
ABSTRACT
In the Netherlands, the physician associate/assistant (PA) was introduced in 2001. We aim to describe the characteristics of PAs in the Netherlands. Information from public resources, mainly a report on capacity needs and a survey of PAs, was aggregated to provide an overview of the Dutch PA population. Results show that 73% were women; ages between 30 and 59 years were all evenly represented; and there was a wide variety in the background, specialty and location. Overall, the demographic characteristics of the Dutch PA profession are comparable with those of other PA workforces in the world. Presently, the PA movement in the Netherlands has a solid base of central support and national policy. PAs have full practice authority, and their numbers are steadily growing. While demand will eventually level out, the ideal number or PA ratio in the healthcare workforce remains unknown.
Introduction
The physician assistant (PA; also known as physician associate in other countries) was introduced into the Netherlands in 2001.1 The main reasons were an expected shortage of physicians, and a desire to control costs and increase continuity of care, both in hospitals and outpatient clinics.1 PAs can provide this continuity because of their familiarity with the ward and patients, and from their consistent presence.2 The PA concept was modelled after the USA and adapted to fit the unique needs of the Dutch. Dutch PAs work in primary and secondary care, and perform various medical tasks. Under Dutch law, they are authorised to prescribe medication and perform predefined medical procedures without direct supervision.3 The primary motive for employing a PA in Dutch healthcare is to increase continuity and quality of care.4 As of 2021, there are five accredited PA education programmes that educate 250 PAs in total per year. The Dutch education process takes 30 months and is organised at a master's degree level. The programmes adhere to a dual work–education model: students develop their medical specialty (2 days per week) throughout the entire length of the programme; they receive education (1 day per week); and they have different clinical placements (2 days per week) covering a broad spectrum of medical disciplines (for example, paediatrics, geriatrics, acute care and surgery).5 Prerequisites are a bachelor's degree in a health profession and at least 2 years of experience in healthcare.3 Early on, the growth of the PA movement was assessed and their need forecasted.6 Presently the PA movement in the Netherlands has a solid base of central support and national policy. PAs have full practice authority, and their numbers are steadily growing and are considered a result of the collaboration between healthcare institutions, a PA association, five universities and the government. As a contribution to the global demand for medical providers, we describe the characteristics of PAs in the Netherlands.
Methods
Information from public resources was collected to provide an overview of the Dutch PA population. The main two data sources were a report on capacity needs in healthcare and a survey of PAs in 2018.6,7 The capacity report was based on data from the national Dutch PA register and several studies.6 From this report we extracted information on gender, overall number / full-time equivalent (FTE) PAs per 100,000 inhabitants, overall number/FTE PAs per 100 FTE specialist care providers and number of PAs in education. The second source was a PA survey, for which, data were collected in 2018.7 All PAs in the Netherlands were surveyed using an online questionnaire regarding their current and previous position, and expectations of future employment. The invitations and a reminder email were sent out by the five Dutch education programmes within their alumni network. A total of 460/1,207 (38%) surveys were completed. Data were weighted to extrapolate the total population of PAs in the Netherlands. The survey was anonymous and ethical approval was waived. Data were validated by a board of researchers comparing the results to previous studies and the PA register in order to provide accurate information to calculate capacity needs. From this survey report, we collected data on age distribution, demographics, profession prior to PA career, current employment, health sector and tasks.
Results
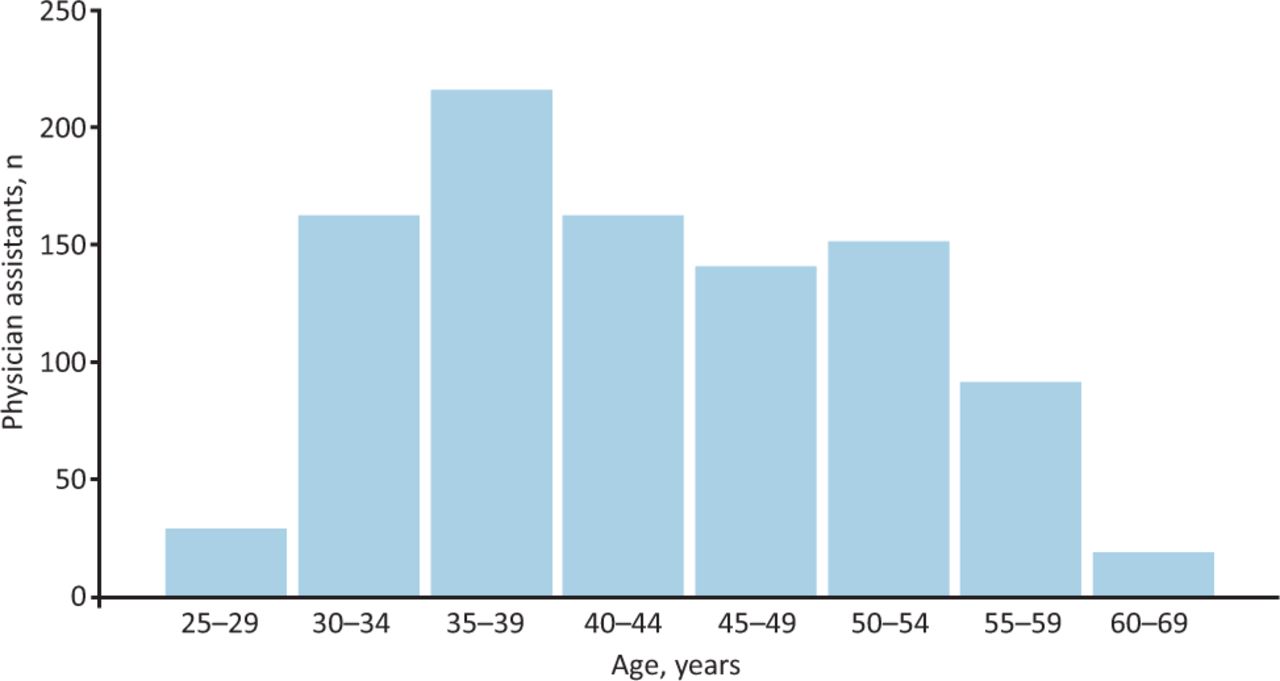
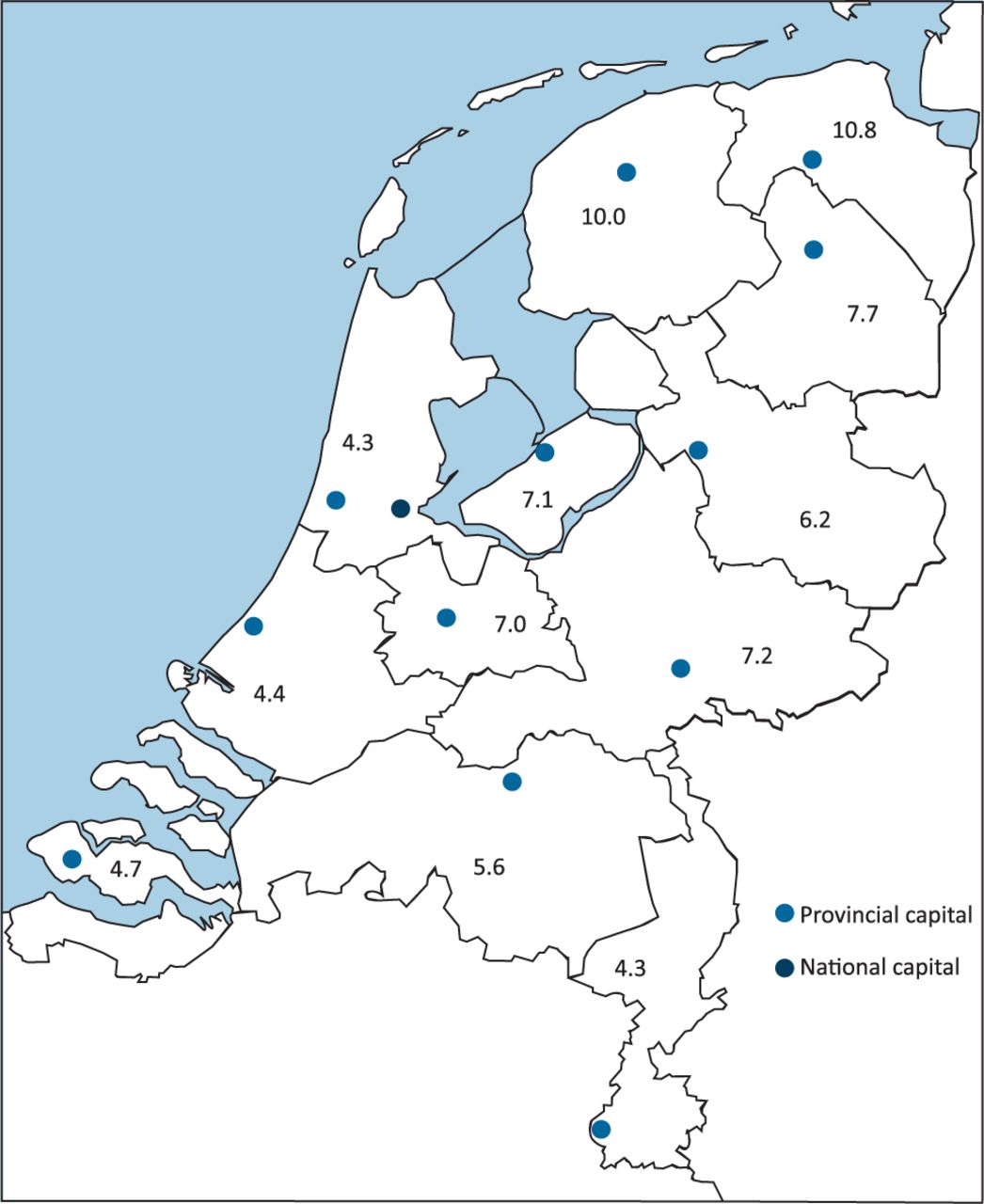
Demographic information and capacity are shown in Table 1 and Fig 1.6,7 All age groups were represented, and more than half (56%) of all PAs were between the ages of 30 and 45 years. There was a slightly higher proportion of female PA students in education between 2012 and 2019 (79.7%) than all PAs (73%). Most PAs began their health career as a nurse prior to their training to become a PA (35%), followed by allied healthcare roles (28%). The number of PAs per 100,000 inhabitants varied between the 12 provinces (Fig 2). A total of 88% of PAs were employed as a PA at the survey time. Most were employed in a hospital or a specialist care setting (Table 2).6,7 Specialist care included general surgery, obstetrics and gynaecology, and orthopaedics. The category of ‘other’ included specialties with fewer than 12 FTE PAs. In Table 2, we also report which specialty PAs in education were employed in during their training. Besides the training in their chosen specialty, they did various clinical placements to train as a generalist. These data show a relative increase in family medicine compared with the PAs that graduated before 2018.
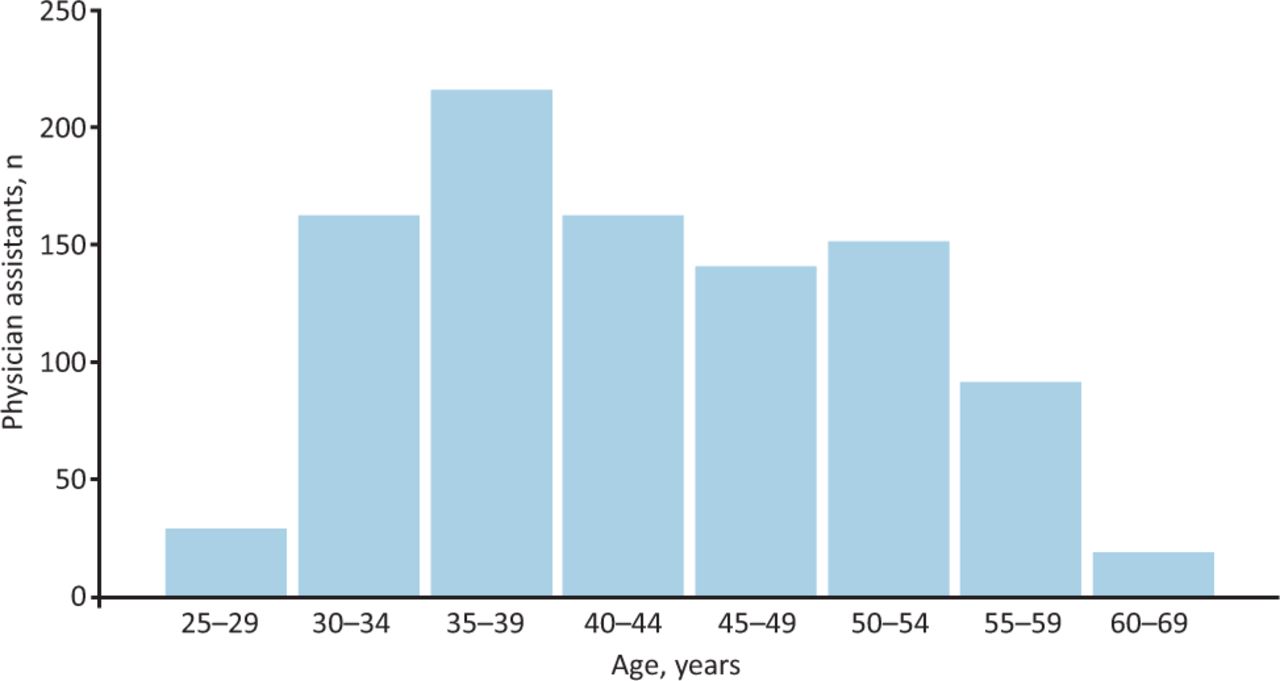
Age distribution of physician assistant population.

Map of the Netherlands with physician assistant rate per 100,000 inhabitants in each province.
Characteristics of physician assistant population
Overview of physician assistant distribution across different health sectors
The survey provided a view of tasks by PAs (Table 3). In total, 91% of all PAs perform patient consultations.7 These PAs spend half (49%) of their time interviewing and evaluating patients. Other tasks were consultations with professionals, development or innovation projects to improve healthcare services, and quality of care activities (including organisation and supervision of students). PAs spent most of their time on patient encounters, performing procedures or functioning in the role of an attending physician (eg overseeing patient care in a hospital ward). This follows previous research on PA activity analysis in Dutch hospitals.8
Tasks performed by physician assistants reported in the survey
Discussion
The data reveal that the Dutch PA profession has similar demographic characteristics to other PA populations. In the UK, the Faculty of Physician Associates (FPA) census 2020 reported that 66% were women, 22% were men and 12% were unknown.9 Whereas the population in the USA started out predominantly consisting of men, more recent data show that between 66.8% and 75% are women.10 Age distribution reported in these articles is similar to the age distribution of the Dutch population. Despite the relatively short period that the PA education programme has existed in the Netherlands, the Dutch PA workforce now spans all age categories in 2 decades. This is explained by the fact that an applicant is employed as a ‘PA in training’ when they start PA education. Often, employers select their applicants from a list of internal candidates, including older, more experienced nurses or paramedics. The programme consists of a dual work–education model. The students follow education 1 day a week, and the rest of the time is divided between their own specialty and various clinical rotations that cover the broad disciplines of medicine. This way, students develop the medical specialty they are employed in throughout the entire length of the programme next to being trained as a generalist.5
Regarding the distribution of specialties, Morgan et al report a slightly higher percentage of PAs working in primary care in the USA (23%) compared with the Netherlands (13.5%).11 However, the Dutch PA family medicine definition excludes general internal medicine, general paediatrics and geriatrics. The UK shows a similar trend in which the percentage of PAs that work in general practice has been increasing over the last decades, up to a current percentage of 30%.12,13 The percentage of PAs that work in obstetrics and gynaecology is substantially more prominent in the Dutch population compared with the USA. In the last decade, Dutch PAs have become more visible in genetics, ophthalmology and psychiatry. Straughton et al report a similar trend regarding a growing interest in the field of psychiatry in the UK.12 Every three years, PAs in the Netherlands are surveyed for trends and new developments to adjust supply and demand of societal needs.6 Our results show that PAs in the Netherlands spend most of their time on direct clinical care. This is in line with results from other PA populations. In the UK, on average, PAs are contracted for 34 hours for direct clinical care, besides other professional and academic activities.9
Conclusion
While the Dutch PA movement has been underway for 2 decades, each new PA is an addition to the medical workforce rather than replacing another or retiring PA. While demand will eventually level out, the ideal number or PA ratio in the healthcare workforce remains unknown. Life expectancy in the Netherlands is relatively high. Furthermore, there is an ageing population and the utilisation of healthcare services is growing.14,15 In the coming decades, we therefore expect that the PA will become further established inside and outside hospital settings, with a particular increase in elderly care and family medicine. Also, the tasks performed by PAs are still evolving. It would be of interest to compare developments in various countries to optimise PA implementation in healthcare.
Acknowledgements
The authors acknowledge RS Hooker for his valuable suggestions and input regarding the conceptualisation and revision of this manuscript.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.