
Introduction
The Joint Advisory Group on Gastrointestinal Endoscopy (JAG) biennial census provides an insight into the provision of UK endoscopy services.1,2 Since the last census 2 years ago, there has been a significant change in every aspect of endoscopy, brought on by the COVID-19 pandemic.3–5 We report on the 2021 census which was conducted to understand both the impact of COVID-19 and ongoing pressures on endoscopy services.
Methods
The JAG Quality working group developed an initial question set which was refined and reviewed by key JAG stakeholders. The census was disseminated to all JAG-registered services in April 2021 using an online survey platform. Prior to analysis, any missing data from services were sought as part of a second-step verification process. Data were analysed across the domains of endoscopic activity, waiting time targets, workforce, COVID-19, safety, gastrointestinal (GI) bleeding, anaesthetic support, equipment and decontamination. Outcome variables from each section of the census were analysed against independent variables derived from service-specific core demographic data (JAG accreditation status, sector and region) using a variety of statistical methods. Statistical significance is indicated by p<0.05.
Results
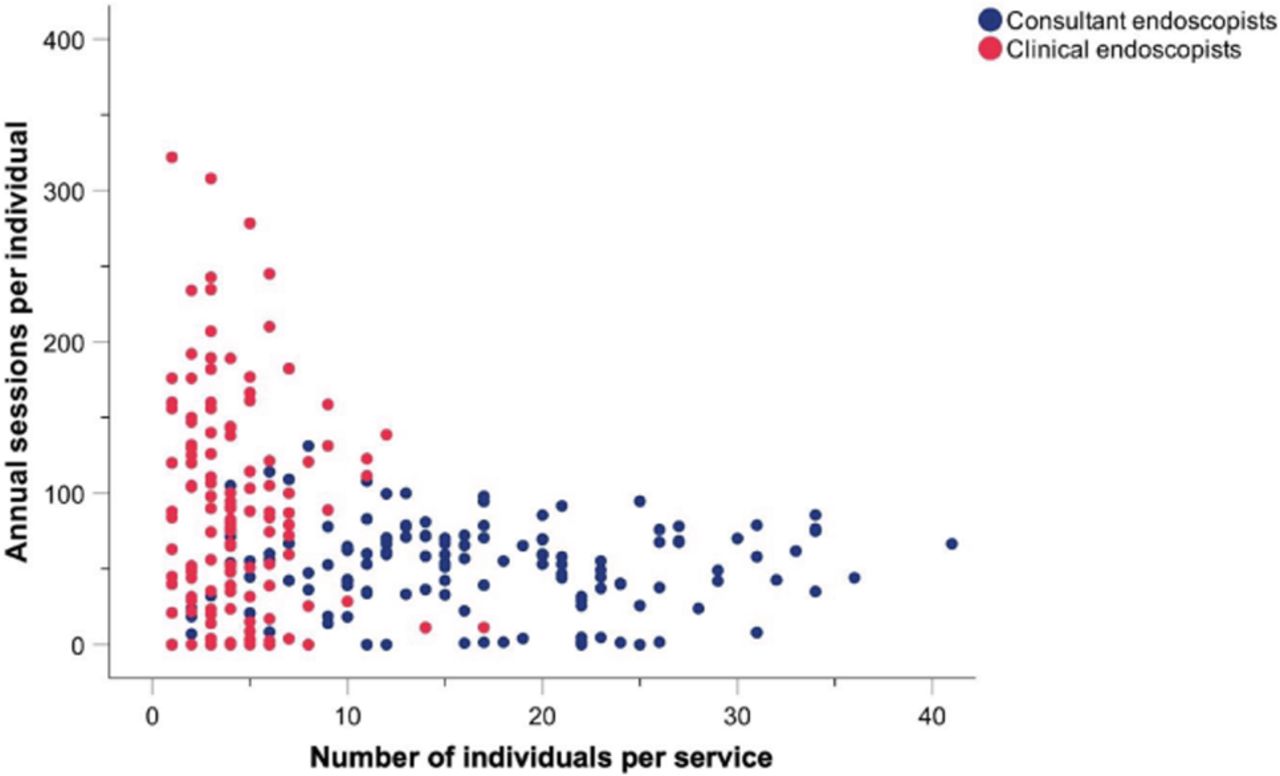
Overall, 321 services completed the census, with information pertaining to 393 individual units (response rate 79.2%). In the first 3 months of 2021, 66.0% of services met urgent cancer waits, 38.7% met routine waits and 33.9% met surveillance waits (Fig 1). Workforce redeployment was the predominant reason cited for not meeting targets. There were significant regional differences in the proportion of patients waiting 6 or more weeks (p=0.001). During the pandemic, 64.8% of NHS endoscopy services had staff redeployed and there was a mean sickness rate of 8.5% with no clear variation across sectors or regions. Endoscopic activity was outsourced. Services were, on average, at 79.3% activity compared with 2 years ago. JAG accredited services were more likely to meet urgent cancer waits, with a lower proportion of patients waiting 6 weeks or more (p=0.03). Clinical endoscopists, who make up 11.0% of the endoscopist workforce, had a significantly greater number of annual planned sessions per individual than consultant colleagues (p<0.001), who make up 81.0% of the workforce (Fig 2). Out of acute services, 86.9% had access to out-of-hours GI bleed cover. Anaesthetist-supported lists were provided in 65.4% of services. Over 10% of services stated that equipment shortage interferes with service delivery. Overall, 42.7% of services would require additional building works to decontaminate more scopes.
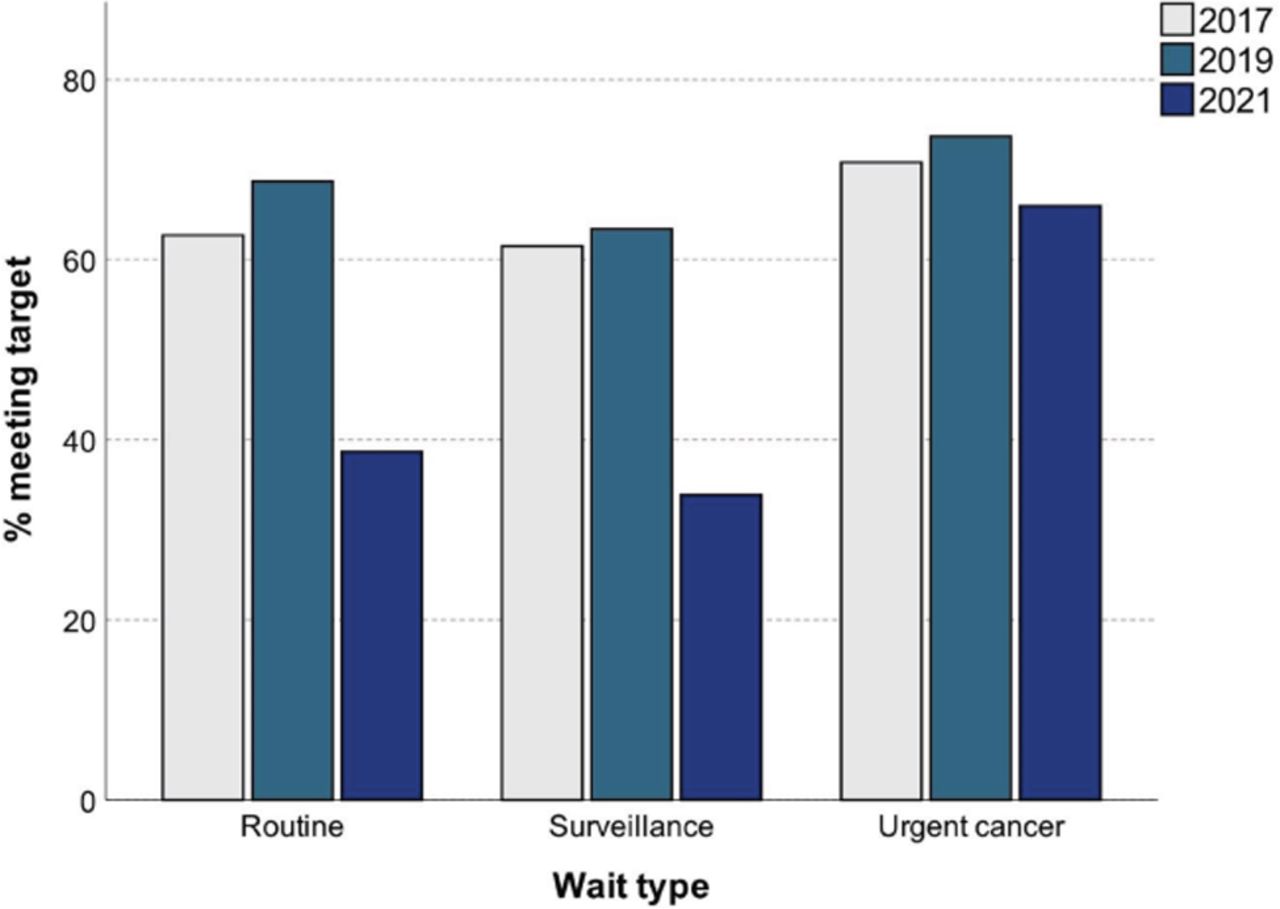
Clustered bar chart demonstrating percentage of services meeting waiting time targets over successive census years.
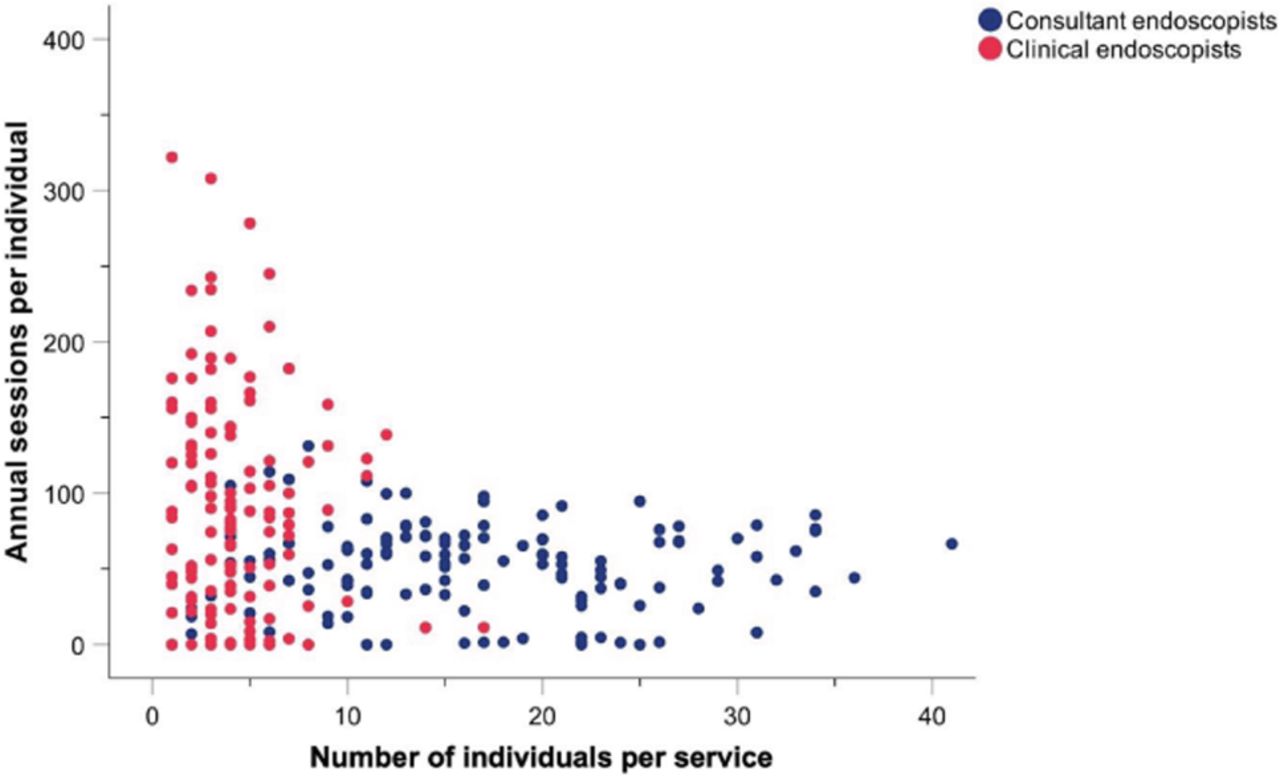
Scatter diagram of planned annual sessions per individual by number of individuals, defined as clinical or consultant endoscopist.
Conclusion
Services are adapting to continued pressure and there are signs of a focused response to demand during a time of ongoing uncertainty. Adherence to service performance was more likely in JAG accredited services. Additionally, a significant minority of services reported equipment shortage and the need to improve infrastructure. These findings will inform ongoing guidance from JAG and key stakeholders.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.