
ABSTRACT
Aim We aimed to examine the effect of the second wave of the COVID-19 pandemic on Academic Foundation Programme (AFP) trainees.
Methods A voluntary, anonymous questionnaire was circulated to all UK AFP doctors. Data were collected from February 2021 to April 2021 then analysed.
Results Of a possible 1,096 trainees, 149 responded to the survey: 48% of respondents were at least partially redeployed, 31% lost academic time and 47% had projects cancelled or postponed. In free-text responses, despite some research opportunities, frustration at lost research time and opportunities were common themes. Trainees also highlighted communication and wellbeing issues.
Conclusion These results demonstrate that the overall effect of COVID-19 on this cohort cannot be underestimated. We propose that a series of measures are implemented to protect and support academic trainees. We hope that these measures would encourage high-quality academic output and help secure the development of the academic clinical workforce.
Introduction
As far back as 2005, the UK Clinical Research Collaboration described academic medicine as being in a ‘perilous state’.1 The Academy of Medical Sciences reported that NHS staff were increasingly under pressure and less able to partake in academic work.2 In addition, a Medical Schools Council survey showed that clinical academic workforce numbers are stagnating.3
The Academic Foundation Programme (AFP) was created in response to the 2005 UK Clinical Research Collaboration report. The AFP, now known as the Specialised Foundation Programme (SFP), gives foundation doctors in the UK the opportunity to dedicate a proportion of time to academic medicine, which allows them to develop knowledge and skills in relation to leadership, research and education.4,5 Academic time can be allocated as a 4-month rotation or split across 2 years. The AFP runs alongside the 2-year UK Foundation Programme and academic trainees account for approximately 7% of the foundation doctor workforce.6
The National Institute for Health and Care Research's (NIHR) update from March 2020 and their ‘research recovery’ update in 2021 revealed how priorities had changed rapidly.7,8 They concentrated efforts on COVID-19 research from March 2020 and advised academics to prioritise patient-facing care.7
During the first and second waves of COVID-19, there were significant disruptions to medical training and education. AFP trainees were re-tasked by the UK Foundation Programme Office (UKFPO) to support colleagues in the clinical setting.9 Craggs et al analysed the disruptions and opportunities to academic foundation training borne out of the first wave of the COVID-19 pandemic and trainee concerns were identified.10 Following this publication, there has been no collaborative response to improve the AFP trainees' experiences. Herein, we seek to further explore the effects that the COVID-19 pandemic has had on the trainees and propose solutions to the issues raised.
Material and methods
We used the same questionnaire as Craggs et al, designed during the first round of this project, to capture the experiences of AFP trainees during the COVID-19 pandemic.10 The first part of the survey collected demographic data, the second focused on redeployment and the final section explored views on the impact on academic training. The list of questions can be accessed in supplementary material S1. No questions were mandatory.
The survey was designed and distributed electronically using Google Forms. The survey was circulated to AFP trainees nationally through the local foundation schools via email. An advert was published in the UKFPO bulletin to encourage participation. Participation was voluntary and anonymous. Data were collected between February 2021 and April 2021. The survey was sent out following the peak of the ‘second wave’ of COVID-19 in the UK to capture the impact of this on AFP trainees.11 In order to increase the reliability of this data, academic foundation schools were contacted via email requesting data on academic trainees' redeployment in the second wave. A copy of the questions that were sent can be seen in supplementary material S2. Local governance permission was granted to allow analysis and publication of the survey results.
The quantitative data were analysed using descriptive statistics. Qualitative analysis was performed on the free-text answers to question 7 section 2, question 2 section 3 and question 1 section 4 (supplementary material S1).
We used phenomenology theory to guide qualitative analysis using an inductive approach.12 Through content analysis, codes were created as the text was read independently by two researchers.13 Final codes were established following comparison and discussion by both researchers. These were then applied to the text to aid interpretation. Due to the narrative nature of the analysis and limited previous research on the topic, saturation was not formally measured.
Ethics statement
We would like to clarify this piece of quality improvement work is non-interventional and only involves a survey. Ethics approval was not required, and we used the Health Research Authority algorithm to confirm this assessment. As defined by the NHS, this type of work only requires local governance permission from the host organisation; permission was granted by Health Education England.
Results
Quantitative results
A total of 149 AFP trainees completed the survey from 13 out of 15 academic foundation schools at 79 separate hospitals in the UK (supplementary material S3). Of the respondents, 74.5% were foundation year-2 (FY2) doctors and 77.9% were on research tracks (supplementary material S4). Results showed 94 (63.1%) respondents were not redeployed and 55 (36.9%) were at least ‘partially’ redeployed (supplementary material S5). Most of the cohort who were redeployed were sent to COVID-19 wards (n=24; 16.1%) followed by general medical wards (n=12; 8.1%) and intensive care units (n=7; 4.7%). A comparison on redeployment numbers in wave one versus wave two is shown in Fig 1. We outline further demographics and data relating to re-deployment in the supplementary material.
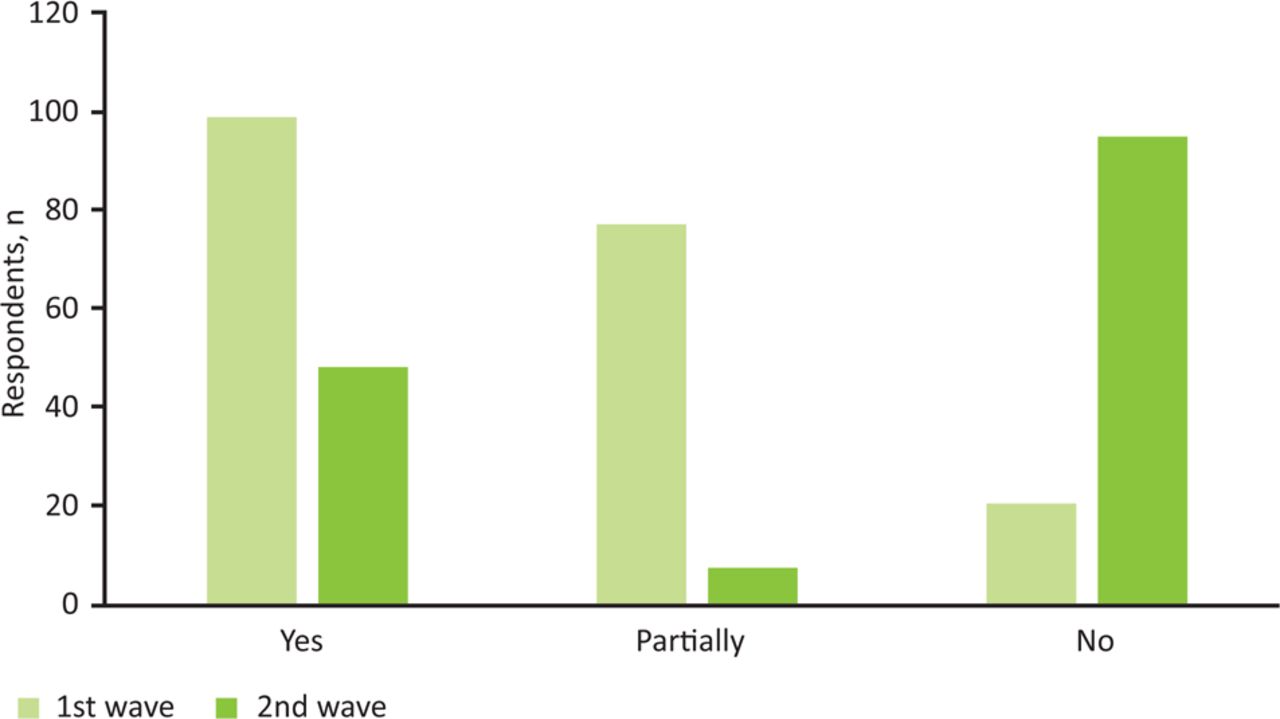
Number of respondents redeployed in 1st and 2nd COVID-19 pandemic waves.
At the time of submission, the following academic foundation schools had replied to the request for data on redeployment: North West of England, Trent (part of East Midlands), Newcastle (part of Northern), and Peninsula and Severn (both part of South West of England). They all reported that no academic trainees from their schools were redeployed in the second wave. Survey responses stated that four trainees from the North West of England school and two from Trent school were redeployed. No trainees from the Newcastle school reported redeployment and there were no responses from trainees in the Peninsula or Severn schools.
Of those who responded to the survey, 52 (34.9%) had lost academic time (Table 1). Alongside this, 68 (45.6%) respondents had their projects cancelled or postponed. A comparison between time lost in wave one to wave two is shown in Fig 2. There was a loss to education and training opportunities for 121 (81.2%) trainees. A third (n=50) of trainees reported that the pandemic resulted in positive outcomes for their academic training.
Effect of COVID-19 on academic time
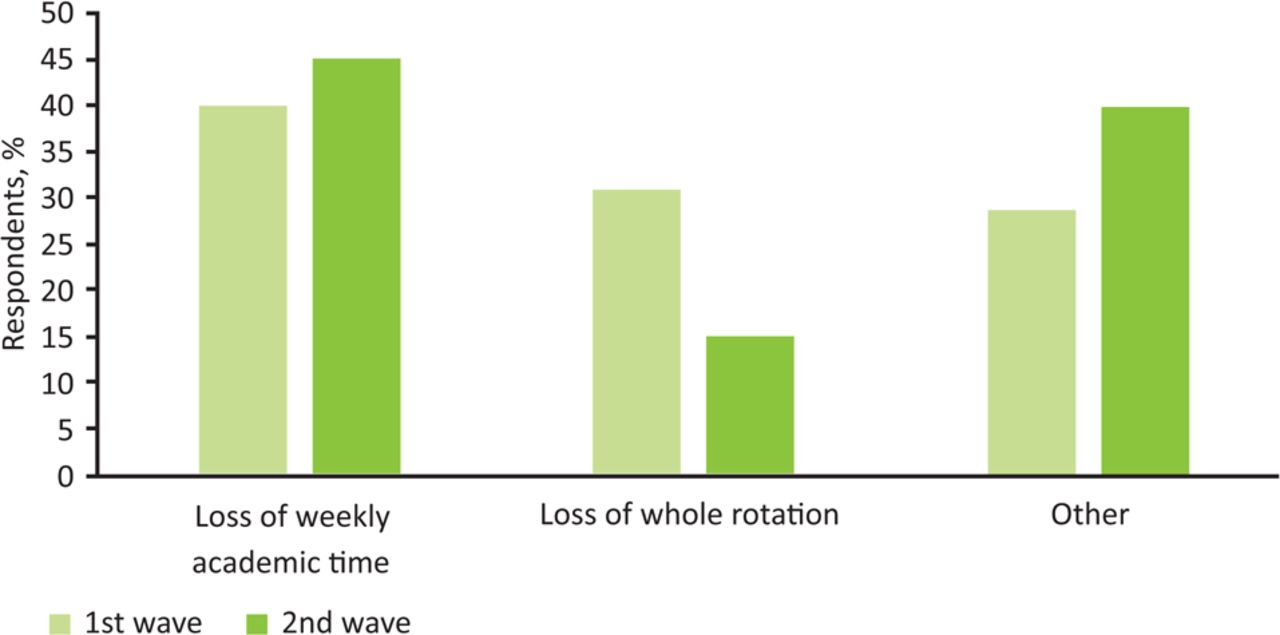
Impact of COVID-19 on academic activity during 1st and 2nd COVID-19 pandemic waves.
Positive qualitative analysis
The free-text box questions included, ‘If the answer to the above was yes, please could you detail what these positives are?’ and ‘Please feel free to use the space below to share any experiences (positive and negative) that you have had during the COVID-19 pandemic relating to your academic work.’
Two main themes emerged from the free-text answers: these were ‘accessibility’ and ‘successful academic ventures’ (Table 2), mentioned in 36 responses. However, of the 149 submissions, 103 either gave no comment or a negative answer to the questions above.
Positive qualitative themes and codes
The theme of accessibility included seven codes: flexible working and collaboration across virtual platforms were mentioned the most, with nine and seven answers, respectively. One respondent noted that there were ‘new project opportunities and the ability to have teaching, academic meetings and conferences virtually so not having to travel which adds cost and often requires more time off that cannot always be facilitated’.
Some AFP doctors carried out successful academic work, represented by five codes linked to this theme. The most common code was ‘COVID-19 research projects’, mentioned in 25 responses. The quote ‘opportunity to be involved in national trials, run teaching sessions on care for COVID patients throughout the hospital, presentations to departments on guidelines and best practice’ shows the variety of work possible for some. Five respondents discussed virtual teaching projects, alongside one reporting a journal publication.
Negative qualitative analysis
The authors analysed the results from the free-text box answers to ‘If there is anything else regarding disruption to your academic time you would like to share with us, please detail it here’ and ‘Please feel free to use the space below to share any experiences (positive and negative) that you have had during the COVID-19 pandemic relating to your academic work.’ Seventy-six responses detailed negative aspects. Free-text comments were sorted into four themes: ‘loss of opportunities’, ‘changes to planned working arrangements’, ‘organisation and communication issues’ and ‘trainee wellbeing’ (Table 3). Many trainee responses covered multiple themes, one comment read: ‘loss of all academic time, loss of academic teaching, projects put on hold. Poor communication from trust leads, not involved in the decision-making process'.
Negative qualitative themes and codes
The most common theme was ‘loss of opportunities’ with 42 related comments. Inability to conduct research in their chosen field was the most frequent issue, with 26 trainees reporting that they had to change projects or could not undertake their project.
A relatively small theme of ‘changes to planned working arrangements’ included issues in both the clinical and virtual working environments. Issues with clinical areas included staff shortages and changeable workplaces: ‘Put on the worst rotas, moving from different wards and specialties on a daily basis’. Ten trainees reported changes to working from home and virtual working as a negative, compared with similar numbers citing this as a positive aspect for improved accessibility.
The theme ‘trainee wellbeing’ emerged from 25 responses. This theme covered both the frustrations at inequity and issues with mental health. Five trainees reported that those on academic blocks were more likely to be redeployed than colleagues on other specialty rotations. A further seven trainees expressed frustration at the inequality of time lost, eg ‘overall this wave felt much less equal, academic trainees lost a huge amount of the academic time, some disproportionately to others’. Some issues raised were common to all healthcare staff (such as burnout) while some related more specifically to academic training (such as guilt associated with taking time off clinical duties). One trainee wrote: ‘I'm exhausted and burnt out, academic work feels like another hoop to jump through.’
Concerns surrounding organisation and communication were expressed by 22 trainees. These included a range of comments including a lack of awareness from rota coordinators and trust staff surrounding academic requirements.
Discussion
This evaluation provides further evidence of the disruption to AFP doctors. Our data includes responses from 13 of the 15 academic foundation schools but has a lower number of responses than the first survey.10 The lower number of respondents could represent survey fatigue as, during the COVID-19 pandemic, there have been many surveys produced and sent out to an already stretched workforce.14 This piece of work is a snapshot and further surveys would be required to ensure external validity.
The mismatch between data collected via the survey versus the results received from academic foundation schools may suggest that hospitals were not reporting all redeployments to academic leads or that schools were not requesting up-to-date data. While the majority of schools did not respond, the disparity in data indicates a need for further investigation on the way trainee data and experiences are collected by academic schools.
The quantitative data showed there was a significant reduction in the redeployment of AFP doctors, with only 55/149 (36.9%) compared with 161/196 (82%) redeployed in the first wave (supplementary material S5).10 This reduction in redeployment could reflect an increased preparedness. Most were relocated to medical or COVID-19 wards (supplementary material S6), similar to the previous survey results. There was a slight reduction in disruption to teaching with 121/149 (81.2%) compared with 183/196 (93%) respondents identifying that their formal education was disrupted.10 These results indicate that foundation doctor education continued to be impacted and suggests that further preparation to safeguard the educational time of trainees is necessary.
It is important to note the impact that COVID-19 has had across academic medicine. Mourad et al discuss widespread redeployment of clinical research staff and the impact on research during the early stages of the pandemic.15 Sohrabi et al add that lockdowns affected supply chains to laboratories and research charities experienced reduced funding.16 The NIHR prioritised COVID-19 research from March 2020 to March 2021 and advised academics to focus on patient-facing care.7,8 Due to high numbers of COVID-19 cases, pressure on NHS services continued during the winter of 2020/2021.11 It is, therefore, unsurprising that the earlier results indicate ongoing disruption to AFP trainees.
The academic vice president of the Royal College of Physicians in May 2020 wrote to stakeholders to encourage them to support clinical academic trainees to return to research. He acknowledged that academic trainees had called for a flexible and individualised approach to support their academic endeavours.17 The letter stated that the NIHR and Health Education England had also released statements in support of academic trainees. A statement produced by the Academy of Medical Royal Colleges in November 2020 echoed similar views and encouraged ‘Programme Directors to accommodate, where possible, equivalent academic “time back”.’18 However, several respondents to our survey wrote about a lack of remuneration in relation to academic time. The results of this survey are disappointing in the context of the stakeholder statements mentioned. Importantly, there have been no changes to the shortlisting scoring methods for academic clinical fellowship posts to reflect the disruption that junior doctors may have experienced.19–21
Survey results from both waves show that there have been some positive outcomes from the COVID-19 pandemic. A third of trainees who responded to this survey reported that the pandemic resulted in opportunities and academic progression, despite challenging circumstances. Gottenborg et al acknowledge the benefits of flexible working, which was made almost compulsory by the pandemic.22 He et al discuss that the rise of virtual working may even help to flatten the hierarchy that is so prominent in academic medicine.23 This was reflected by our survey results, with 36 trainees discussing ‘accessibility’. This included flexible working and collaboration across virtual platforms, often meaning a reduction in costs, particularly for travel and accommodation. This flexibility should be preserved to offer more equal opportunities.
The surveys from both waves highlighted the opportunity to partake in COVID-19-related research. In wave one, 23 respondents reported this opportunity compared with 25 respondents in our survey.10 Despite significant on-going disruption, a small number of trainees were able to present or publish their work.
The mental and physical burden of the COVID-19 pandemic and the impact of this on both academic medicine and healthcare workers in general have been appreciated in the literature.24,25 Craggs et al found that 18 trainees expressed ‘guilt, anxiety and uncertainty’ in the context of their academic work.10 Similar patterns were seen in our results. Trainee wellbeing was discussed by 25 respondents in a negative context, with the most consistent issues being ‘frustration’, ‘burnout’ and ‘guilt’ associated with doing academic work during the pandemic. One trainee wrote, ‘I didn't feel able to leave the ward [to take academic time] because I felt so guilty leaving’.
Several papers have discussed the concept of ‘feeling valued’ in the context of trainee wellbeing.26,27 In our survey, there were concerns about the value placed on academic work. Some trainees found that they were met with a reluctance to allow academic time, a lack of understanding of academic trainee requirements and a failure to reinstate academic training promptly. Ologunde et al found a similar theme from free-text responses to their survey about the AFP.5 One respondent to our survey explained, ‘There is an apparent belief that AFP research is somehow less valuable than other research activity ... which was frustrating’.
The poor organisation and communication experienced by some respondents may have further negatively impacted on wellbeing. A doctor noted that a ‘lack of communications from our hospital and the dean made a tough time even worse’. Results from both our survey and Craggs et al indicate that not all trainees have felt adequately supported through the uncertainty.10 This issue is not unique to academic training: a survey of three NHS trusts found that fewer than half of trainees felt supported by hospital administration and even fewer felt supported by clinical and educational supervisors.26
Gottenborg et al cautioned that junior academics are more vulnerable to ‘negative impacts on their careers, burnout, and career longevity’.22 Arora et al argue that adjustments should be made for academics to allow for the impact of COVID-19.25 While it was recommended that academic training was reinstated, there was no national guidance on the timescale or how to redress academic opportunities that were missed.17,18 Many respondents expressed frustration on this issue, especially from those that were redeployed from academic blocks.
Conclusion
COVID-19 continues to have a significant effect on this cohort of AFP trainees. The following proposals aim to improve the wellbeing of trainees and mitigate the disadvantages that this cohort may face when applying for future academic jobs and funding. In turn, we hope that these measures would encourage high-quality academic output from the new SFP programme and help secure the development of the academic clinical workforce.
Key points
Academic foundation schools should be aware of any academic trainees that are redeployed and collect data consistently across all areas to ensure that the impact on academic training can be reliably measured.
If academic trainees are redeployed, all efforts should be made to ensure that this does not affect the entirety of a trainee's protected academic time and that a clear plan is made for remuneration.
Reinstatement of disrupted academic time should be consistent, ideally across all deaneries but certainly within them.
Any redeployments or cancellations of academic opportunities must be clearly communicated with trainees in a timely manner.
If academic time is affected, expectations of academic output must be altered to fit with this. While academic clinical fellowship scoring systems have not been adjusted for this cohort, there is still time to alter systems for their next round of applications (eg into specialist trainee-3 posts). Academic recruiters should make this a priority.
Deaneries should create clear lines of communication with trusts employing academic trainees to ensure everyone from senior doctors to administrators are aware of the academic trainee requirements and support their need to meet this. This is especially important for redeployments to areas that do not usually have academic trainees.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj:
S1 – Questionnaire used to gather survey results.
S2 – Questions sent to academic foundation schools.
S3 – Respondents and their academic foundation school location.
S4 – Respondent demographics.
S5 – The number of Academic Foundation Programme doctors redeployed.
S6 – Summary of redeployment locations.
Acknowledgements
We would like to thank the Health Education England (North West) administration team for their help in disseminating and advertising the survey. We would also like to thank all the AFP doctors who took the time to respond to the survey and all healthcare workers for their invaluable ongoing work during the COVID-19 pandemic.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.