Article Text

Abstract
Objectives To compare the incidence of serious infection (SI) across biologic drugs used to treat rheumatoid arthritis (RA) using data from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis (BSRBR-RA).
Methods The BSRBR-RA is a prospective observational cohort study. This analysis included patients with RA starting a new biologic. The primary outcome was SI defined as an infectious event requiring admission to hospital, intravenous antibiotics or resulting in death. Event rates were calculated and compared across biologics using Cox proportional hazards with adjustment for potential confounders. Secondary outcomes were the rate of infection by organ class and 30-day mortality following infection.
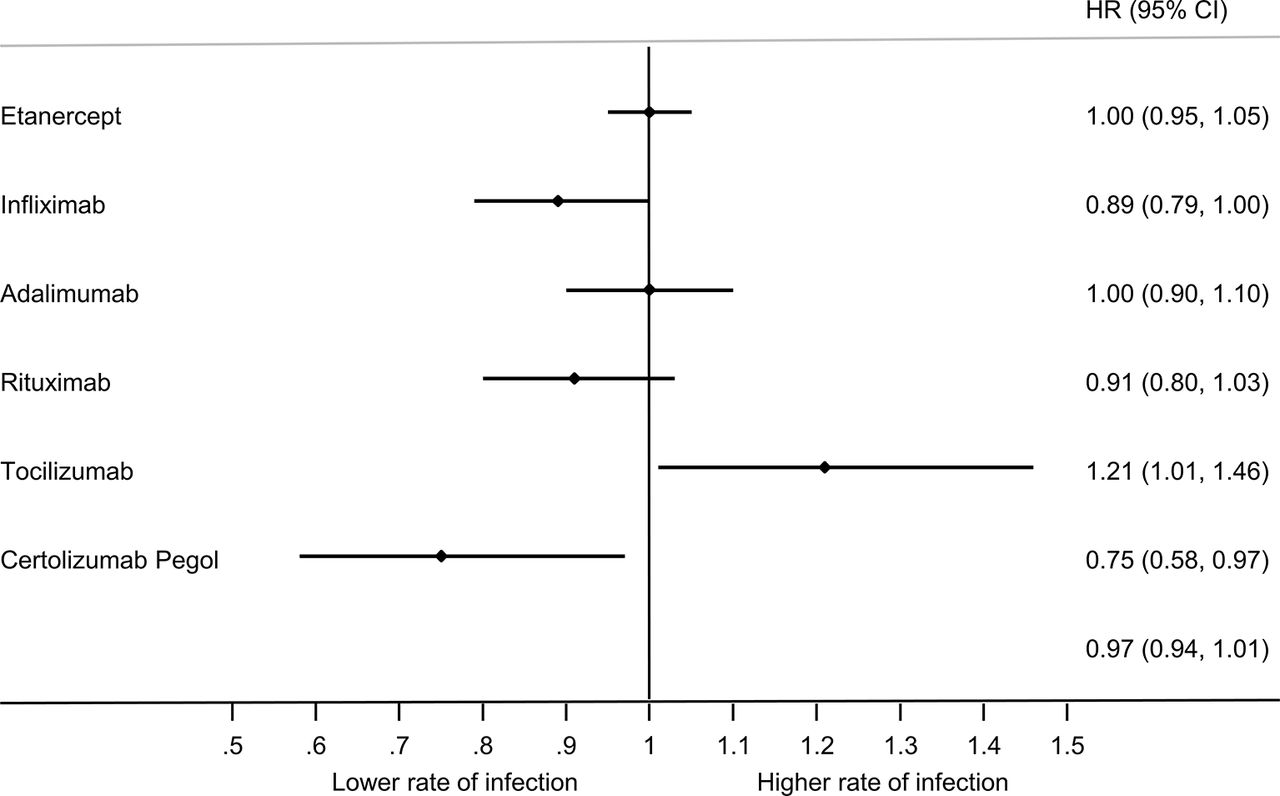
Results This analysis included 19 282 patients with 46 771 years of follow-up. The incidence of SI was 5.51 cases per 100 patient years for the entire cohort (95% CI 5.29 to 5.71). Compared with etanercept, tocilizumab had a higher risk of SI (HR 1.22, 95% CI 1.02 to 1.47) and certolizumab pegol a lower risk of SI (HR 0.75, 95% CI 0.58 to 0.97) in the fully adjusted model. The 30-day mortality following SI was 10.4% (95% CI 9.2% to 11.6%).
Conclusions The rate of SI was lower with certolizumab pegol than etanercept in the primary analysis but the result was no longer significant in several sensitivity analyses performed suggesting residual confounding may account for the observed difference. From these results, it would be wrong to conclude that certolizumab pegol has a lower rate of SI than other biologics; however, the risk does not appear to be significantly higher as has previously been suggested.
- rheumatoid arthritis
- infections
- dmards (biologic)
- epidemiology
Statistics from Altmetric.com
Background
Infection represents a substantial source of both morbidity and mortality for patients with rheumatoid arthritis (RA). A recent real world study of UK patients with RA reported that 8% require hospital admission each year due to serious infection (SI).1 The predictors of infection in RA include patient factors (older age, concomitant illness), disease-specific factors (level of disease activity and disability) and immunosuppression. Conventional synthetic disease-modifying anti-rheumatic drugs (cs-DMARDs) in RA have relatively little impact on infection risk; however, corticosteroid exposure appears to be an important predictor of infection.2 3
Anti-TNF therapy is associated with an increased rate of SI when compared with cs-DMARD therapy with the risk greatest during the first 6–12 months of therapy.4–6 The infection risk with other biologics acting through different mechanisms in RA is less well established. One would hypothesise that biologic drugs acting on different cellular and cytokine targets would have a different pattern and rate of SI associated with them.
There are few head to head clinical trials between biologic therapies in RA. Those studies that do exist understandably focus on efficacy as their primary endpoint. While safety data are often included, the studies are not powered to detect significant differences in the rate and pattern of infection seen.
A large network meta-analysis of biologics found that the incidence of SI was comparable across biologic drugs used to treat RA with the exception of two drugs.7 Anakinra and certolizumab pegol were both found to have a significantly higher rate of SI than other biologics. However, a network meta-analysis relies on an indirect comparison between drugs and if there are differences in study design it can be prone to error. In contrast, national registers use the same methodology for detecting and reporting of adverse events for each drug.
Early work from the German RABBIT register showed that the incidence of SI with anti-TNF was approximately 6% per year but the population of people receiving biologics has changed over the past 15 years and these analyses need updating.8 There is a paucity of real world data on the infection risks associated with newer biologics such as tocilizumab. Results from a Japanese register showed no significant difference in the rate of SI with tocilizumab compared with anti-TNF therapy (HR 2.23, 95% CI 0.93, 5.37), but the CIs were wide and it is possible that the study was just underpowered to detect a difference.9
We set out to describe and compare the incidence and pattern of SI within the British Society for Rheumatology Biologics Register (BSRBR-RA) by biologic drug.
Methods
Data source
We used data from the BSRBR-RA, a prospective observational study established to evaluate the safety of biologics. The methodology has been described in detail previously.10 The inception of the register in 2001 was to meet national recommendations that all individuals with RA starting anti-TNF therapy should be enrolled in a postmarketing surveillance study. Initial biologic cohorts were for etanercept and infliximab users. Adalimumab, rituximab, tocilizumab and certolizumab-pegol cohorts have since been recruited. Abatacept received a European product license in 2007 but was not approved as a first-line biologic in the UK until 2012 and as such was not adopted into the BSRBR-RA.
Patient and physician questionnaires are returned every 6 months for the first 3 years and an annual physician questionnaire is completed thereafter. All adverse events are coded according to Medical Dictionary for Regulatory Activities (MedDRA) definitions. The BSRBR-RA is linked to the national death register meaning that the date and cause of death were available for individuals who died during the study period.
Drug exposure
This analysis included patients with RA starting a new biologic. Individuals were considered ‘at risk’ from treatment start for 3 years or until the date SI, three half-lives after drug cessation, death or last follow-up before June 2016, whichever came first. For the rituximab cohort, patients were considered ‘at risk’ until 270 days after the last infusion. If two infusions were separated by more than 270 days, the subject was considered to have been continuously ‘exposed’, reflecting the varying dosing frequency of rituximab. Biosimilars have been included in the register since 2015 but at the time of analysis there was insufficient follow-up data to include them in this study. Patients who switched therapy were allowed to contribute follow-up time to more than one cohort. All patients provided written informed consent.
Outcome
The primary outcome was any SI—defined as an infection resulting in death, hospitalisation or requiring intravenous antimicrobial therapy. Events could be identified in one of three ways: from patient questionnaires, physician questionnaires or death certificates. When identified by questionnaire, event of interest forms were sent to the patient and treating clinician to gather more information. Events were divided into seven categories based on organ class of infection (sepsis, lower respiratory, skin, gastrointestinal, bone/joint, genitourinary and other). The MedDRA codes for each category are shown in the online Supplementary figure 1. Secondary outcome measures were the organ class of infection and the 30-day mortality following serious infection.
Supplemental material
Statistical analysis
Event rates were calculated by dividing the number of SI by the time under observation for each drug with CIs calculated using a Poisson distribution. Rates were compared across biologics using Cox proportional hazards regression for time to first SI. Etanercept was chosen as the reference for comparison as it was the most widely used drug in the register. Potential confounders were identified a priori and adjustment was performed for age, gender, Disease Activity Score 28-erythrocyte sedimentation rate (DAS28-ESR), Health Assessment Score (HAQ), disease duration, smoking, seropositivity, polypharmacy and baseline steroid usage. Previous work with the BSRBR-RA has shown that polypharmacy is a good predictor of infections at a population level and can be used as a surrogate for comorbidity.11 Individuals were divided into three categories (0–5, 6–9 and >10) based on the number of medications they were taking excluding therapy for RA, and this category was used in the adjusted model. Multiple imputation of missing baseline variables was performed with 20 cycles using the ICE package in Stata V.14. Assumptions of the Cox model were tested graphically using Nelson-Aalen plots and with Schoenfeld residuals.
Sensitivity analyses
As the patient characteristics of those receiving biologics have changed since the inception of the register, a sensitivity analysis looking only at individuals starting a biologic from 2010 onwards was performed.
Confounding by indication is a major problem in observational studies that can be partially addressed using propensity scores (PS). A separate PS model was created for each treatment comparison using an inverse probability of treatment weights model. A single PS for each patient was calculated based on the following baseline covariates: age, gender, DAS28, HAQ, disease duration, seropositivity and non-biologic DMARD therapy. Further information on the PS model is available in the online Supplementary table 4.
Supplemental material
Patients starting their first biologic will have different disease characteristics compared with those who have failed on a previous biologic. Certain biologics tend only to be used as second or third line options and therefore comparing users of these drugs to new biologic users will be affected by channelling bias. A second sensitivity analysis was performed excluding those who were biologic naive, therefore, limiting only to individuals who have ‘failed’ at least one biologic agent.
A further sensitivity analysis was performed adjusting for individual comorbidities instead of polypharmacy. Comorbidities that predicted infection in a single variable model (diabetes, asthma and chronic obstructive pulmonary disease) were included in the multivariable model.
Previous studies have shown that the infection risk is greatest shortly after starting a new biologic. A sensitivity analysis was performed limiting to patients in their first year of follow-up in the register.
Results
A total of 19 282 individual patients were included in the analysis contributing 46 771 patient-years follow-up. The baseline characteristics of patients separated by drug therapy are shown in table 1. There were no missing data for age, gender or number of drugs. For the remaining covariates used in the adjusted analyses, there were less than 5% missing data.
Baseline demographics of the cohort
Incidence of serious infection
In total, 2606 events were classified as SI at a rate of 5.51 events per 100 patient years of follow-up (95% CI 5.29 to 5.71).
Etanercept was the largest cohort and was set as the reference group for other comparisons. In this cohort, the crude incidence of SI was 5.56 per 100 patient years (table 2). Three drugs had significantly different rates of SI compared with etanercept. These were rituximab, tocilizumab and certolizumab.
Incidence of serious infection by drug
Both rituximab (6.29 cases per 100 patient years) and tocilizumab (6.98 cases per 100 patient years) had a higher rate of infection than etanercept in the unadjusted model. In the adjusted model, rituximab no longer had an increased rate of SI (HR 0.91, 95% CI 0.80 to 1.03).
Certolizumab pegol had the lowest crude incidence of infection at 3.80 cases per 100 patient years. The rate was significantly lower than etanercept in both the unadjusted and fully adjusted model (table 2). The adjusted relative risks by drug is shown in figure 1.

Adjusted relative risk of infection by drug.
The results of the primary analysis were supported by the sensitivity analysis using propensity scores to adjust for potential confounding. Certolizumab was again found to have a significantly lower rate of SI, while tocilizumab had a higher rate of SI (see online Supplementary table 2). A sensitivity analysis limiting to new starters from 2010 found certolizumab still had a lower point estimate of serious infection rate but findings were no longer statistically significant in the fully adjusted model (HR 0.85, 95% CI 0.60 to 1.21).
Supplemental material
In the sensitivity analysis excluding biologic-naive patients, the rate of infection was comparable across the drugs with the exception of tocilizumab which had a higher incidence of SI than etanercept (HR 1.85, 95% CI 1.48 to 2.31). Full results for all the sensitivity analyses are shown in the online Supplementary table 2.
Infection by organ class
Respiratory infections accounted for 42% of all SI and were the most frequently recorded class of infection for all drugs in the register followed by soft tissue and skin infections (see online Supplementary figure 1). The incidence of serious infection by organ class for the entire cohort of biologic users is shown in figure 2.

{kind=link}
{kind=link}
Incidence of infection by organ class.
A full breakdown of the relative risk by drug class for each of the organ classes is shown in table 3. Etanercept had a comparatively low rate of respiratory tract infections at 1.81 cases per 100 patient years. This was significantly lower than adalimumab and tocilizumab in the fully adjusted model but not significantly different from the other drugs (table 3).
Adjusted relative risk of infection by organ class for each drug
Supplemental material
The rate of sepsis was significantly higher with rituximab than etanercept (HR 2.08, 95% CI 1.14 to 3.80). The reverse was seen when looking at skin infections with rituximab showing a significantly lower rate of events than etanercept (HR 0.54, 95% CI 0.39 to 0.75).
Adalimumab (HR 0.65, 95% CI 0.52 to 0.82) and certolizumab (HR 0.27, 95% CI 0.11 to 0.67) were associated with a significantly lower rate of skin infections than etanercept.
30-Day mortality by drug
The 30-day mortality following a serious infection for the whole cohort was 10.4% (95% CI 9.2% to 11.6%). The organ class of infection was a strong predictor of subsequent mortality. Sepsis/bacteraemia had the highest mortality at 45% (95% CI 33% to 61%) compared with just 2% (95% CI 1% to 3%) following skin infections. Sepsis remained a significant predictor of mortality in the fully adjusted model. The choice of biologic therapy was not a significant predictor of death following serious infection.
Conclusions
The rate of serious infection in this analysis was similar to that published in comparable cohorts of patients with RA treated with biologics.6 8 The pattern of infection was also similar to previously published work with respiratory infections the most frequently documented class of infection followed by skin and soft tissue infection.12 Small differences were observed between the drugs. It is important to appreciate the difference between relative and absolute risk when considering biologic choice. For patients whose baseline risk of infection is low, the choice of biologic will have very little impact on their subsequent infection risk. However, for patients with multiple risk factors who have a high baseline risk of infection, then choosing a drug with a slightly higher relative risk of infection can have a much larger impact on their infection risk.
In the unadjusted analysis, rituximab had a higher incidence of infection than etanercept but in the adjusted analysis the difference was no longer statistically significant. This suggests that patient factors as opposed to the drug itself were responsible for the observed difference. It is important to remember that drugs that are normally given second and third line are given to a different population than those starting a first biologic. Table 1 shows that the patients receiving rituximab tended to be older and with longer disease duration than those receiving other biologics.
A higher rate of infection was observed with tocilizumab compared with etanercept in both the adjusted and unadjusted models. Given the large sample size, this is unlikely to have occurred just by chance. It is possible that there was confounding but the result remained significant in a sensitivity analysis limiting to contemporary practice from 2010 onwards (HR 1.34, 95% CI 1.01 to 1.79) and a second sensitivity analysis excluding biologic-naive patients (table 2). These would suggest a true association. Our results were comparable with data from the German biologics register which found a higher relative risk of infection among tocilizumab users compared with those receiving anti-TNF therapy (relative risk 1.15).13 There is little directly comparative literature of infection risk between tocilizumab and other biologics. The ADACTA trial was an RCT comparing tocilizumab monotherapy with adalimumab monotherapy in RA.14 It found that tocilizumab had superior efficacy compared with adalimumab suggesting that it may be a more potent drug which could provide a biologically plausible link to a higher infection rate. In the ADACTA trial, no difference was observed in the rate of serious infection between the drugs but event numbers were small with just 13 SIs recorded throughout the entire study.
In the primary analysis, certolizumab pegol had a significantly lower incidence of SI than etanercept. This is in direct contradiction to the 2011 Cochrane review which found that certolizumab had a higher rate of infection.7 In that review, the incidence of infection with certolizumab pegol was approximately 3–4 times higher than other anti-TNF drugs. It would seem unusual for drugs acting on the same pathway with similar efficacy to have such drastically different infection risks. In the EXXELERATE study, a direct head to head clinical trial of certolizumab pegol versus adalimumab the rate of serious infection was the same with both drugs at 3% though event numbers were small.15 The Cochrane review was a network meta-analysis using indirect comparisons between biologics to estimate the relative risk of infection. Differences in how the control groups are treated, for example, different levels of glucocorticoid therapy as well as the crossover design of studies included can give misleading relative risks when comparing drugs between different studies.
A large number of patients in the certolizumab pegol cohort had never previously been on a biologic. In the sensitivity analysis limiting only to individuals who had failed at least one biologic, certolizumab pegol no longer had a favourable infection rate compared with etanercept. This suggests that unmeasured confounders may be responsible for the difference that was observed in the primary analysis. It is notable that etanercept entered the register in 2001 but certolizumab pegol recruitment did not commence until 10 years later in 2011.
A different pattern of infection was seen between the drugs. It was interesting to observe that a lower rate of sepsis was seen with the anti-TNF drugs compared with rituximab. Previous work from the German RABBIT register found that the risk of developing sepsis among individuals with SI and mortality from sepsis was lower with anti-TNF therapy compared with non-biologic DMARDs.16 This is perhaps not surprising as TNF is thought to be an important cytokine in the development of sepsis and clinical trials have been carried out to evaluate the use of TNF blockade in treating patients with severe sepsis.17 18 Many of the initial trials of anti-TNF in sepsis found no significant change in the mortality rates but they may have been underpowered. A recent meta-analysis has shown a small but significant reduction in mortality with anti-TNF among patients with sepsis.19 These clinical trials were looking at the benefit of giving a single dose of anti-TNF to patients who already had developed sepsis. It is possible that greater benefit would be seen in individuals who were already taking anti-TNF therapy when they developed an infection.
The all-cause mortality in the overall cohort was low at 0.84% per year but was significantly increased immediately following a serious infection. Over 10% of patients who suffered a serious infection died within 30 days of the event highlighting the significance of these events. Sepsis was a significant predictor of mortality.
Strengths
The large sample size, robust method of data capture and accurate coding of adverse events including SI is a strength of the BSRBR-RA and allowed comprehensive analysis of SI in biologic-treated patients. What sets this study apart from many others looking at the safety of biologics is our choice of etanercept as the comparator arm. Previous studies using registries have mostly compared the risk of starting a biologic with the risk of continuing current DMARDs in patients with severe disease. This is an increasingly irrelevant comparison as most clinicians faced with a patient who has not responded to DMARDs will opt to start a biologic. Cost and efficacy will have a big influence in drug decision but in those who are at high risk of infection, safety will also play an important role. It is therefore vital to have directly comparative studies.
Limitations
As the previously mentioned Cochrane review showed a varying infection risk with different biologics, clinicians may have channelled higher risk patients away from drugs that they perceive to have the greatest infection risk towards supposedly ‘safer’ drugs. We have adjusted for baseline variables that predict infection but there will always be a degree of unmeasured confounding that we cannot adjust for. This could help to explain why such a drastically different infection risk was seen with certolizumab pegol in our analysis and the 2011 Cochrane review.
Caution needs to be exercised when interpreting the relative risk of infection by organ class. This secondary analysis was performed on smaller numbers of events and is more prone to error from misclassifications than the primary analysis. Multiple comparisons were performed and as such the chance of finding statistically significant results by chance increases. In efficacy studies, one would normally adjust the p value when performing multiple comparisons to reduce the risk of false positives. However, in pharmacovigilance studies, one is more concerned about missing a potential safety signal and false negatives are the greater concern. We have therefore not adjusted the significance level despite performing multiple comparisons.
This study has identified differences in the incidence and patterns of SI between biologic drugs in a large RA cohort. For the majority of patients, biologic therapies remain a safe and efficacious treatment strategy. However, in a population of ‘high-risk’ individuals, differences in the relative risk of infection can have a significant impact on the absolute risk of SI. Recognising the subtleties in the differential infection risk profiles between drugs is a step towards personalised medicine and safer prescribing habits.
Acknowledgments
AIR was funded by a clinical fellowship from the NIHR Biomedical Research Centre at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. This manuscript is based on work previously presented at EULAR 2017 as a conference abstract.
References
Footnotes
Handling editor Josef S Smolen
Contributors All authors were involved in the design and statistical analysis of the study as well as manuscript drafting and gave approval to the final version.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests The BSR commissioned the BSRBR-RA as a UK-wide national project to investigate the safety of biological agents in routine medical practice. BSR receives restricted income from UK pharmaceutical companies, presently Abbvie, Celltrion, Hospira, Pfizer, UCB and Roche, and in the past Swedish Orphan Biovitrum and Merck. This income finances a wholly separate contract between the BSR and the University of Manchester. The pharmaceutical company funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript and decision to submit the manuscript for publication. KH has received honoraria from Pfizer and Abbvie (<US$10 000). JG has received honoraria for speaking or attending conferences from Pfizer, BMS, UCB and Celgene (<US$10 000).
Patient consent Not required.
Ethics approval The study was approved by the North-West Multicentre Research Ethics Committee (MREC 00/8/053, IRAS: 64202).
Provenance and peer review Not commissioned; externally peer reviewed.