
ABSTRACT
Increasing hospital admissions and staffing pressures mean that most medical registrars find their workload is now heavy or unmanageable. Core medical trainees increasingly think the role of medical registrar is too unattractive or difficult, resulting in less competition for such posts. In autumn 2013, the Future Hospital Commission and Shape of Training outlined their vision to reform postgraduate medical training to better meet the needs of older patients with multiple comorbidities. The Future Hospital Commission proposes that there is a greater emphasis on internal medicine from medical school, with expansion of training opportunities and service provision. Shape of Training recommends a six-year training programme culminating in a Certificate of Specialty Training. New initiatives, such as broad-based training, credentialing and rotas with more continuity, are potential ways to increase training in internal medicine. It is clear that training to achieve generalist expertise is as important as training to achieve specialist expertise.
Introduction
Year on year, medicine continues to advance, yet the day-to-day experience of those practising the art of being a physician appears increasingly challenging. In September 2013, the Future Hospital Commission provided an important and timely vision for the way forward. A major part of its report, Future hospital: Caring for medical patients, outlines changes needed in the work of physicians and therefore the education and training of future doctors.1 The following month saw the publication of The Shape of Training, a national review of the future of postgraduate medical training, sponsored by the Academy of Medical Royal Colleges (of which the RCP is a member), the General Medical Council, the Medical Schools Council and Health Education England.2 This paper will place current challenges in postgraduate education within the context of the training recommendations from both of the recent reports.
Pressures on medical registrars and core medical trainees
The RCP, the Joint Royal Colleges of Physicians Training Board (JRCPTB) and the Future Hospital Commission are aware of the challenges and the need for change after gathering evidence from medical registrars, core medical trainees and the wider workforce. Medical registrars, who mostly comprise higher specialty trainees (ST3+ or SpR) in (general) internal medicine or acute medicine, will be the future consultants during most of the 30-year timeframe explored by the Shape of Training Review. They are also the current ‘workhorse’ of a hospital, as described by other doctors, or, in their own words, the ‘heart of the hospital’ out-of-hours.3 The RCP has been increasingly concerned about the role and work experience of the medical registrar, particularly their role in the delivery of (general) internal medicine. This culminated in last year's publication of The medical registrar: Empowering the unsung heroes of patient care, which gave the results of a survey of over 2800 medical registrars along with recommendations.3 Many of those surveyed enjoyed their roles as senior clinical decision maker, leader of the medical team and teacher to other junior doctors. However, it was also evident that this crucial group of doctors is put under critical pressure by the increase in hospital admissions and changes to the working environment: 26.9% of medical registrars consider their workload ‘unmanageable’ and 70.6% say it is ‘heavy’.4 The trainees working under them recognise this too, with 38.8% of foundation year 2 doctors and 37.4% of core medical trainees believing that the registrar workload is ‘unmanageable’.4 Indeed, these trainees do not think any other registrar is nearly as busy, with the majority believing that the workload is ‘light’ or ‘about right’ for surgical, anaesthetic/intensive therapy unit (ITU) or GP registrars.
Some of this workload is due to increasing admissions, some due to the unwillingness or inability of other specialties to manage patients, and some due to the four-hour waiting time target resulting in less thorough assessment and management of patients in A&E. Also, other trainees are now less experienced but have more unwell patients under their care and so the medical registrar is more often called upon to assist with inpatient care. Compounding this, there is poor staffing out-of-hours, a constantly changing team and inadequate rest for registrars. Their roles are poorly defined, which means that they can be responsible for almost anything even if they lack adequate preparation or support. This leads to less time being available for training to be consultants. Training length has already been reduced due to Modernising Medical Careers and the European Working Time Directive.5,6 Training deficiencies are especially noticeable in management and leadership but also in clinical domains in new consultants in many specialties.7–10
As a consequence, there has been a marked change in the popularity of various medical specialties. Insufficient doctors are now applying for registrar training in specialties with a large contribution to (general) internal medicine, such as acute medicine or diabetes and endocrinology. For example, in 2011, 50% of consultant posts advertised in geriatric medicine were unfilled due to lack of applicants.11 By contrast, specialties perceived to have little future responsibility for (general) internal medicine have become much more popular. Dermatology was the most competitive medical specialty for ST3 recruitment in 2013. The resulting recruitment gaps mean medical registrar rotas are becoming unsustainable and more difficult to manage.
The supply of future medical registrars and consultants comes from those in core medical training. Core medical training may lead into other specialties such as radiology, intensive care, emergency medicine or general practice, but it is essential that a large proportion of trainees continue to higher medical training to avoid shortfalls in medical specialties. Not only must they be well trained but training must lead to an enthusiasm and excitement about a long-term future career as a physician. Sadly both recent anecdote and a subsequent survey by the JRCPTB suggest that the pressure of service change is also having a significant negative impact on core medical trainees. Indeed the JRCPTB survey suggested ‘a picture of hardworking doctors feeling they are overwhelmed by service work, unrecognised and unsupported by their employers… harassed and hardworking supervisors with very little acknowledgement of the training nature and requirement of their post. About half do not feel ready to progress to the next training level’ (B Burr, personal communication). An earlier survey found that 10% of CT2 trainees had never managed acute myocardial infarction and 11% had not managed diabetic ketoacidosis.12 They also had less experience of practical procedures, with only a minority of CT2 trainees being able to perform them independently: 28% for DC cardioversion, 33% for intercostal chest drain and 42% for non-invasive ventilation.
So the evidence from physicianly trainees is that the current service model is undermining their training and that there are not enough doctors with the right skills to meet the service pressures. The experience of core medical trainees and medical registrars should not come as a surprise. The RCP highlighted the problems early last year in its document, Hospitals on the edge? The time for action, which in turn stimulated the Future Hospital Commission's priorities and recommendations.13 It reported that the pressures on the acute medicine service ‘are relentless and intense’. The key factors are the increasing clinical demand and in particular, the changing patients and their changing needs. Over a decade, there has been a 37% increase in emergency admissions, with a reduction in hospital bed numbers. Patients are older and those admitted to hospital have an increasing number of chronic illnesses. This pressure has to be put in the context of the success of medicine in some areas, particularly the success of physician specialists in dealing with single organ pathology. For example, stroke care has improved dramatically with the introduction of stroke units, direct access to specialists, faster times to thrombolysis and constant evaluation by the RCP's Sentinel Stroke National Audit Programme.14 The same is true for myocardial infarction and upper gastrointestinal bleeding. While the evidence is unequivocal that many patients have benefited from specialisation and expertise in a single condition, this also leads to fractured, fragmented, uncoordinated care from a patient's perspective. Specialists may ignore or not manage co-morbidities and the increasing numbers of patients with multiple conditions may not know who their consultant is.
Recommendations of the Future Hospital Commission
All the evidence and challenges set out above were considered by the Future Hospital Commission. Not surprisingly, it makes significant recommendations for medical education and training to support the current and future needs of patients and the model of care set out within the Commission's report. Specifically, it requires ‘a cadre of doctors with the knowledge and expertise necessary to diagnose, manage and coordinate continuing care for an increasing number of patients with multiple and complex conditions.’1 This includes the expertise to manage older people with frailty and dementia. The National Institute for Health and Care Excellence (NICE), which has long produced respected guidelines for single conditions, is now also looking at producing guidelines for people with multiple co-morbidities after calls from researchers.15
The report emphasised that this will mean a change in the overall medical skill mix to allow for holistic and coordinated care while also ensuring timely access to highly specialised practitioners and procedures. In order to do this, it will be necessary to:
> train and deploy greater proportion of doctors to deliver expert, holistic care in (general) internal medicine
> valued and support the contribution of medical registrars in any new model.
In terms of medical education and training, the support required will include:
> in the short-term, an expansion of training opportunities in acute and (general) internal medicine
> much greater emphasis on acute and (general) internal medicine, starting at undergraduate level
> an increase in the length of broad-based training programmes and early training (pre-ST3) to include acute and (general) internal medicine and aspects of community care
> increased participation in service provision in acute and (general) internal medicine for all medical specialties
> a strong focus on improving non-core skills and in particular an understanding of what clinical leadership means for all doctors
> in the future, a possible remodelled training pathway in which all trainees focus on acute or (general) internal medicine before further specialisation occurs.
But these expectations for change in the education and training of physicians do not occur in a vacuum. Although some immediate change is needed to support the service and the pressure on current registrars, this must only be considered a transition to the whole system change envisaged in the full report. In delivering a new model of seven-day care with continuity of clinical teams that provide the most expert and appropriate care for patients at all stages of their journey, fundamental change is required in many hospitals. The model of a single ‘take’ day with a wide distribution of patients must change to the model described by the Future Hospital Commission. There needs to be a named consultant, who spends longer blocks of time in (general) internal medicine alongside trainees to provide the continuity of care and a team-based approach to (general) internal medicine. Stable teams of physicians supporting the acute care hub should work there for between three and seven days. Trainees themselves may have longer blocks of time in the acute care hub with separate dedicated blocks of time providing other inpatient ward support and for specialty training.
Preliminary evidence that this does improve satisfaction for physicianly trainees and improve training has been produced through a pilot scheme under Health Education England's Better Training Better Care initiative – which also found that there was improvement in the care of patients at weekends.16 Simply having a longer period of continuity and responsibility leads to more interest in (general) internal medicine and gives feedback on outcomes (such as on post-take ward rounds), so vital to learning but increasingly difficult to achieve in the current fragmented system.
The Shape of Training Review
At the same time as the Future Hospital Commission was reviewing medical training, a national group (comprising the four countries of the UK), led by the GMC but also including the four departments of health, the Academy of the Medical Royal Colleges, Health Education England, the Medical Schools Council and the Confederation of Postgraduate Deans, was reviewing all postgraduate medical training in the UK. Their final recommendations were published in October 2013.2 Not surprisingly it found many of the same service challenges and therefore problems with training that were identified for physicians by the Future Hospital Commission.
Some of the key messages included:
> Patients and the public need more doctors who are capable of providing general care in broad specialties across a range of different settings. This is being driven by a growing number of people with multiple co-morbidities, an ageing population, health inequalities and increasing expectations.
> Postgraduate training needs to adapt to prepare medical graduates to deliver safe and effective general care in broad specialties.
> Medicine has to be a sustainable career with opportunities for doctors to change roles and specialties throughout their career. Doctors in academic training pathways need a training structure that is more flexible.
> We will continue to need doctors who are trained in more specialist areas.
These themes resonate strongly with some of the findings and recommendations of the Future Hospital Commission, although the Shape of Training is about all doctors and not just physicians. A caveat is that the Shape of Training is a very high-level document, which sets out themes rather than specific training pathways. Those themes include the vision that training does not stop at a certificate of completion of training (CCT). Although there will be a certificate of specialty training (CST), there is an expectation that many, if not all, doctors will continue formal education and training, as opposed to CPD, throughout their career. This is a new and quite radical concept in the UK. The document is clear that we need more doctors providing ‘general’ care in broad specialties, but it is also clear that we will still need specialists. In addition, it says that regulators must make a reality of the career flexibility that is so often talked about but still seems so difficult to achieve in practice.
As expected, such a radical change is proving controversial. It is such a high-level document that there remain many completely unresolved questions, including:
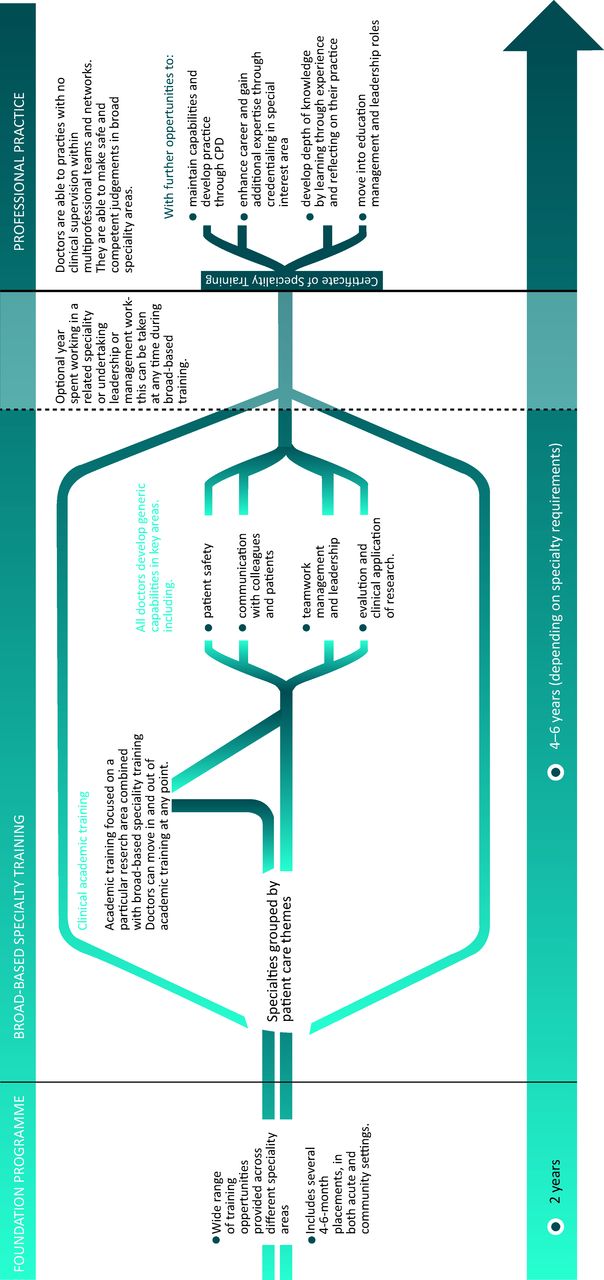
> There are now only 6 years of training available up to a CST (Fig 1) but what does this mean for current 7 year pathways? Some believe this is simply a cost saving plan.
Fig 1.Post-graduation training pathway overview proposed by Shape of Training review. Adapted from Securing the future of excellent patient care – the final report of the Shape of Training Review.2
> Improving the training and status of (general) internal medicine is widely supported, but it is recognised to be complex and the more training that is done in internal medicine, the less time there is for other training prior to CST.
> As described earlier, there is a very clear evidence base for specialist care of single conditions and often a public expectation that they must see the best specialist for their current condition.
> The model seems likely to require more physicians in total to provide both generalist and adequate specialist cover. Is this affordable for the health service?

At the heart of the Shape of Training, though, is the expectation that the training of doctors must meet the needs of patients more successfully than is currently the case. This chimes exactly with the drivers and the findings behind the Future Hospital Commission's report.
Next steps
The Future Hospital Commission presents a radical but achievable vision of the reform of hospital services to meet the patients’ needs. It recognises the current challenge and tension between service provision and training and wants to see urgent action. In particular, as soon as possible, in going forward all physicianly trainees should expect to both participate in (general) internal medicine as well as formally train in (general) internal medicine, to dilute the present overwhelming workload and thereby improve patient care. However, the RCP is clear that these changes must not take place without the reforms of the acute care hub and a stable team to provide an appropriate and supportive environment for all trainees undertaking training in (general) internal medicine. The two changes need to happen together.
The Shape of Training Review recognises the same challenges as the Future Hospital Commission but has a medium to longer term vision, with a 5–10 year implementation timetable. Thus the Shape of Training Review timeframe is not a reason to delay acting upon the recommendations of the Future Hospital Commission, and indeed the review will need substantial discussion and further work to develop a long-term sustainable model that has the necessary support of the medical profession. Possibly the most fundamental recommendation is around what a CST means and how training will occur post-CST rather than pre-CCT currently. The RCP has strongly argued that getting this right will underpin other changes in the Shape of Training Review and we believe that specialty training post-CST must be nationally planned, nationally funded and assessed to a national standard.
Without such a model being in place, it is unlikely that support from current trainees or consultants towards a more generalist CST will be forthcoming. As both of these documents make very clear, generalist expertise is needed as much as specialist expertise. There must be a guaranteed route to achieve both. The JRCPTB has recently started pilots of Post-CCT Fellowships, but this is a long way from becoming a national system of CST credentialing.17 This area of work should be the main starting point for the Shape of Training.
Seeing the reality of post-CST credentialing will then lead into a much more informed discussion about the aims, curriculum and delivery mechanisms in the six years of training between Foundation and a CST. We simply do not know whether the model will be a CST in internal medicine or a CST in internal medicine with a theme (such as cardiology), or even whether for a small number there would be the option of CSTs without any internal medicine but with the risk of future career inflexibility. The detail is certainly not present but there is no doubt about the willingness to debate and discuss the flexibility needed to ensure we provide the doctors that future patients need. The current status of the Shape of Training is that this is the end of the beginning and not the beginning of the end.
Conclusions
We, as physicians, are doing more and more for our patients. There is wide agreement that the current hospital model does not work effectively or efficiently and we are struggling to meet the changing and complex clinical needs of patients. This is putting increasing pressure not just on consultants but on those training to be physicians and crucially on their wish to be a physician in the current model. The Future Hospital Commission set outs vital changes in the model of delivery but also expectations both for the short term and the medium term in how we should be training our doctors to support current trainees in patient care.
The publication of both documents has started an intense debate among physicians and is certainly challenging the status quo. The balance between specialism and generalism must be resolved but the work of the Future Hospital Commission suggests that this requires radical change in how we provide care, not just in training. We certainly do not know the financial and workforce implications of the proposed models. Belatedly, physicians are only just beginning to decide how to reinvent and reinvigorate general (internal) medicine to make it an attractive high status career pathway. Just as vitally, maintaining the attractiveness and training requirements of specialist careers will only happen if post-CST credentialing is properly planned and shown to work at an early stage.
The Shape of Training Review recognises all these challenges not just for physicians but for other specialties and provides one long-term vision for a more flexible training programme to meet health service and patient needs. While there is much similarity in the principles behind the educational statements in the Future Hospital Commission and the Shape of Training Review, the Future Hospital Commission is based in the here and now and trying to help and support the current crisis. The Shape of Training is a much longer term vision and one that physicians will expect to shape in the coming years.
- © 2014 Royal College of Physicians








{kind=link}