Article Text

Abstract
Objective: A double blind, randomised, placebo controlled study to evaluate the safety and efficacy of etanercept to treat adult patients with ankylosing spondylitis (AS).
Methods: Adult patients with AS at 14 European sites were randomly assigned to 25 mg injections of etanercept or placebo twice weekly for 12 weeks. The primary efficacy end point was an improvement of at least 20% in patient reported symptoms, based on the multicomponent Assessments in Ankylosing Spondylitis (ASAS) response criteria (ASAS 20). Secondary end points included ASAS 50 and ASAS 70 responses and improved scores on individual components of ASAS, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), acute phase reactants, and spinal mobility tests. Safety was evaluated during scheduled visits.
Results: Of 84 patients enrolled, 45 received etanercept and 39 received placebo. Significantly more etanercept patients than placebo patients responded at the ASAS 20 level as early as week 2, and sustained differences were evident up to week 12. Significantly more etanercept patients reported ASAS 50 responses at all times and ASAS 70 responses at weeks 2, 4, and 8; reported lower composite and fatigue BASDAI scores; had lower acute phase reactant levels; and had improved spinal flexion. Etanercept was well tolerated. Most adverse events were mild to moderate; the only between-group difference was injection site reactions, which occurred significantly more often in etanercept patients.
Conclusions: Etanercept is a well tolerated and effective treatment for reducing clinical symptoms and signs of AS.
- AS, ankylosing spondylitis
- ASAS, Assessments in Ankylosing Spondylitis
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ESR, erythrocyte sedimentation rate
- NSAIDs, non-steroidal anti-inflammatory drugs
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- TNFα, tumour necrosis factor α
- VAS, visual analogue scale
- ankylosing spondylitis
- etanercept
- tumour necrosis factor inhibitors
- biological treatment
Statistics from Altmetric.com
- AS, ankylosing spondylitis
- ASAS, Assessments in Ankylosing Spondylitis
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ESR, erythrocyte sedimentation rate
- NSAIDs, non-steroidal anti-inflammatory drugs
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- TNFα, tumour necrosis factor α
- VAS, visual analogue scale
Ankylosing spondylitis (AS) is an underrecognised, debilitating disease predominantly affecting the spine that is characterised by axial skeletal ankylosis and inflammation at the insertions of tendons. The prevalence of AS is most clearly described in the white population where a link to the HLA-B27 antigen is best defined, and is believed to be around 0.5%, with estimates ranging from 0.1% to 1.1%.1 Peripheral joints also may be affected. The disease occurs three times more often in men than in women,2 and onset typically occurs between 20 and 40 years of age. Although AS advances slowly, damage to the spine is progressive and leads to pain, fatigue, stiffness, and functional impairment. Patients with AS often have a restricted or poor quality of life and may face a reduced life expectancy.3–8 The socioeconomic burden of their disease can be considerable, owing to work disabilities and the use of healthcare/assistance resources, and sometimes to the patient’s depressed mood or low social functioning.1,9–13 Current therapeutic options for AS, such as non-steroidal anti-inflammatory drugs (NSAIDs), offer temporary pain relief but confer little if any clinical benefit on spinal mobility. Disease modifying antirheumatic drugs (DMARDs), including methotrexate and sulfasalazine, may benefit peripheral arthritis but do not appear to affect the spinal involvement of AS.14–17
Tumour necrosis factor (TNF) α (TNFα), is a proinflammatory cytokine that appears to have a key role in the pathogenesis of AS.12,18–22 Etanercept is a fully human recombinant protein, comprising two molecules of soluble TNF receptor p75 and the crystallisable fragment component of immunoglobulin G1, which specifically binds to and neutralises TNFα.23,24 Etanercept is effective in the treatment of other TNF related diseases, including rheumatoid arthritis (RA), juvenile chronic arthritis, and psoriatic arthritis (PsA).25–27 More recently, a phase 2 clinical study has shown that etanercept reduces disease activity in patients with spondyloarthropathies, including reactive arthritis and AS.28–31 Similar results have been reported with infliximab, a chimeric monoclonal antibody against TNFα.32,33
The current double blind, randomised, multicentre European trial examined the efficacy of etanercept to treat AS in adults, using the recently published criteria of an international consortium of experts, the Assessments in Ankylosing Spondylitis (ASAS) Working Group.34 Previous etanercept trials in AS have been conducted at both North American and European investigative sites. This study is the first conducted exclusively at European centres. Because there are potentially important differences between populations studied and in the way patients are treated in different geographical locations, it was important to this study to confirm the results of a multinational study of etanercept that was conducted concurrently.35 These trials are the first studies performed with anti-TNF biological agents using the ASAS response criteria as the primary end points.
PATIENTS AND METHODS
Study design
A double blind, randomised, placebo controlled study was conducted to evaluate the efficacy and safety of etanercept in the treatment of adult patients with active AS. The study took place from March 2002 to August 2002 in 14 investigative centres in eight countries: Belgium, Finland, France, Germany, Italy, The Netherlands, Spain, and the United Kingdom. All centres received approval from their independent ethics committees, and all patients provided written informed consent to participate. The study included a screening period of up to 4 weeks, followed by a 12 week treatment period in which patients received etanercept or placebo. Efficacy and safety evaluations were performed at weeks 2, 4, 8, and 12.
Patients
Patients aged 18–70 years with active AS were eligible for the study. AS was diagnosed using the modified New York criteria.36 Disease activity was measured using a set of visual analogue scales (VAS) on which patients rated the severity of their symptoms from 0 (none) to 100 (most severe) in four symptom domains: (a) spinal inflammation; (b) back pain; (c) patient global assessment of disease activity; and (d) physical function. Active disease was diagnosed if the patient had an average score ⩾30 for spinal inflammation and a score ⩾30 on at least two of the other three domains.
Patients were excluded if they had complete ankylosis (fusion) of the spine; previously used TNFα inhibitors, including etanercept; used DMARDs other than hydroxychloroquine, sulfasalazine, or methotrexate within 4 weeks of baseline; used multiple NSAIDs; used >10 mg prednisone daily; or changed doses of NSAIDs or prednisone within 2 weeks of baseline. Patients were permitted to continue prestudy physiotherapy.
Patients who met eligibility criteria were stratified on the basis of concomitant DMARD use at baseline and randomly assigned to receive etanercept or placebo. The protocol did not require screening for tuberculosis.
Study product
Based on previous clinical trials of etanercept in patients with RA and PsA, a 25 mg dose delivered subcutaneously twice weekly was selected for patients with AS. Patients self administered the product and were given individual packages containing injection supplies and instructions for storage and use. To preserve the integrity of the blind study, placebo and etanercept supplies were similar in appearance.
Efficacy end points
The clinical response to etanercept was evaluated chiefly on the basis of response criteria recommended by the ASAS Working Group,34 which covered the same four domains used in this study to assess disease activity at enrolment—that is, spinal inflammation, back pain, patient global assessment, and physical impairment. Spinal inflammation was scored as the average of two VAS questions about the duration and intensity of morning stiffness, taken from the previously validated six item Bath Ankylosing Spondylitis Disease Activity Index (BASDAI).37 Pain was scored as the average of two VAS questions about total back pain and nocturnal back pain. Patient global assessment was measured by VAS. Functional impairment was assessed by the 10 item Bath Ankylosing Spondylitis Functional Index (BASFI), a validated VAS based composite of functional ability in patients with AS.38 Table 1 shows details of the BASDAI and BASFI indexes and other efficacy end points.
Efficacy end points used to assess etanercept
The primary efficacy end point was the percentage of ASAS 20 responders after 12 weeks of treatment. ASAS 20 responders were patients who reported improvements of at least 20% and absolute improvement of at least 10 units in at least three of the four symptom domains, with no worsening in the remaining domain. Secondary end points included the percentage of ASAS 20 responders at weeks 2, 4, and 8; the percentage of patients improving 50% or more (ASAS 50) at any visit; and the percentage improving 70% or more (ASAS 70) at any visit. ASAS 50 and 70 responses also required improvement in at least three domains and no deterioration in the remaining domain. Other patient reported end points consisted of symptom improvements in individual ASAS domains and improvements on the composite BASDAI and its individual components. Effects on acute phase reactants were measured by tests for C reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Effects on spinal mobility were measured by Schober’s test, chest expansion, and occiput to wall distance.
Safety analyses
Patients were monitored for adverse events and abnormal laboratory test results over the course of the study. Vital signs were monitored, and standard haematology, serum chemistry, and urine analysis tests were evaluated. In addition, blood samples were tested for antibody to etanercept at baseline and at week 12, using an enzyme linked immunosorbent assay (ELISA) modified from the method published earlier.39
Statistics
Disease activity and safety analyses were based on the intention to treat population and included all patients who received at least one dose of the “blinded” test article. The last observation carried forward technique was used to handle missing data for continuous and ordinal end points. Patients who withdrew from the study prematurely were treated as non-responders at each assessment interval thereafter for ASAS and other patient reported responses. All statistical tests were two sided. The Cochrane-Mantel-Haenszel test, stratified by baseline DMARD use, was used to evaluate efficacy differences between the etanercept and placebo groups, and χ2 and Breslow-Day tests were used to evaluate direct and interactive effects of DMARDs on ASAS responses. For safety analyses, Fisher’s exact test was used to compare the percentage of adverse events occurring in etanercept and placebo treated groups. Based on a previous trial, week 12 response rates of 35% in the placebo group and 75% in the etanercept group were expected. Assuming similar response rates, this study design provided 90% power with 40 patients in each group.
RESULTS
Study objective
This study was conducted to evaluated the safety and efficacy of etanercept to treat adult patients with AS.
Patient recruitment and retention
A total of 84 patients were enrolled in the study; 45 were assigned to receive etanercept and 39 were assigned to placebo. The average age of patients was 43.2 years. Most participants were male (79%), and the majority were white (94%). The treatment groups had similar baseline disease activity scores and concomitant use of DMARDs, NSAIDs, and corticosteroids. Demographic characteristics were largely similar, except that etanercept patients were, on average, 5 years older than placebo patients, had had AS disease for 5 years longer (table 2), and also had significantly higher baseline CRP levels (see table 4).
Baseline demographic and descriptive characteristics
Two patients treated with etanercept discontinued the study for non-safety reasons. The first patient discontinued after a single dose of etanercept because he did not meet the inclusion criterion of active disease, and the second patient withdrew his consent 8 days after treatment was started. Both patients were treated as non-responders at subsequent times. The remaining 82 patients completed the study.
Efficacy results
Significantly more etanercept patients than placebo patients (26 (60%) v 9 (23%); p<0.001; 95% confidence interval (CI) 17.4 to 56.4%) were ASAS 20 responders at week 12, the primary efficacy end point. The primary end point was not significantly affected by the concomitant use of DMARDs (p = 0.632), nor was there an interaction effect between DMARDs and etanercept on ASAS 20 at week 12 (p = 0.694).
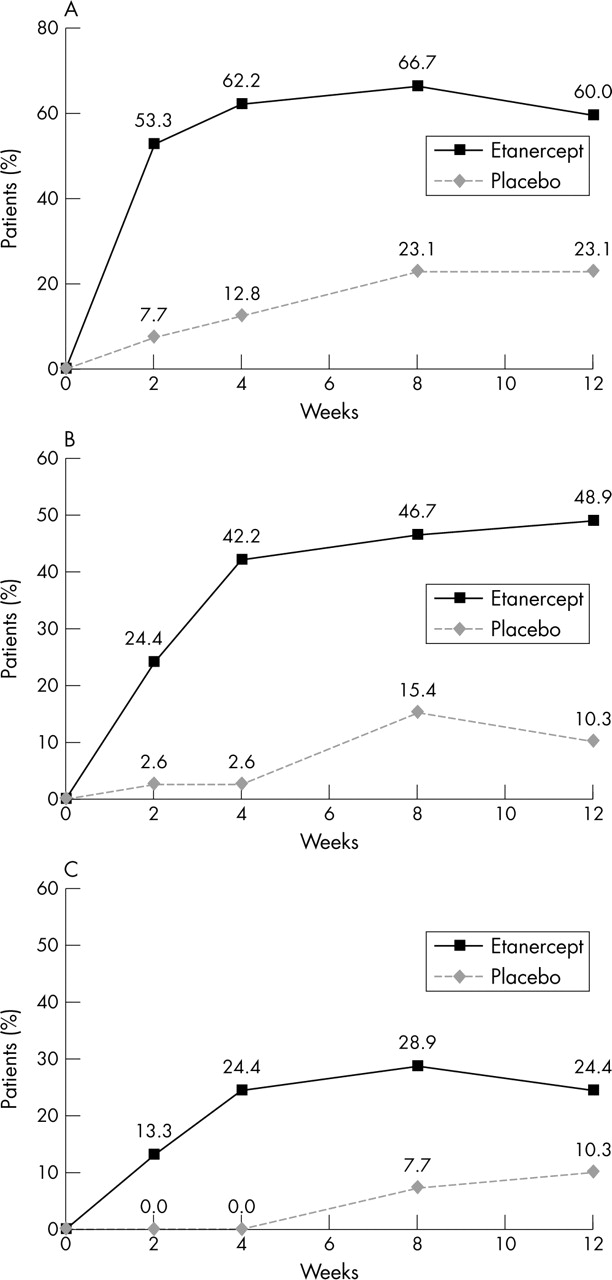
Significant improvements in the etanercept group were evident by week 2, the earliest assessment point, and were sustained thereafter (fig 1A). There were also significantly more responders in the etanercept group at the ASAS 50 level at all visits (p<0.01) and at the ASAS 70 level at weeks 2, 4, and 8 (p<0.05) (figs 1B and C). By week 12, nearly half of the patients treated with etanercept improved 50% or more on the ASAS criteria, and a quarter of them improved 70% or more.

(A) Achievement of ASAS 20, by treatment group; (B) achievement of ASAS 50, by treatment group; (C) achievement of ASAS 70, by treatment group.
ASAS responses used in this study were based on the average of total and nocturnal back pain. The ASAS Working Group criteria, published after plans for this study were completed, recommended using VAS for total back pain only. Sensitivity analyses using total pain scores alone confirmed nearly identical results to those reported here.
In addition to improved responses on the overall ASAS criteria, etanercept patients significantly improved their mean scores on the individual ASAS components (p<0.01 versus placebo). Scores of etanercept patients improved 43% on both the spinal inflammation and back pain measures, 37% on patient global assessment of disease activity, and 35% on the functional impairment index (compared with 16%, 6%, 13%, and 3% improvements, respectively, for placebo patients; table 3). Although scores on individual components of the BASFI are not provided in this paper, etanercept was significantly more effective than placebo in improving nine of 10 types of functional abilities.
Comparison of ASAS and BASDAI Scores before and after 12 weeks of treatment
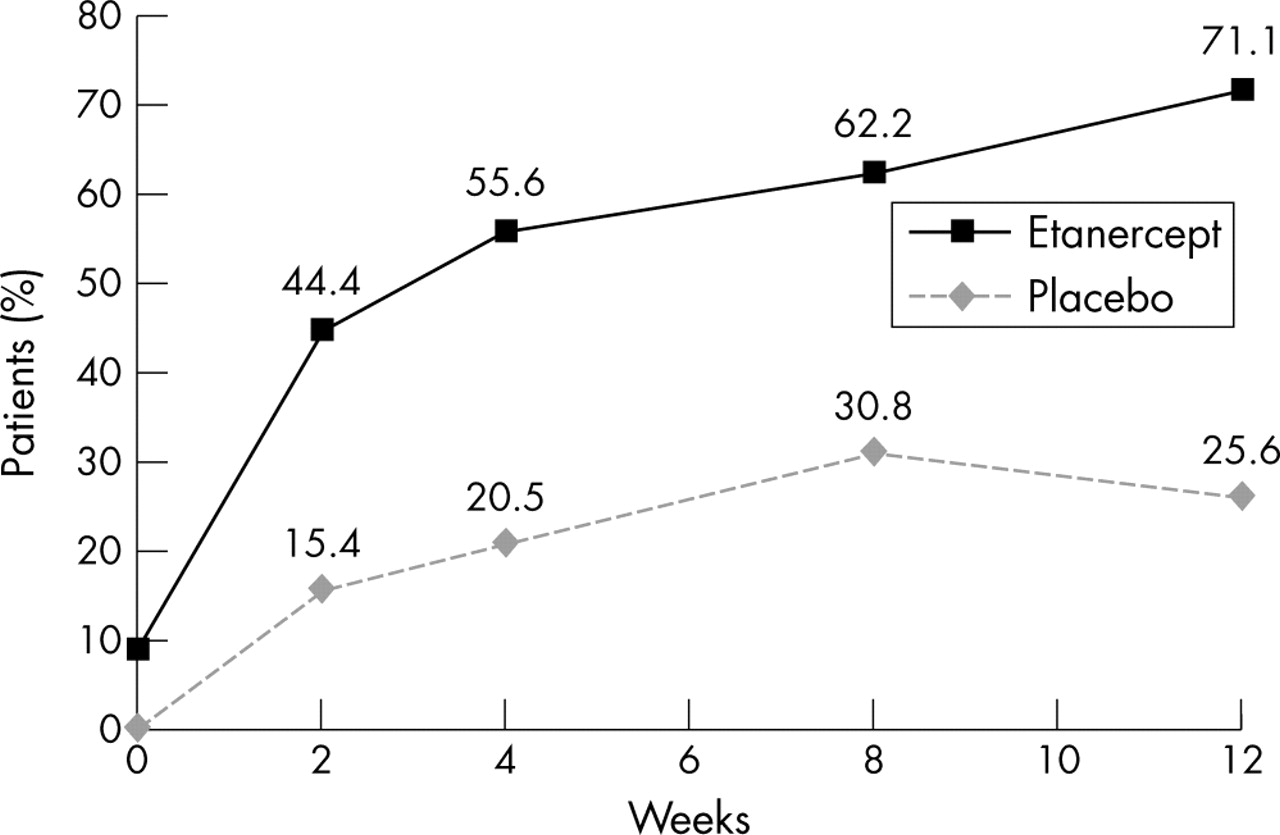
Scores on the BASDAI composite index and the BASDAI fatigue component improved 44% among etanercept patients (p<0.01 versus placebo). In addition, a post hoc analysis of BASDAI responses showed that the percentage of etanercept patients with BASDAI scores <40 increased from 9% at baseline to 71% at week 12 (fig 2).
{kind=link}
{kind=link}
Percentage of patients with BASDAI scores <40.
Acute phase reactants, CRP and ESR, also significantly decreased in etanercept patients (p<0.0001), with percentage changes of 70% and 80%, respectively (table 4). Spinal flexion, as measured by Schober’s test, improved in etanercept treated patients but not in placebo patients (p<0.01). Other measures of spinal mobility also improved more in etanercept patients, but the differences were not significant.
Comparison of acute phase reactants and spinal mobility values before and after 12 weeks of treatment
Patients in this trial had limited peripheral joint disease. Numbers of swollen and tender joints were 2 and 6, respectively, for the entire group. Given the paucity of this information, no meaningful results on peripheral joint disease were obtained.
Safety results
Etanercept treatment was generally well tolerated. Adverse events were mostly mild to moderate, and there were no discontinuations for safety reasons. Treatment-emergent adverse events reported by 5% or more of patients in either treatment group were generally similar (table 5). As in previous studies of etanercept, injection site reactions occurred significantly more often in etanercept patients (33%) than in patients receiving placebo (15%, p<0.05). No antibodies to etanercept were detected.
Number (%) of patients with treatment emergent adverse events or infections (occurring in ⩾5% of patients in either treatment group)
One serious adverse event was reported. An etanercept treated patient with acute myocardial infarction underwent angioplasty but continued in the study. The same patient developed grade 3 abnormality of liver function test results at the week 12 visit, which was considered to be related to concomitant indometacin treatment. The abnormalities resolved after indometacin was discontinued, and the patient completed the study.
DISCUSSION
AS is a chronic inflammatory disease, often leading to permanent spinal damage, a considerable handicap, and a poor quality of life. Current treatments for AS are inadequate for most patients, especially treatments for axial skeletal involvement.
In this 12 week study, twice weekly self administered injections of 25 mg etanercept produced rapid, significant, and sustained improvement in multiple clinical and biological measures of AS, regardless of concomitant DMARD use. Patient improvements were evident at the 2 week visit and were sustained up to the end of the study at week 12. Notably, the only differences between the groups at baseline were that etanercept patients were on average 5 years older, had had AS for 5 years longer than patients receiving placebo, and had higher baseline CRP levels. Given the magnitude of the etanercept treatment response in this study, it is unlikely that these baseline differences affected the results in any significant way. Furthermore, in light of recent analyses indicating that older patients and patients with longer disease duration are less likely to have a major clinical response to TNFα inhibitors,40,41 this group’s demonstrable response to etanercept is particularly encouraging.
The finding of multiple positive effects in this study of European patients supports the results of two other efficacy and safety studies of etanercept to treat AS. The first was a 16 week American study, which showed that etanercept was efficacious in the treatment of many symptoms reported by patients with AS, including pain, vitality, and physical function.28 The second was a 24 week multinational study that was conducted concurrently with the present study and included similar end points.35 When the ASAS benchmarks of 20%, 50%, and 70% improvement were used, both the current study and the 24 week study found that etanercept treatment was significantly better than placebo, with robust improvements occurring as early as week 2.
Treatment with etanercept also improved BASDAI scores; by week 12, 71% of etanercept treated patients achieved BASDAI scores <40, which the ASAS Working Group considers as the threshold value indicating a need for anti-TNFα treatment.42 Moreover, fatigue scores, which are felt to be an important outcome in AS, improved significantly with etanercept treatment.43 Because fatigue is associated not only with disease activity and functional ability but also with patients’ global sense of wellbeing and mental health status,44 improvement in this area may lead to a better quality of life for patients with AS.
In the current study, CRP levels and ESR values significantly decreased in patients taking etanercept, which may be indicative of disease modification, not just symptomatic relief of AS.45–48 Spinal mobility, as measured by Schober’s test, significantly improved in etanercept treated patients, which suggests that damage caused by AS may not be permanent. The lack of significant between-group differences in chest expansion and occiput to wall distances at the end of treatment may be due to the short duration of the study and/or the relatively small number of patients enrolled. In the 24 week study mentioned earlier, which enrolled more patients, all three spinal mobility measures significantly improved with etanercept treatment.35 Owing to the short duration of this trial, the impressive therapeutic results must interpreted with some caution. None the less, the relative ineffectiveness of current treatments such as DMARDs and NSAIDs is underlined by the fact that etanercept treated patients who continued to receive these treatments enjoyed no apparent efficacious advantage over those who were not receiving these drugs.
The efficacy results are also consistent with those reported for infliximab33,49; however, no antibodies to etanercept were found in this study. The lack of etanercept immunogenicity in this trial might be explained by the trial’s brevity, and the frequency of etanercept antibodies after long term treatment in patients with AS is unknown. It is noteworthy, however, that in etanercept trials of up to 2 years in patients with RA, the level of etanercept antibody reactivity has been reported to be around 3%.50,51 Additionally, these results contrast with the recent finding of a study of infliximab to treat Crohn’s disease, in which 61% of patients produced antibodies to infliximab after a mean of 3.9 infusions of 5 mg/kg over a mean of 10 months. In the latter study, antibody concentrations ⩾8.0 μg/ml significantly reduced serum concentrations of infliximab, which in turn significantly decreased the duration of treatment response.52
Etanercept was well tolerated in adult patients with AS. Although approximately one third of patients had injection site reactions, no serious infections occurred, and no patients withdrew because of these reactions or other adverse events. Etanercept’s safety profile was similar to that seen in patients with RA and PsA. Although pharmacokinetic measures from the current study are not shown in this article, a separate analysis of clearance and steady state trough concentrations showed that etanercept’s pharmacokinetic profile in patients with AS was similar to that in patients with RA53; thus, it appears that the disposition of etanercept is unaltered by the AS disease state.
As noted above the socioeconomic burden of AS can be considerable. Thus, the relatively higher cost of etanercept treatment compared with less efficacious treatments should be weighed against the costs of AS disease.
In summary, etanercept produced a rapid and sustained reduction of the clinical signs and symptoms of AS. Given these results, further investigation of longer term treatment with etanercept is warranted to further define its therapeutic utility. The use of imaging tools also is warranted to investigate the effects of etanercept on spinal disease, and such tests may shed light on whether etanercept can halt the progression of AS.
Acknowledgments
This trial was funded by Wyeth Research.
Ron Pedersen, an employee of Wyeth, is acknowledged for his study design advice and statistical analysis. Susan Coyle, an employee of Wyeth, is acknowledged for her writing support.
REFERENCES
Footnotes
-
Presented in part at the Annual European Congress of Rheumatology in Lisbon, Portugal, June 2003.