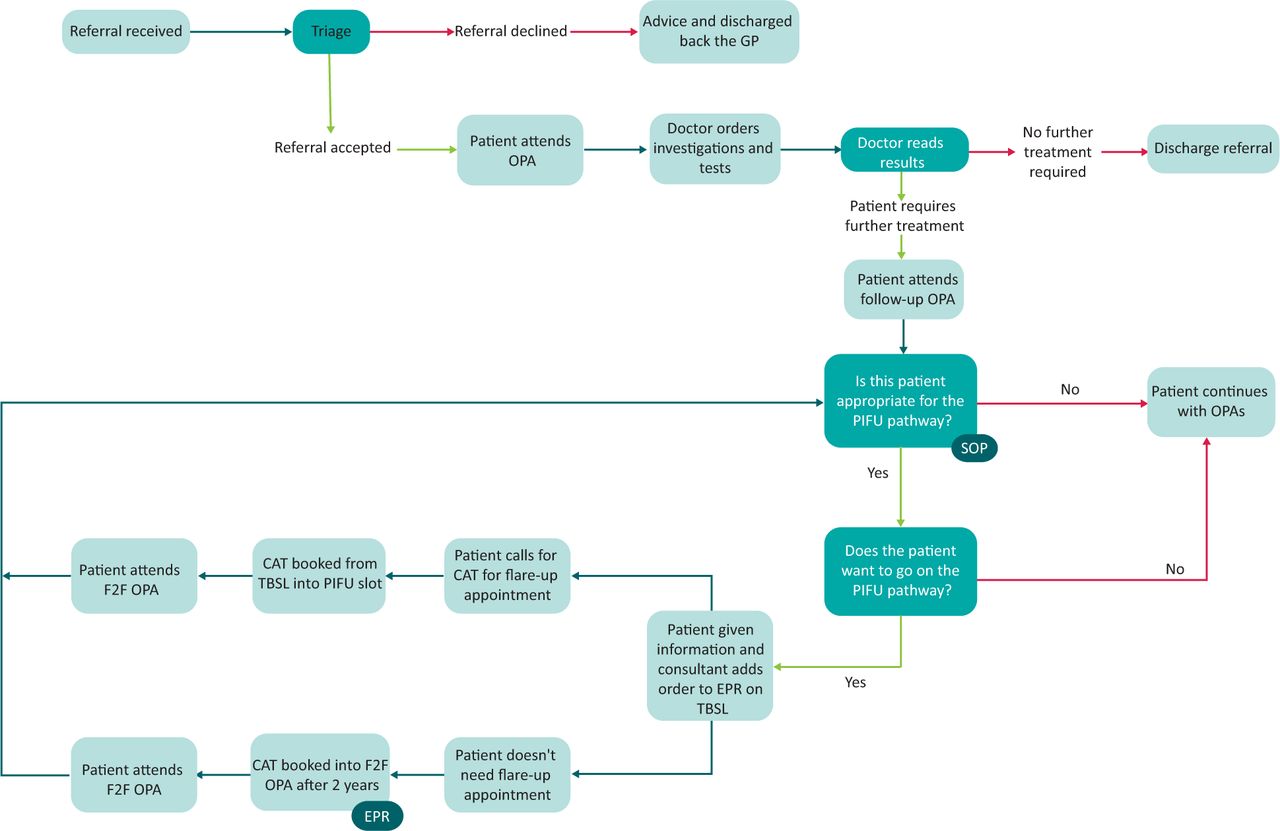
The pathway for patient-initiated follow-up. The start of the pathway (pre-PIFU) may differ between specialties. The outcome may be that the patient will receive a standard safety net appointment in the future or is discharged if they did not initiate their own follow-up within a set timescale. CAT = clinical administrative team; EPR = electronic patient record; F2F = face-to-face; GP = general practitioner; OPA = outpatient appointment; SOP = standard operating procedure; TBSL = to be scheduled list.
Standard operating procedure for patients suitable for patient-initiated follow-up
Virtual consultations
In June 2019, RBFT joined the NHSE and NHS Improvement (NHSI) video consultation pilot, trialling the use of video consultations in outpatient settings, using the Attend Anywhere platform. Training was provided for staff using this platform. Computer screens with integrated cameras were placed in various locations in the trust. Laptops with built in cameras and integrated headsets were also provided for clinicians to conduct virtual consultations from any secure location.
Care closer to home
A comprehensive analysis of where patients lived and the closest location at which they could be seen was carried out in 2017. Using the multi-site model of care, utilisation was measured across all sites. Resources were shifted or increased to promote care in a location that was closer to home for the patient.
Remote monitoring
IT software systems were integrated with the hospital electronic patient record (EPR) for remote monitoring of patients. Blood results were automatically entered on the system after a patient had their regular blood test taken. Members of the specialty team checked the system daily. The clinical team set the parameters and any blood results outside this range were flagged by the system. The patient and their GP were then contacted, eg to advise if any change in treatment was necessary without the need for an outpatient appointment.
Improving operational delivery
We systematically reviewed the skill mix and performance of staff against the criteria articulated in the RBFT SOPs. We developed a room-booking tool within our patient administration system (PAS). We have participated in the submission of the NHS benchmarking data from 2017–2020.
The best practice menu for the OTP and its contents are in supplementary material S1, Table S1. This was supported by a series of ‘how to’ guides and a communications plan. These guides were adapted to the specialty requirements and used a customised approach to speed up its implementation.
Results
There was an increased uptake across all work streams during this period. The percentage change in specialties (from 20 specialties) implementing the various different work streams from 2016/2017 to 2020/2021 are shown in supplementary material S1, Fig S1. While outpatient transformation occurred in all 20 specialties in referral streaming, there were some specialties where the other work streams (eg PIFU or virtual consultations) did not result in any significant transformation. This is highlighted in the relevant work stream sections. The benefits of the OTP are shown in Table 1.
Referral streaming, and advice and guidance
From January 2017 to March 2017, an average of 43% of referrals received were triaged (Fig 2). For the same period in 2021, this increased to 92% of the referrals received via eRS. Of these referrals, 80% were accepted and 20% were returned to the referrer with advice on the management of the patient; for example, in the first 4 months (April 2018 to July 2018) of implementation of referral streaming in two specialties (dermatology and cardiology), 17%–23% of referrals were returned with advice without a need for a clinic appointment. There was no substantial increase in staffing of consultants, physician associates or specialist nurses in these specialties during this period.
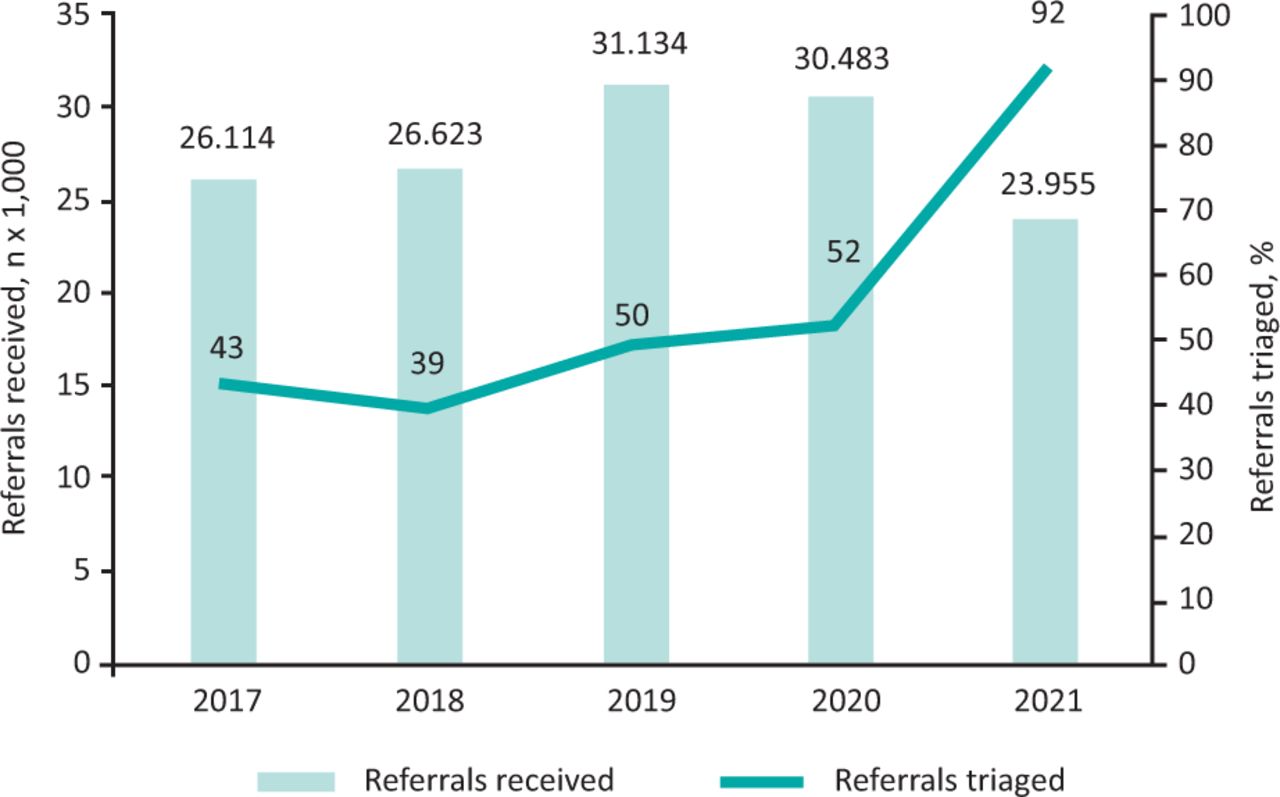
Triage and streaming of outpatient referrals for the fourth quarter (Q4; ie the last 3 months of a financial year) per year.
PIFU
Since 2017, we implemented PIFU in a number of specialties and this resulted in 3.2% of total attendances on a PIFU pathway by the end of July 2021 (see supplementary material S1, Fig S2). The implementation of PIFU resulted in a projected saving of up to 15,000 follow-up appointments per year. This calculation was based on using the total number of follow-ups delivered in 2019/2020 and 5% of these patients moving onto a PIFU pathway. From this, one in four patients would be offered a safety net appointment and those one in four patients would initiate their follow-up prior to discharge. As an example, in rheumatology, the number of PIFU patients had increased from 50 in August 2018 to 620 in January 2021. Before PIFU, patients waited up to 12 weeks for an appointment, whereas now they are reviewed within 5 days after calling the service. The waiting time for a new appointment went from an average of 43.3 days in January 2018 to 30.7 days in January 2021. PIFU was also implemented in other specialties such as dermatology; ear, nose and throat (ENT); and pain management. In April 2021, the percentage of PIFU patients on the list divided by the number of booked follow-ups in the future for dermatology, ENT and pain management was between 24%–37%. In some specialties (eg ophthalmology, urology and cardiology), transformation through PIFU did not occur in the 2017 to 2021 period. The percentage of PIFU patients in these specialties were less than 0.3%. We developed a harm-or-risk register through our governance system for any events or incidents that may have caused detriment to patient care with PIFU. Reporting systems (eg Datix) allows for reporting of events that were reviewed in clinical governance meetings. The outpatient services operational team constantly reviewed and updated the register. There was provision of information on self-management and education on their condition to empower patients on PIFU.
Virtual consultations
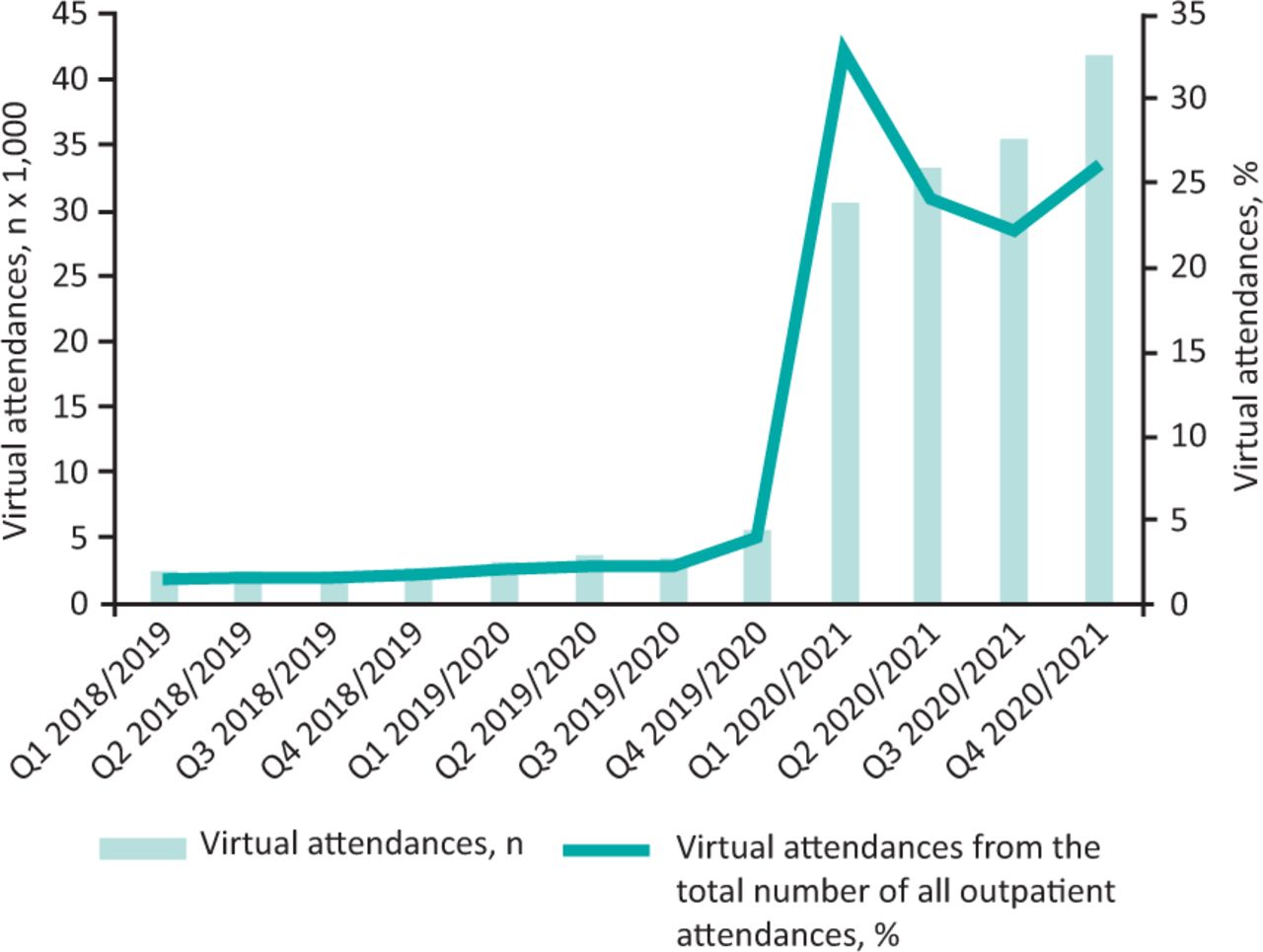
Virtual clinics started in 2017 and there was a 3.4% use in the first year. As we were rolling out the video consultations, we suddenly faced the outbreak of COVID-19 in early 2020. The digital readiness of our outpatient service accelerated the deployment of equipment and software to ensure patients could still have their reviews virtually in the midst of the COVID-19 pandemic.4 All specialties conducted virtual clinics. During the first wave of COVID-19 in April 2020, 36% of the clinics were done virtually. In the second phase in January 2021, virtual activity sat at 28%. There was a growth in virtual activity from 7% in 2019/2020 to 28% in 2020/2021 (Fig 3). In some specialties, there was a lower uptake of transformation through use of virtual consultations; for example, in ophthalmology and cardiology, the use of virtual consultations only rose from 0% in both specialties in 2017 to 8.9% and 12.8%, respectively, in 2021.
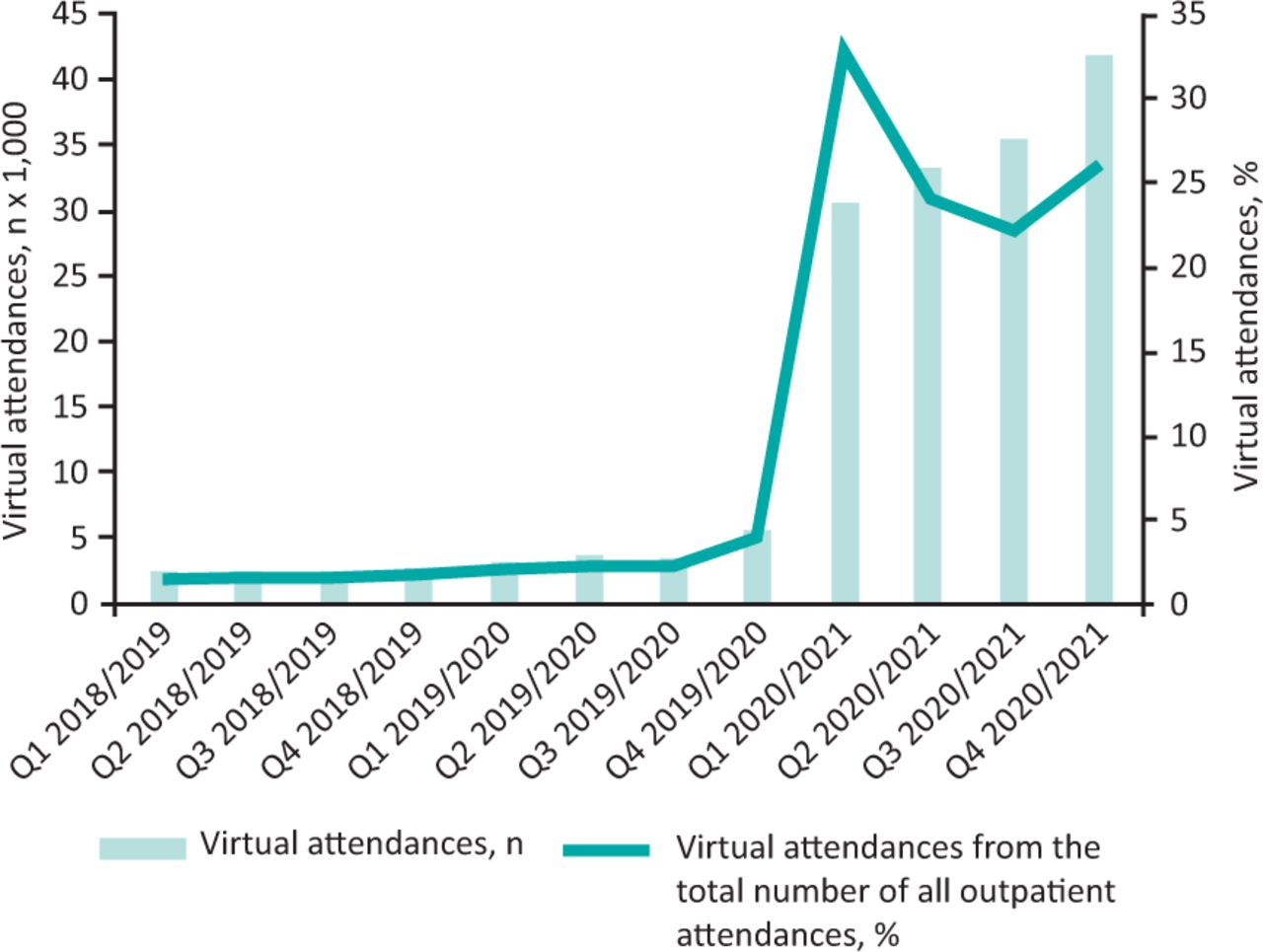
Virtual attendances for period 2019 to 2021 (separated into financial quarters).
Care closer to home
In 2016/2017, 17% attendances were conducted in sites outside the RBH. In 2019, a substantial relocation of services to Townlands Memorial Hospital reduced our footfall at RBH by a further 3% in attendances resulting in 20% of clinic attendances done off the RBH site. The rooms freed up in the outpatient area of the RBH were used to accommodate the acute emergency care ambulatory unit (AECU).
Remote monitoring
From 2016/2017 to 2020/2021, there was a three-fold increase in patients on remote monitoring and freeing up an average of 6,000 follow-up appointment slots a year. Remote monitoring was most beneficial for specialties with patients on long-term medication that required regular review such as haematology, anti-coagulation, gastroenterology and rheumatology. As a result of remote monitoring, the cost of checking results manually was reduced. Through automation, there was saving of up to 6 hours of clinician time a day. This includes time saving for the band 6/7 specialist nurses, specialist registrars and consultants. The anti-coagulation team reduced did not attend (DNA) appointments for blood testing through use of remote monitoring with automated alerting and reminder letters. Since its implementation, there was a six-fold reduction in DNA rates between 2016 and 2019, shown in supplementary material S1, Fig S3.
Improving operational efficiency
The completed skill mix review for outpatients staffing allowed budgets to be moved between departments to offer a more equitable service. The appointment of a central outpatient services manager from January 2021 strengthened the overall management with a focus on room utilisation and performance reporting. The room-booking tool provided room utilisation information to enable the optimum level of asset and resource management as well as room requirement information for use in the future planning and development of our estates.
Patient engagement
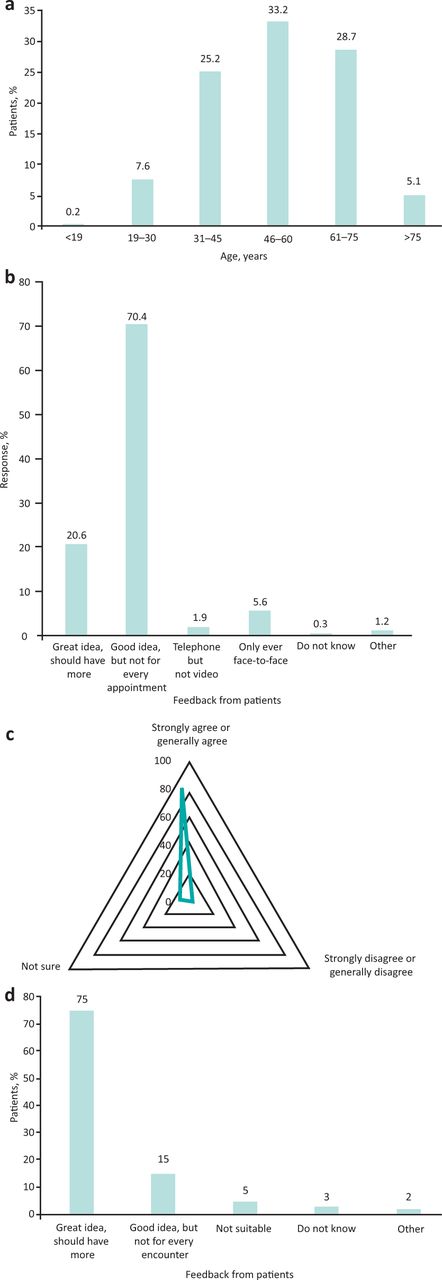
In October 2020, we conducted a survey to measure patient satisfaction of their outpatient attendance. We received 500 responses to the survey (Fig 4a–c). The female:male ratio was 7:3 and focused on adults. The demographics of those responding to the survey were reflective of the population. The majority of patients were supportive of having virtual clinics with 91% of 500 respondents grading it as good to great. However, they were also clear that this was not suitable for every appointment. Patients were also supportive of PIFU with 90% of 105 respondents grading it as good to great (Fig 4d); for illustration, please see this quote from a patient who was on the PIFU pathway:
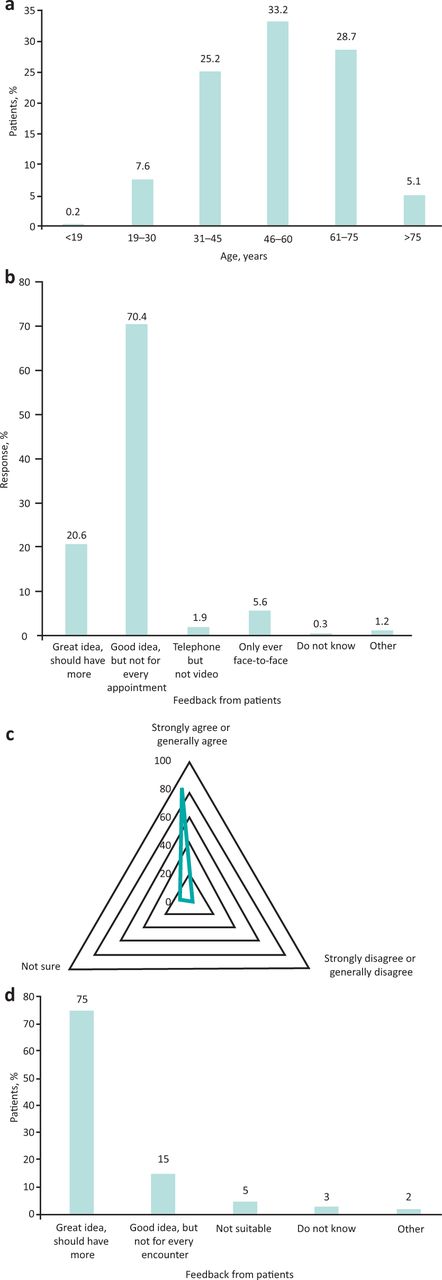
Response from the patient survey in October 2020. a) Age distribution of 500 patients completing the outpatient survey. b) Feedback from patients on virtual clinics. c) Feedback from patients on having appointments outside the main acute hospital site. d) Feedback from 105 patients on their experience of patient-initiated follow-up (PIFU).
I am very pleased with the follow-up care. It works really well, and I am able to just email or make contact when I need to be seen and the appointment is [then] sorted very quickly. This makes much more sense than been sent through 6-monthly or yearly appointments direct from the hospital. It means I get seen when I feel I need to be seen. The appointment is much more useful and also means it's not wasting clinicians' and also my time with journeys to and from the hospital, which may not have been needed at the time [that] the hospital [would have] arranged it. Hopefully by arranging follow-up appointments in this way, it helps cut down on people that DNA appointments as you only make the follow-up when you actually need it.
Discussion
The number of outpatient visits in England has doubled to 94 million in the past decade, 20% of potential appointments are cancelled or reported as DNA, costs have spiralled to £8 billion per year, and appointments generate 4,700 million kg of carbon emissions.5 The RCP's 2018 paper, Outpatients: The future, recognised that transforming the model of care means ‘taking into account all the costs related to an intervention, including loss of income to a patient attending an appointment and the impact of transport on public health.’1 The recent The NHS long term plan announcement that, over the next 5 years, up to a third of face-to-face outpatient visits will be avoided, challenging us to go further on reducing clinically unnecessary activity and moving activity to virtual means.2
Our OTP redesign had a system-wide approach and the journey to implement it was positive. Additional system-wide benefits include reducing air pollution, improving service efficiencies and reducing pressure on the hospital site. There will be further benefits from freeing up car parking spaces and savings for patient journey times. The impact of the OTP best practice menu and ‘how to’ guides resulted in a reduction in waiting times for appointments; for example, in referral streaming, the improved waiting times were from transformation and not due to an increase in staffing or workforce during this period.
A key area of focus was how we identified resources released from outpatient modernisation and transformation. Resources are released from staff time in not undertaking unnecessary work and from reducing the physical footprint of outpatient services. Repurposing the resource may help support operational pressures within the system (eg supporting the non-elective pathway), for instance, in remote monitoring, the release of clinical time as well as reduction in follow-ups allowed clinicians to see new and urgent referrals in a quicker time.
The impact on the wider MDT from the OTP was upskilling and role enhancement. We have focused on staff engagement to raise awareness of the programme and the need for change. The aim was to highlight successes and provide tools to support implementation of new ways of working. Administrative staff provided system support for outpatient clinics including setting up virtual clinics, collection of pre-clinic questionnaires and follow-up activity. Nurses were able to use more telephone and remote monitoring services to manage follow-up patients supported by data from the software program. There was also role enhancement with allied health professionals (such physician associates) doing more teleclinics and remote monitoring. It was also necessary to ensure that no harm resulted from the transformation. Both clinicians and patients reported any incidents, and we developed a harm register in order to prioritise safety and quality of the service.
The COVID-19 pandemic tested the OTP, in particular, virtual clinics were accelerated allowing clinician–patient interaction during the pandemic.6 Using video in this way increased convenience for the patient, reduced travel costs and minimised the need for patients to take time out of their day to attend hospital. It also reduced congestion on the acute site. In some specialties, transformation through virtual clinics did not significantly happen due to the nature of the conditions seen by these specialties where face-to-face clinical examination or investigations were essential; for example, in cardiology and ENT, transformation took place with the delivery of one-stop-shop clinics. PIFU is an integral part of the COVID-19 recovery phase and has many benefits for patient care. This includes reduction in non-value adding appointments and allowing the patient to be seen by their specialist when they need it most. NHSE and NHSI are supporting providers to roll out PIFU.7 Systematic reviews of PIFU has shown that it increases patient and clinician satisfaction as well as promotes health and service quality.8,9
Conclusion
At the core of our OTP is a comprehensive, system-wide model that identified the impact of the programme's objectives on the organisation, all outpatient sites and individual treatment functions. The model supported clinical specialties in exploring options and the scale of the opportunities to reduce waste and transform outpatient delivery. To sustain this in line with The NHS long term plan, we have implemented a total outpatient pathway system that is end-to-end and patient focused. This transformation will drive improvement in quality and effectiveness of patient care.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj:
S1 – The RBFT outpatient services transformation programme best practice menu, implementation of the outpatient work streams, patient-initiated follow-up and did not attend numbers.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}