
Abstract
BACKGROUND: Symptoms are common and often remain medically unexplained.
OBJECTIVE: To assess 5-year symptom outcomes, determine how often symptoms remain unexplained and assess their relationship with mental disorders.
DESIGN: Prospective cohort study.
PARTICIPANTS: Five hundred consecutive patients presenting to a medicine clinic with physical symptoms.
MEASUREMENTS PREVISIT: Mental disorders, symptom characteristics, stress, expectations, illness worry, and functional status. Post-visit (immediately, 2 weeks, 3 months, 5 years): unmet expectations, satisfaction, symptom outcome, functional status, and stress.
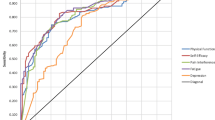
RESULTS: While most subjects (81%) experienced symptom improvement by 5 years, resolution rates were lower (56%), with 35% of symptoms remained medically unexplained. Most patients with medically unexplained symptoms (MUS) did not have a mental disorder. Mood or anxiety disorders were not associated with MUS (relative risks [RR]: 0.94, 95% confidence interval [CI]: 0.79 to 1.13), or with lower rates of symptom improvement (RR: 1.14, 95% CI: 0.60 to 2.2). In contrast, most patients with somatoform disorders had MUS and were unlikely to improve. Worse functioning (RR: 0.95, 95% CI: 0.91 to 0.99), longer duration of symptom at presentation (RR: 0.5, 95% CI: 0.28 to 0.87), illness worry at presentation (RR: 0.56, 95% CI: 0.35 to 0.89), or lack of resolution by 3 months (RR: 0.47, 95% CI: 0.26 to 0.86) reduced the likelihood of symptom improvement at 5 years.
CONCLUSIONS: More than half of patients presenting with a physical symptom resolve by 5 years, while a third remain medically unexplained. Most patients whose symptom remained unexplained had no mental disorder. While mood and anxiety disorders were not associated with MUS or worse outcomes, most patients with somatoform disorders had MUS and were unlikely to improve.
Similar content being viewed by others
References
Schappert SM, Nelson C. National Ambulatory Medical Care Survey 1995–96 summary. Vital Health Stat. 1999;13:1–122.
Von Korff M, Deyo RA, Cherkin D, Barlow W. Back pain in primary care: outcomes at one year. Spine. 1993;18:855–62.
Valdini AF, Steinhardt S, Valicenti J, Jaffe A. One-year follow up of fatigued patients. J Fam Pract. 1998;26:33–8.
Kroenke K, Lucas CA, Rosenberg ML, Scherokman BJ, Herbers JE. One-year outcome in patients with a chief complaint of dizziness. J Gen Intern Med. 1994;9:684–9.
Weber BE, Kapoor WN. Evaluation and outcomes of patients with palpitations. Am J Med. 1996;100:138–48.
Wasson JH, Sox HC, Sox CH. The diagnosis of abdominal pain in ambulatory male patients. Med Decis Making. 1981;1:215–24.
Arndorff DK, Knottnerus JA, Hujjnen LG, Sarmans R. How well do general practitioners manage dyspepsia? J R Coll Gen Pract. 1989;39:499–502.
Martina B, Buchell C, Strotz M, Battega E, Gyr N. First clinical judgement by primary care physicians distinguishes well between nonorganic and organic causes of abdominal or chest pain. J Gen Intern Med. 1997;12:459–65.
Kroenke K, Jackson JL. Outcome in general medical patients presenting with common symptoms: a prospective study with a 2-week and a 3-month follow-up. Fam Pract. 1998;15:398–403.
Marple RL, Kroenke K, Lucey CR, Wilder J, Lucas CA. Concerns and expectations in patients presenting with physical complaints: frequency, physician perceptions and actions, and two-week outcome. Arch Intern Med. 1997;157:1482–8.
Kirmayer LJ, Groleau D, Looper KJ, Dao MD. Explaining medically unexplained symptoms. Can J Psychiatr. 2004;49:663–72.
Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med. 1989;86:262–6.
Kroenke K, Arrington ME, Mangelsdorff AD. The prevalence of symptoms in medical outpatients and the adequacy of therapy. Arch Intern Med. 1990;150:1685–9.
Richardson RD, Engel Jr., CC. Evaluation and management of medically unexplained physical symptoms. Neurologist. 2004;10:18–30.
Kroenke K, Jackson JL, Chamberlin J. Depressive and anxiety disorders in patients presenting with physical complaints: clinical predictors and outcome. Am J Med. 1997;103:339–47.
Jackson JL, O’Malley PG, Kroenke K. Clinical predictors of mental disorders among medical outpatients. Validation of the “S4” model. Psychosomatics. 1998;39:431–6.
Jackson JL, Houston JS, Hanling SR, Terhaar KA, Yun JS. Clinical predictors of mental disorders among medical outpatients. Arch Intern Med. 2001;161:875–9.
Smith RC, Gardiner JC, Lyles JS, et al. Exploration of DSM-IV criteria in primary care patients with medically unexplained symptoms. Psychosom Med. 2005;67:123–9.
Feder A, Olfson M, Gameroff M, et al. Medically unexplained symptoms in an urban general medicine practice. Psychosomatics. 2001;42:261–8.
Nease Jr., DE, Volk RJ, Cass AR. Does the severity of mood and anxiety symptoms predict health care utilization? J Fam Pract. 1999;48:769–77.
Creed F, Barsky A. A systematic review of the epidemiology of somatisation disorder and hypochondriasis. J Psychosom Res. 2004;56:391–408.
Henningsen P, Zimmermann T, Sattel H. Medically unexplained physical symptoms, anxiety, and depression: a meta-analytic review. Psychosom Med. 2003;65:528–33.
Maiden NL, Hurst NP, Lochhead A, Carson AJ, Sharpe M. Medically unexplained symptoms in patients referred to a specialist rheumatology service: prevalence and associations. Rheumatology (Oxford). 2003;42:108–12.
Jackson JL, Strong J, Cheng E, Meyer G. Patients, diagnoses, and procedures in a military internal medicine clinic, comparison with civilian practices. Military Med. 1999;164:194–7.
Jackson JL, O’Malley PG, Kroenke K. A psychometric comparison of military and civilian medical practices. Military Med. 1999;164:112–5.
Jackson JL, Kroenke K. The effect of unmet expectations among adults presenting with physical symptoms. Ann Intern Med. 2001;134:889–97.
Ware JE, Nelson EC, Sjerbpirme CD, Stewart A. Preliminary tests of a 6-item general health survey: a patient application. In: Ware JE, Stewart AL, eds. Measuring Functioning and Well Being: The Medical Outcomes Study Approach. 1st ed. Durham: Duke University Press; 1997:199–308.
Kroenke K, Spitzer RL, Williams JB. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. 2002;64:258–66.
Spitzer RL, Williams JB, Kroenke K, et al. Utility of a new procedure for diagnosing mental disorders in primary care: the PRIME-MD 1000 study. JAMA. 1994;272:1749–56.
Loerch B, Szegedi A, Kohnen R, Benkert O. The primary care evaluation of mental disorders (PRIME-MD), German version: a comparison with the CIDI. J Psychiatr Res. 2000;34:211–20.
Kroenke K, Spitzer RL, deGruy III FV, et al. Multisomatoform disorder. An alternative to undifferentiated somatoform disorder for the somatizing patient in primary care. Arch Gen Psychiatr. 1997;54:352–8.
Rubin HR, Gandek B, Rogers WH, Kosinski M, McHorney CA, Ware JE. Patients’ ratings of outpatient visits in different practice settings: results from the Medical Outcomes Study. JAMA. 1993;270:1449–53.
Spitzer RL, Kroenke K, Williams JB, Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282:1737–44.
O’Malley PG, Jackson JL, Kroenke K, Yoon IK, Hornstein E, Dennis GJ. The value of screening for psychiatric disorders in rheumatology referrals. Arch Intern Med. 1998;153:2357–62.
Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom. 2000;69:205–15.
Speckens AE, van Hemert AM, Spinhoven P, Hawton KE, Bolk JH, Rooijmans HG. Cognitive behavioural therapy for medically unexplained physical symptoms: a randomised controlled trial. BMJ. 1995;311:1328–32.
O’Malley PG, Jackson JL, Santoro J, Tomkins G, Balden E, Kroenke K. Antidepressant therapy for unexplained symptoms and symptom syndromes. J Fam Pract. 1999;48:980–90.
Noyes Jr., R, Kathol RG, Fisher MM, Phillips BM, Suelzer MT, Woodman CL. Psychiatric comorbidity among patients with hypochondriasis. Gen Hosp Psychiatr. 1994;16:78–87.
Noyes Jr., R. The relationship of hypochondriasis to anxiety disorders. Gen Hosp Psychiatr. 1999;21:8–17.
Noyes Jr., R, Kathol RG, Fisher MM, Phillips BM, Suelzer MT, Woodman CL. One-year follow-up of medical outpatients with hypochondriasis. Psychosomatics. 1994;35:533–45.
Hernbest RJ, Stewart M. Patient-centeredness in the consultation. Does it really make a difference? Fam Pract. 1990;7:28–33.
Krupat E, Bell RA, Kravitz RL, Thom D, Azari R. When physicians and patients think alike: patient-centered beliefs and their impact on satisfaction and trust. J Fam Pract. 2001;50:1057–62.
Roter DL, Hall JA, Katz NR. Relations between physicians’ behaviors and analogue patients’ satisfaction, recall, and impressions. Med Care. 1987;25:437–51.
Hall JA, Irish JT, Roter DL, Ehrlich CM, Miller LH. Satisfaction, gender, and communication in medical visits. Med Care. 1994;32:1216–31.
Jackson JL. Communication about symptoms in walk-in clinics. J Gen Intern Med. 2005;20(suppl 1):69–70.
Author information
Authors and Affiliations
Corresponding author
Additional information
The opinions expressed in this paper are those of the authors and should not be construed, in any way, to represent those of the U.S. Army or the Department of Defense.
Rights and permissions
About this article
Cite this article
Jackson, J.L., Passamonti, M. The outcomes among patients presenting in primary care with a physical symptom at 5 years. J GEN INTERN MED 20, 1032–1037 (2005). https://doi.org/10.1111/j.1525-1497.2005.0241.x
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1111/j.1525-1497.2005.0241.x