
ABSTRACT
Background Evidence suggests that discussing resuscitation with patients and relatives from ethnic minority groups is problematic for healthcare professionals (HCPs), but there is limited evidence exploring these issues or offering guidance for HCPs in navigating these challenging discussions. This study explores the barriers and enablers to HCPs discussing deterioration and resuscitation decisions with patients and families from ethnic minority groups.
Results Personal, cultural, religious/spiritual and health beliefs, emotions, and communication quality and skills were discussed. Participants described that the interaction between these factors as complex, impacting the way some patients and families responded to do not attempt cardiopulmonary resuscitation (DNACPR) orders and the particular challenges these pose.
Conclusion Key barriers and enablers for healthcare professionals discussing resuscitation with patients and families from Black, Asian and minority ethnic communities were identified. The findings highlight areas of improvement for training, both relating to DNACPR discussions and ‘cultural competence’.
Introduction
Advance care planning (ACP) offers people opportunities to discuss and document their wishes for the way they wish to be cared for when they become seriously ill. This includes discussions about cardiopulmonary resuscitation (CPR), where the success and outcome of CPR is uncertain. ACP includes decision making around whether to attempt CPR in the event of cardiorespiratory arrest. Decision making often involves discussions with the patient or their next-of-kin, and may include palliative care specialists. Alternatively, doctors or senior nurses may decide that attempting CPR would be futile.
ACP and DNACPR derive from western ethical and legal frameworks prioritising autonomy. ACP has been shown to improve outcomes at the end of life, resulting in higher quality of life and patient satisfaction.1 Evidence suggests people from ethnic minority groups engage in ACP less frequently.2–5 Ethnic minority patients access specialist palliative care services less frequently and later.5,6
Healthcare professionals (HCPs) in the UK report a lack of confidence, knowledge and skills in providing culturally sensitive end-of-life care for ethnic minority patients and in undertaking ACP with patients generally.7,8 Here, we will present findings from the ‘Thinking ahead study’ which explored the nuances of discussing resuscitation with ethnic minority patients and relatives in the UK, and the interventions that doctors and nurses perceive have improved their confidence, knowledge and skills in these situations. The study was conducted from October 2016 to June 2018 in Leicester, the first UK city where no single ethnic group is in the overall majority, as 55% of the population self-reported their ethnicity as non-White British and almost a quarter of residents over 60 years are from ethnic minority groups.9,10
Methods
Thirty-two semi-structured qualitative interviews were conducted with senior medical and nursing staff working in hospitals, hospice and community settings.
Recruitment
Experienced doctors (general practitioners (GPs), consultants, registrars (ST3 equivalent or above)) and senior nurses (band 6 and above) who had self-reported experience of working with patients from ethnic minority groups were purposely sampled to represent professional experience across a range of settings and specialties.
Twenty doctors and 12 nurses were recruited from a range of clinical areas (Table 1). Eleven were men and the sample was ethnically and religiously diverse with 31% from non-White British backgrounds. Fifty-three per cent described themselves as Christian, 21% had no religion, 6% were Sikh, 6% were Hindu and 12% were Muslim.
Profession of respondents to interviews
A topic guide was iteratively developed to explore confidence in discussing DNACPR, perceived barriers and facilitators to DNACPR conversations with ethnic minority (and other) groups, impact and influence of patients’ health/faith/cultural beliefs and practices, training (received or needed), and effects and consequences of end-of-life care planning. Informed consent was taken at the beginning of each interview and all interviews were audio recorded and transcribed verbatim.
Ethical approval was granted by the University of Leicester Ethics Sub-Committee for Medicine and Biological Sciences (IRAS Ref 200998). Health Research Authority (HRA) approval was sought and granted after recommendation by the sponsor, University Hospitals of Leicester NHS Trust.
Analysis
Data was analysed using the constant comparison approach of grounded theory.11 Transcripts were coded separately by two of the authors through an iterative process of reading, reflection, re-reading, coding and interrogation, followed by a process of discussion of codes and then further interrogation by the research team. Data analyses were supported by NVivo 11.
Results
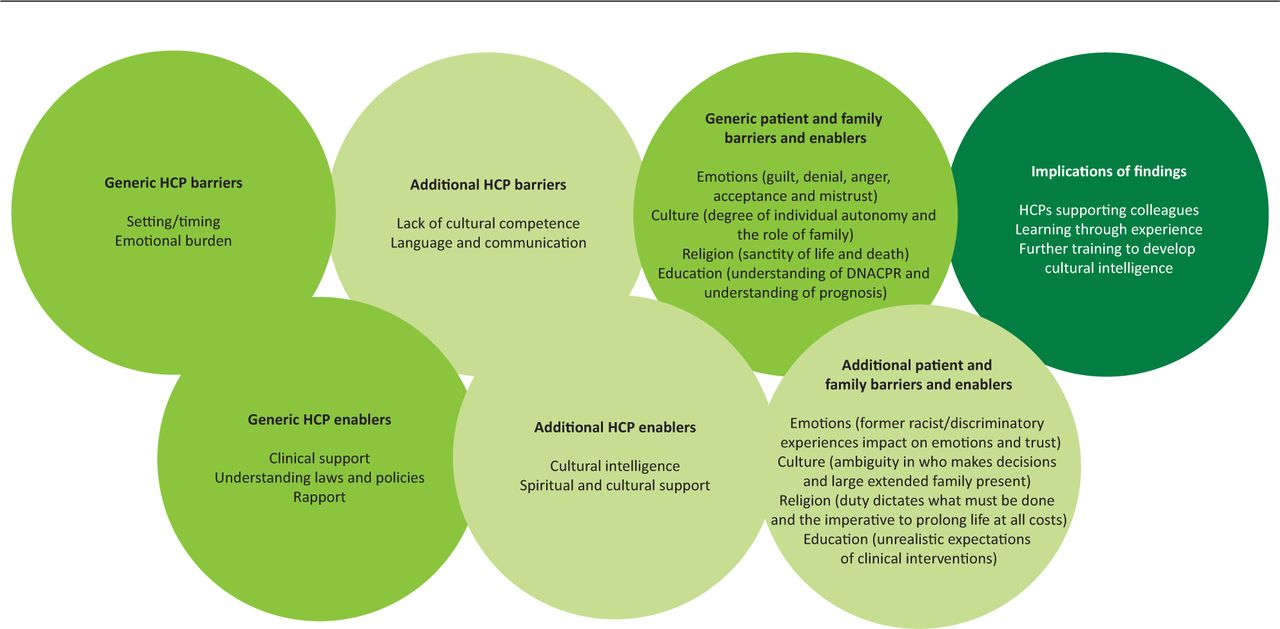
Participants identified universal challenges in decision making with patients and relatives, regardless of ethnic background. The emotive nature of the discussions along with the perceived acceptance of the patient's prognosis and their understanding of DNACPR were key influencers in the discussion. Participants identified factors that increased the complexity of having resuscitation discussions with patients and families from ethnic minority groups. Fig 1 is a framework demonstrating both generic and additional ethnic minority-specific barriers and enablers faced by patients and HCPs in having the resuscitation discussion and the implications of these findings. Key themes identified in Table 2 are explored.
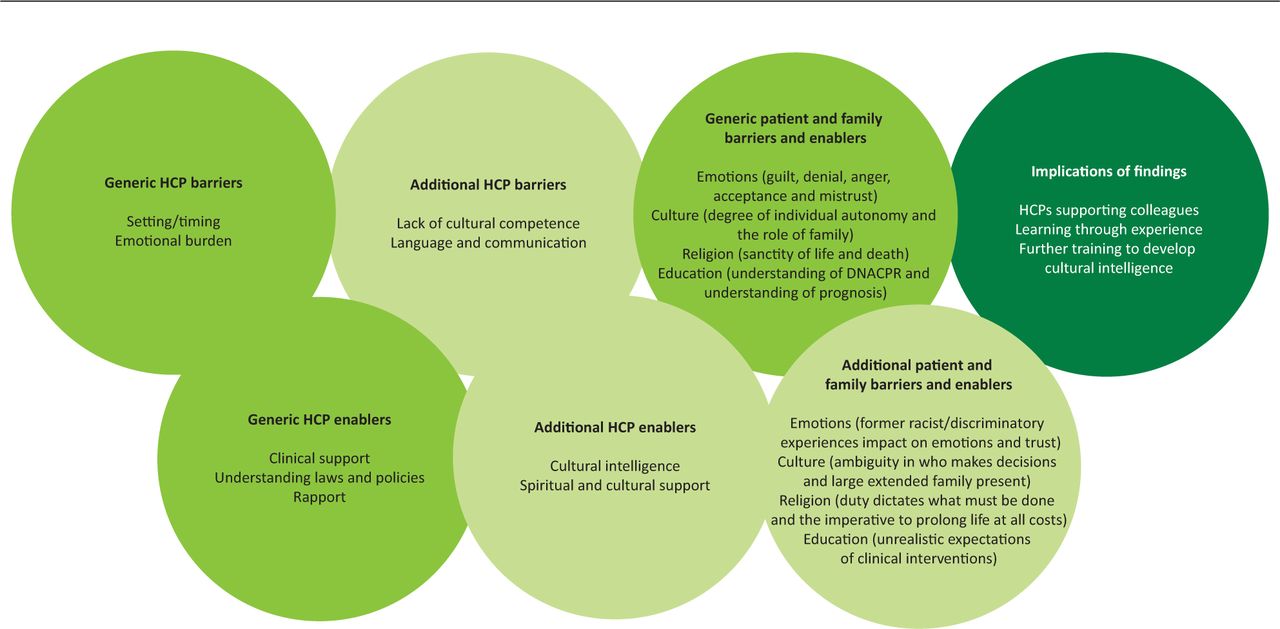
Generic and additional ethnic minority-specific barriers and enablers faced by patients and healthcare professionals in having the resuscitation discussion. DNACPR = do not attempt cardiopulmonary resuscitation; HCP = healthcare professional.
Themes of generic and additional ethnic minority-specific barriers
Additional patient and family barriers: individual autonomy and the family culture
All participants emphasised that their preference was to speak primarily to the patient about resuscitation decisions. GPs and some nurses gave examples of what they perceived to be lack of autonomy among older Asian patients. Some participants reported that patients did not wish to speak about resuscitation, they preferred that the doctor made decisions for them while others wanted to consult their family for decision making.
Participants discussed their experiences of collaborative decision making in some South-Asian communities, often manifesting as a result of a language barrier, a male relative or community member would act as a ‘spokesperson’ for the patient. Female relatives were perceived as being discouraged or prohibited from taking part in the discussion. Participants talked about the tensions this raised in their duty of care for the patient in determining if the patient's own wishes were being met. H32, oncology nurse specialist:
We can't even sometimes get through to the patient and ask them [about resuscitation] because the family are guarding the patient.
H06, palliative nurse specialist:
Sometimes culturally the oldest son … will take charge … And we have to accept that is maybe culturally what is expected of him but at the same time, you never feel quite so confident because … you need to be broaching it with the patient, not just with that family member.
The number of people present at discussions also presented challenges. In the outpatient setting, discussions were usually between the doctor, patient and usually one relative. However, in the home or inpatient setting, large groups were more typical. Participants reported uncertainty determining who information should be shared with and gained from, and how to manage the situation sensitively. H01 surgical registrar:
Sometimes with Asian families in particular … [there are] 30 people at once or something, [it] is pretty intimidating … Whereas European families or Black families … it’ll tend to be a smaller number of people.
Additional HCP barriers: language and communication
Most participants spoke about the obvious challenge of a language barrier. Using interpreters was reported to assist, but several complexities were identified.
Participants questioned the quality of translation, including inaccuracies due to misinterpretation by any agent in the conversation, or to a lack of direct translations for certain words or concepts. H21 GP:
None of these words [about resuscitation] mean anything. So, you have to explain about jumping, you know, pushing your chest down. You know, do you want us to put a bag over your face and give you air? And it's using the appropriate language for the appropriate person is key to allow them to understand what you are going to put them through.
Instances of serious actual or potential omissions, especially when family members acted as interpreters, were reported (such as choosing not to disclose the prognosis or question about resuscitation to the patient or convey their own opinions rather than the patient's). Such issues were also identified when using professional interpreters, where cultural taboos or other reasons may prevent transparent translation. H22 haematology consultant:
I’ve transplanted patients whose embassy [interpreters] had told them they had a little weakness in the blood, but they clearly had acute leukaemia … The embassy pays us to do this work and we’ve been told that we’re only to use the embassy interpreters [but] they’ve been told what can be translated.
No participant recalled having training on working with interpreters, although some had trained juniors informally. Participants felt that they had learnt from positive and negative experiences, but many still lacked confidence using them. Some participants shared tips for working with interpreters when having conversations about deterioration and CPR. This included preparing the interpreter about the focus of the conversation and likely emotional reactions because of the possibility that the interpreter may become upset. H22 haematology consultant:
I have seen an interpreter burst into tears because they were going to have to tell a very young patient with small children that this was a fatal disease and that the treatment wasn't working … I think we probably ought to talk to our interpreters after the meeting; one, to get their view on the [family] dynamic … And, how are you? You know, are you alright? So that they actually have an opportunity to download, because we are really poor at it.
Generic patient and family barriers and enablers: religious reasoning (sanctity of life and death)
Some participants reported experiences with a small number of patients and a larger proportion of family members who wished to prolong life at all costs. Some participants expressed concern that patients appeared to be ‘cocooned’ by family as a result of cultural expectations around duty and care. Hence, they wanted doctors to attempt resuscitation despite the clinical opinion regarding considerable harms or absence of benefit in the intervention. They described how this was commonly framed religiously as the sanctity of life, and participants found it difficult to challenge such arguments. Some participants identified specific communities they perceived as following this ideology. Muslims were most frequently identified by participants but examples of patients from Catholic, other Christian denominations, Orthodox Jewish, Traveller and African backgrounds were all mentioned, demonstrating the breadth of this reasoning. Describing a meeting after the patient's death with a Muslim family who had opposed a DNACPR decision, H16 palliative consultant:
I said to them, ‘You seem much more at peace with what's happened today than you were on Friday.’ And he said, ‘While she was alive, our duty was to fight to give her life.’
However, most participants recognised that this belief was not universal across these communities or religions, and felt that the wish for resuscitation was shaped more by personal interpretation rather than religious teachings per se. H21 GP:
So, you have to be careful that you don't say, ‘Somebody is a Sikh, therefore, they will react in this way.’ What you have to say is [that] they have a belief system, but they will have a variable belief system. And this same rule applies to the Muslim faith, the Hindu faith etc.
Participants also identified factors that they had found facilitated effective DNACPR discussions.
Additional HCP enabler: cultural intelligence
Participants gave examples of how cultural intelligence enabled them to navigate situations and ensure that the patient was offered full information about their prognosis despite family members intervening and appearing to place a barrier to this. Asking patients and their families to share their reasoning behind their views was a specific communication skill that deepened disclosure, and shared understanding and enabled personalised discussions. H11 palliative consultant:
I’ll say to people, ‘Help me understand [why they disagree],’ and then that might help with trying to make [my] explanations and discussions better kind of fit to their world view.
One participant explained how findings from a study, which identified that people from ethnic minority groups wanted more information about their disease, made them feel more confident in challenging family members.
A shared cultural background was described by some as a facilitator in challenging religious viewpoints. For instance, a participant from a Muslim background themselves described an occasion when they had used their knowledge of the Qur’an to challenge a Muslim family's belief that not attempting resuscitation went against their faith. H09 medical registrar:
[In the Qur’an, there are verses about] respect of the body, respect of the person and how you need to ensure that the person lives dignified and respectful. So … when I noticed that their mind is set that you have to resuscitate, I had to say, ‘How do you think about [these verses]?’
Additional HCP enabler: spiritual and cultural support
Utilising chaplaincy services to help overcome misconceptions and explore the patient's belief system was considered a useful resource. Cultural support workers to explain context to professionals and guide culturally appropriate ways of having DNACPR discussions with particular ethnic minority groups was also mentioned, and one nurse had sought support from the Muslim Council of Britain.
Training and support: in conducting DNACPR discussions and cultural competence
The majority of doctors emphasised the need for earlier career training regarding the law and how to broach the DNACPR discussion with patients from diverse communities and involve their family members in the discussion. None of the nurse participants mentioned this as being a need, but some spoke of the importance of having support and guidance from more experienced colleagues. H03 cardiology nurse:
It's really hard to sit in somebody's front room … and initiate a conversation about them dying when their pictures are around you and that. So, I don't know if it's all about training. I think you need some support, so when you have these conversations there is a debrief or there is somebody you can go to.
All participants had completed ‘culture and diversity awareness’ eLearning modules. They felt that this was a convenient platform, useful for learning facts, but opinions were largely negative as it was perceived as focusing on poor practice rather than guiding good practice.
Those who felt most confident providing culturally sensitive care to patients identified cultural competency training as helping them to understand the similarities and differences between different ethnicities, and to feel confident talking about beliefs without feeling intrusive.
Courses which were tailored to the participant's role and experiences were recalled as useful. Participants agreed that more communication skills training focusing on the task of DNACPR discussions would be valuable and that cultural competency training should be developed to provide doctors with an appreciation of how this plays out in clinical contexts, decision making and end of life. H07 renal consultant:
I know from an epidemiological and genetic point of view how they’re different … But then you have to factor in whether they’re first generation, second generation, and all the other complexities that come with it … We are taught the generics of treating everyone equally and fairly and accepting diversity, but nothing about the peculiarities of beliefs.
The majority favoured using face-to-face training using real case scenarios and simulations with opportunities to share experiences to discuss ‘best practice’ and talk to expert patients. H23 GP:
Perhaps the most valuable thing might be the opportunity to, you know, sit down with some expert patients who have been there, who have had that discussion and kind of understand what they, you know, understand their view.
Discussion
This study offers much needed insight into the challenges that HCPs face when discussing DNACPR with patients from ethnic minority groups, facilitating a deep exploration of individual HCP experiences in one of the most diverse areas of the country.
Like others, our findings highlight that challenges in communication between HCPs, patients and their families are a key barrier to resuscitation discussions.6,7 Building rapport and explaining the condition and prognosis were key enablers, particularly when patients and their families appeared to have limited knowledge of their prognosis. Using professional interpreters was considered an imperfect best practice, where significant challenges remained; certain words or concepts may not be directly translatable and there were concerns regarding quality assurance.
Most participants recognised heterogeneous preferences for decision-making processes. However, their dominant ethical and legal framework prioritised patients’ autonomy. Understanding was very limited as to how to accommodate different preferences, which were felt to be more common with ethnic minority patients. Our findings suggest that supporting clinicians in how to assess these factors and develop skills in wider stakeholder decision-making would be valuable.
Our study explores the viewpoint of one stakeholder within these discussions. Participants’ perceptions of patients’ and families’ thoughts and wishes is based on reflective speculation and does not explore the views and experiences of patients and relatives.
There was a lack of understanding of how all the various forms of social stratification (such as class, ethnicity, sexual orientation, age, religion, disability and gender) impact on lived experiences and inform belief systems. This intersectionality impacts on patients’ and their families’ perceptions of ACP and related resuscitation decisions.12 While the themes of language, family and religious beliefs are established within the discussion of trans-cultural clinical practice, our findings identify how these may cumulate in DNACPR discussions appearing to ask patients to choose whether to live or die. This can lead to feelings of mistrust and conflict. Our findings highlight that current training is limited and does little to tackle such complexities.
Participants felt more confident in having DNACPR discussions when they had existing knowledge about patients’ religious, spiritual and cultural values. Their confidence leading these conversations was developed experientially. Our findings highlight the need and desire for further training to develop ‘cultural intelligence’ to navigate the taboos about death and deliver culturally sensitive end-of-life care, including discussing deterioration and decisions about resuscitation.6
HCPs have a professional responsibility to demonstrate reflective practice and continuous development, and so it could be deemed unprofessional to refuse training or declare oneself as being perfect at having such difficult conversations.13 However, being able to probe participants about what this training could comprise has provided a valuable evidence base for future research. Future training needs to create opportunities for HCPs to share experiences of good practice, as well as recognise unintentional and unacknowledged biases, anxieties and prejudices about other cultural values and beliefs.14
Conclusion
HCPs find conversations about deterioration and resuscitation challenging generally. Additional factors related to communication, religion and family increases this complexity when the patient is from an ethnic minority group. HCPs receive little training in navigating this complex intersectionality.
In this study, HCPs sought to access reflective support, sharing of practices with colleagues and learning though simulated scenarios. Novel approaches are required to ensure that the focus of training is upon empowering HCPs to probe patients’ beliefs, maintaining their focus on the individual rather than providing ‘recipe’ type approaches which can lead to stereotyping communities.
Summary
Acknowledgements
This study was funded by LOROS and the study sponsor was the University Hospitals of Leicester NHS Trust. We would like to thank all the participants who freely gave up their time to take part in this study. We would also like to thank Dr Helen Eborall, lecturer, from the University of Leicester and Dr David Miodrag, consultant in palliative medicine, from John Eastwood Hospice for their input in the design and development of the study.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.