
Introduction
COVID virtual wards were introduced by NHS England in January 2021 in an attempt to facilitate the early supported discharge of patients hospitalised with COVID-19 through closely supervised community follow up.1 The ‘COVID virtual ward round’ is a hospital-led service wherein patients have daily virtual review from a clinician to review their progress. It differs from ‘COVID oximetry @ home’ which is a general practitioner (GP)-led service for the monitoring of lower acuity COVID-19 positive patients.1
There are several different referral pathways into the COVID-19 virtual ward as displayed in Table 1.
Referral criteria for COVID oximetry @ home and COVID virtual ward round services
When COVID-19 cases began increasing in December 2021 due to the highly contagious novel Omicron variant, there were fears hospitals could become overwhelmed with COVID-19 admissions, hence a drive to utilise the COVID virtual ward service.2
At Princess Royal University Hospital (PRUH), a district general hospital in South-East London, we were not meeting the target COVID virtual ward referral numbers of 15% of the total COVID-19 admissions, so decided to complete an audit to review possible reasons why.
Materials and methods
At PRUH an electronic spreadsheet is produced daily detailing all adult inpatients with a positive COVID-19 PCR test. On 13 January 2022, we analysed the day's spreadsheet and reviewed the clinical notes of all COVID-19 positive adult inpatients, extracting the following data:
If patients had symptoms of COVID-19 (ie cough, breathlessness, anosmia, coryzal symptoms, headache or myalgia) or were asymptomatic
Supplemental oxygen requirements
If patients required ongoing inpatient (IP) care or were medically fit for discharge (MFFD)
If MFFD what the discharge delay reason was
Patient suitability for step-down to a COVID virtual ward based on NHS England guidelines (see Table 1).
We excluded patients aged <18 years and those without a positive PCR swab result.
Results and discussion
On 13 January 2022, there were 85 inpatients at PRUH with a positive COVID-19 PCR test.
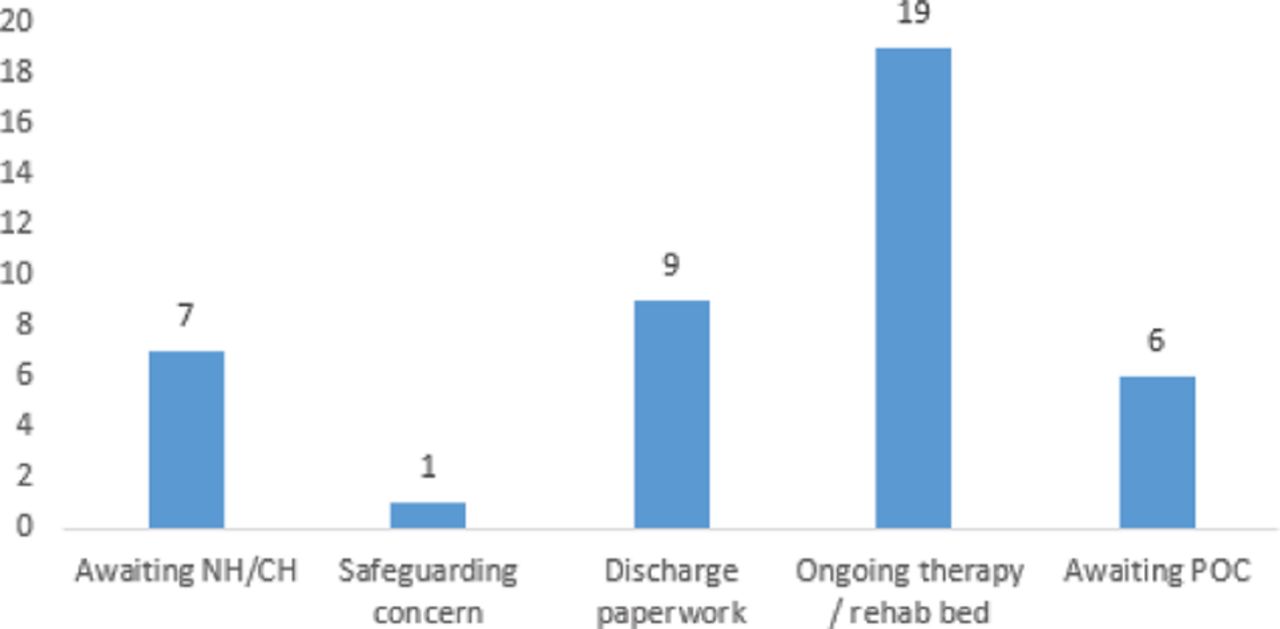
20 patients (24%) had signs/symptoms of COVID-19, whereas 65 (76%) were asymptomatic. Nine patients (11%) were requiring supplemental oxygen and 76 (89%) were not. 43 (51%) required ongoing IP care and 42 (49%) had been deemed MFFD. Of those needing IP care, only seven (16%) needed COVID related treatement. Only two patients (2%) met criteria for referral to the COVID virtual ward service (for low dose oxygen weaning) and the remaining 83 patients (98%) did not. The most common cause for discharge delay among MFFD patients was ongoing therapy (42%; see Fig 1).

Causes of discharge delay in medically fit for discharge patients
The majority of patients in our cohort were asymptomatic, with many identified as COVID-19 positive when admitted for an alternative cause, so most did not require step-down to the COVID virtual ward.
Conclusion
The COVID virtual ward can facilitate early discharge of COVID-19 positive patients; however, the target of referring 15% of all COVID-19 inpatients to the service was unrealistic in our district general hospital, with only 2% of our cohort eligible.
We propose increasing therapy services would better improve patient flow in our trust.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.