
Introduction
Clinicians are often best placed to identify problems and design solutions within their clinical environments. Current training scheme requirements for doctors in training mandate participation in quality improvement projects (QIPs).1 Often the ‘lived experience’ for trainees is that these QIPs are simplistic, not aligned to the departmental needs, and hence not sustained following trainee doctor rotations.2
The InQuIRe (In-hospital Quality Improvement for Respiratory) Faculty was formed in August 2020 as a departmental quality improvement (QI) faculty at a large teaching hospital with two acute hospital sites. The faculty's vision was to increase participation in QI across our multidisciplinary clinical staff, with a framework and support for mentorship and sponsorship.
Materials and methods
Our aims were to:
increase the number of respiratory QIPs registered on the LifeQITM platform
improve engagement and progression for respiratory QIPs
improve handover and sustainability of QIPs at times of trainee rotation.
Multiple plan, do, study, act cycles were devised to test change ideas aligned to our primary improvement drivers, namely: QI training for staff, QI participation, communication of active QI work to wider staff and progression of QI work past the initial planning phase.
Members of the multidisciplinary team, including medical, nursing, physiotherapy, pharmacists and clinician library staff, were invited to join the faculty. Fortnightly meetings were held to discuss the progress of departmental QIPs and troubleshoot difficulties. More recently, an educational focus using action learning sets has been introduced. Some staff have progressed to become local or national improvement leaders. Many individual respiratory QIPs have been presented at national improvement conferences.
Results and discussion
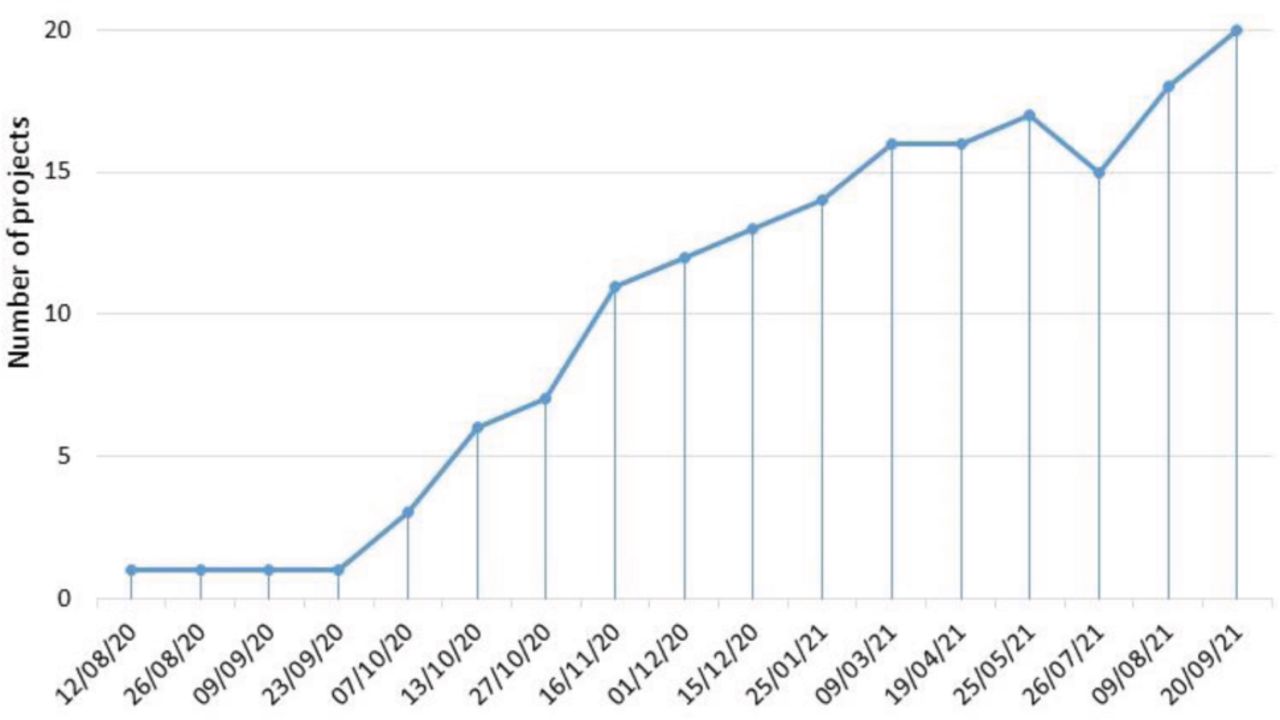
23 new QIPs were registered in the first year of the faculty (Fig 1). The mean LifeQITM QI progression score improved from 0 to 1.63. Some individual projects became sustainable, reaching a progression score of 4.5. Five projects were subsequently closed due to completion or lack of progression.
Some of our more successful projects have led to embedded system change, scaling at trust level and measurable improvements in patient outcomes. This was most seen in projects where faculty members were directly involved in mentoring the QIP team. However, some projects struggled to progress, often related to limited senior sponsorship and the impact of COVID-19 operational workforce pressures.
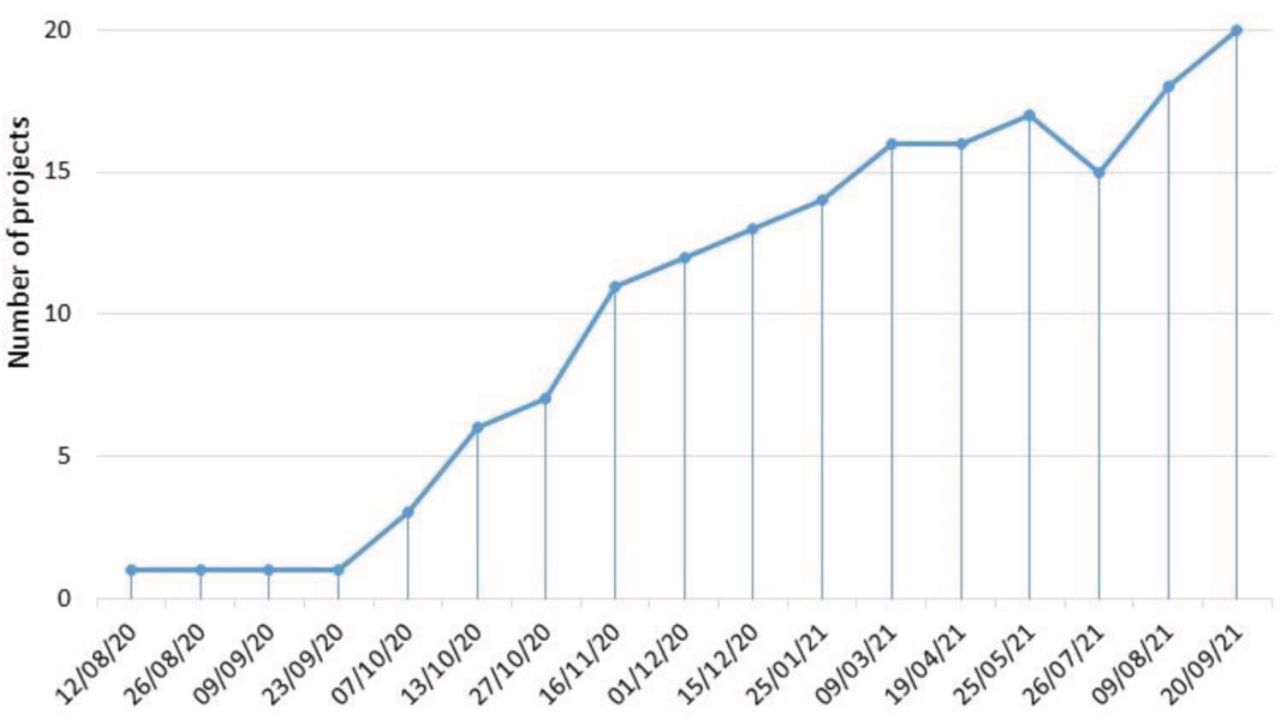
Number of active quality improvement projects registered in the respiratory department.
Conclusion
The departmental QI faculty has enabled a process for rotating medical staff to join existing projects rather than starting new, unsustainable projects. There is now oversight of all QI work across the department with fortnightly faculty meetings. We have shown that a multidisciplinary QI faculty can embed a culture of continuous improvement and lead to sustainable change. It is a useful model for improving access, organisation and project progression across a large department and may be transferrable to other departments within NHS organisations. A faculty should ideally be supported by dedicated administration support and time allocated for members to do this work in order to be sustainable in the future.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.